
Abstract
Work-related musculoskeletal disorders affect a large percentage of diagnostic medical sonographers. Ultrasound transducer design has been identified as a major contributing factor to hand and wrist strains. The purpose of this study was to determine if the design of the ultrasound transducer affects the amount of pressure exerted by the hands of the sonographer to achieve a quality scan. The study also aimed to determine if the amount of pressure exerted on the transducer relates to the subjective pain level reported by the sonographer. The study found that the average maximum pressure and average force exerted was higher when scanning with a small transducer compared with a large transducer, and the thumb typically exerted a much greater pressure and force. Sonographers reported pain during the scan trials, as well as throughout their typical workdays, leisure pursuits, and daily activities.
Musculoskeletal disorders are one of the most common types of work-related illnesses and have been recognized as one of the leading causes of absence among working populations. Conditions that are caused or exacerbated by activities within the workplace are labeled as work-related musculoskeletal disorders (WRMSDs) and are characterized by pain and discomfort of tendons, muscles, and supporting structures of the body. 1 One area of the health care industry that has been specifically affected by the burden of WRMSDs is diagnostic medical sonography.
WRMSDs affect approximately 80% to 85% of sonographers; 40% describe their pain as severe, and 20% of these individuals lose their career as a result.2,3 Due to continuous advances in productivity demands, sonographers today have increased their daily patient load, spending more time scanning patients and less time resting between scans. 3 Unfortunately, these can be detrimental to the health and career of the sonographers. 2
Evidence suggests the high prevalence of WRMSDs in sonography is due to the awkward wrist positions, repetitive motions, static muscle contractions, and forceful manual exertions that sonographers must apply to obtain a quality image of the patient’s target organ. 2 Ultrasound transducer design has been identified as a major contributing factor to hand and wrist strains. 3 While scanning, the sonographer must apply continuous pressure to keep the transducer in contact with the patient’s body, which may be sustained for up to 90 minutes at a time. The pressure required to hold onto the transducer depends on the size and shape of the handle, as well as grip preference.
A patient’s body morphology also plays a role in hand and wrist strains among sonographers. 4 Over the past decade, there has been an increase in the number of obese patients scanned by sonographers. 4 Studies have shown that the more obese the patient, the more pressure must be exerted on the transducer and the abdomen to obtain a quality scan. 4
Bastian et al 2 measured grip pressure through force matching with a digital dynamometer. The study concluded that the larger the patient, the higher the estimated grip pressure. It was also found that estimated grip pressure did not differ between handedness. The findings are consistent with previous studies, which have suggested that both inexperienced and experienced sonographers could benefit from ambidextrous abilities without increasing risk factors for injury or decreasing scan quality during clinical practice.2,5 The Bastian et al study used force matching to determine grip pressure placed onto the transducer. Although there is some support for force matching, it was felt that a direct measurement would be the most accurate way to determine the pressure and force applied to the transducer. The present study sought to address this limitation by using a capacitive sensor mat placed directly on the handle of the transducer to measure pressure exerted while scanning. The purpose of this study was to determine if the design of the ultrasound transducer affects the amount of pressure exerted by the hands of the sonographer to achieve a quality scan. The study also attempted to determine if the amount of pressure exerted on the transducer relates to the subjective pain level reported by the sonographer.
Methods
A mixed-methods approach combining the simultaneous collection and interpretation of both qualitative and quantitative data was chosen, using a concurrent triangulation strategy (convergent parallel design) to merge the two sets of results into an overall interpretation. The quantitative and qualitative data were combined and compared to provide a comprehensive understanding of the association between the pressure and force exerted by sonographers while scanning and the physical pain perceived, as reported by comments made by sonographers before, during, and after scanning. The study was approved by the Institutional Human Research Review Committee as one of two partner studies completed simultaneously; the other study evaluated upper extremity kinematics (shoulder, elbow, and wrist joint angles) during kidney scans.
Participants and Sampling
The volunteer patient was a 23-year-old white man, measuring six feet, three and a half inches tall and weighing 254 pounds. With a body mass index (BMI) of 31.3, the patient would be categorized as obese by the World Health Organization. 6 The same volunteer was scanned by each of the three sonographers. The three sonographer participants were all female, right-hand dominant general sonographers, and they had been practicing diagnostic medical sonography for at least three years. All three sonographers worked full time; however, one sonographer worked in an outpatient setting, and the other two worked in acute settings. Institutionally approved informed consent forms were signed by the patient volunteer and all three sonographers prior to initiating the study.
Instrumentation and Materials
Ultrasound transducer
Two different ultrasound transducers were used to determine the relationship between handle size, hand pressure required to produce a quality scan, and subjective pain experienced after scanning. The two transducer designs were selected after consultation with an experienced sonographer and professor of diagnostic ultrasonography and based on their widespread use in abdominal sonography. The ultrasound machine used was a Philips iU22; the transducers utilized in this study were a large C5-1 and a small S5-1 (Philips Medical, Bothel, WA). (Figure 1).

Photograph of the C5-1 and S5-1 transducers used with a centimeter scale indicating transducer sizes.
Pressure sensor
The pressure required to produce a quality scan was measured via a capacitive sensor mat wrapped around the handle of the transducer. The Novel Pliance-X capacitive sensor (Novel Electronics, St Paul, Minnesota) is a dynamic pressure distribution measuring system that is designed for a variety of applications, including medical, ergonomic, and biomechanical testing scenarios (Figure 2). 7 The Pliance-X sensor was chosen due to its size and flexibility as well as its ability to produce a dynamic, high-resolution map of pressure distribution of the fingers, thumb, and palm during grip. 8 The sensor provides a sensitivity of ±0.25 N/cm2 and a range of ±0.5 to 60 N/cm2, with a sampling rate of 60 Hz. 9 The Pliance-X sensor mat has been determined to be a valid method to measure grip force, with greater validity and reliability than other grip force measuring techniques.8,9 The Pliance Online Program was used to collect and display the data captured by the sensor mat after calibration, recording the parameters of force (N), peak pressure (kPa), mean pressure (kPa), and contact area (cm2). 7
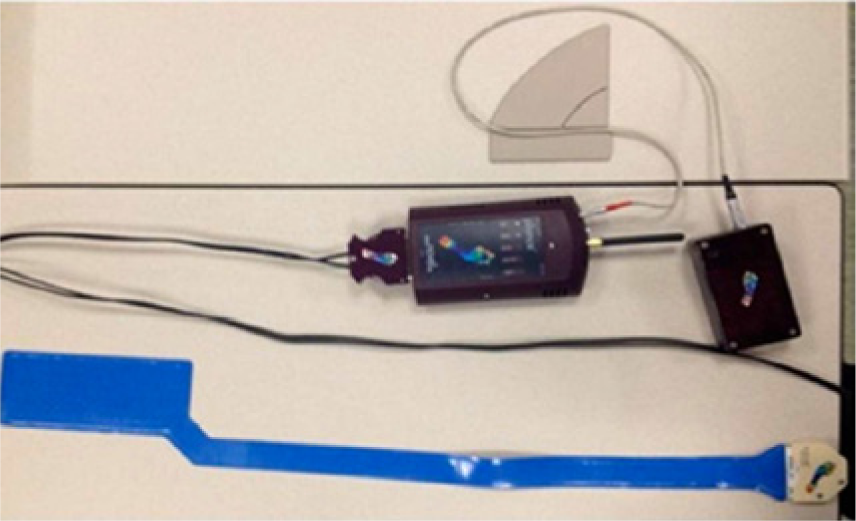
Photograph of the Novel Pliance-X capacitive sensor with Bluetooth device.
Questionnaire
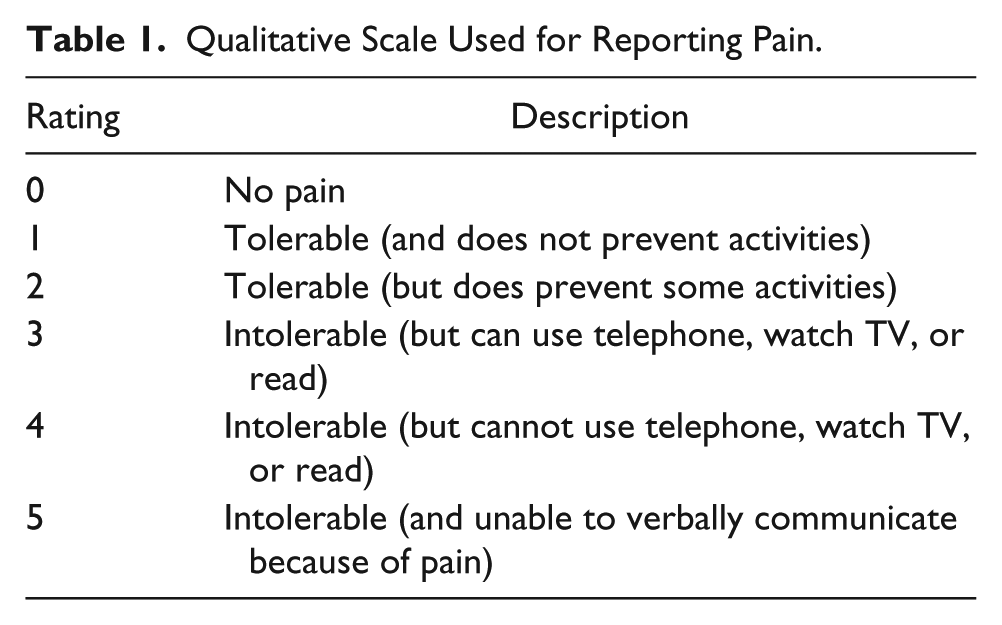
A pre- and postscan questionnaire was administered to the sonographers. The prescan questionnaire collected current information regarding demographics, grip and pinch strength, pain experienced, limitations in daily activities, and impact on work performance. A similar postscan questionnaire collected information regarding pain experienced and transducer design preference. To record the subjective descriptions of pain, both the pre- and postscan questionnaires used a body pain diagram in which the sonographers indicated the different locations of their pain by shading the corresponding areas of the diagram. The severity of pain experiences was determined using the Functional Pain Scale (FPS), with pain rated on a scale from 0 (no pain) to 5 (intolerable, unable to verbally communicate) (Table 1). 10
Qualitative Scale Used for Reporting Pain.
Procedures
After completing informed consent, each sonographer filled out the prescan questionnaire and demographic form. The sonographers’ baseline grip and pinch strengths were measured, including measurements of lateral pinch (between the radial side of the index digit and volar tip of the thumb), tip pinch (between the volar tip of the thumb and index digit), and three-jaw chuck pinch (between the volar thumb and the volar fingertips of the index and middle digits). These values were collected using a calibrated Jamar hand dynamometer and Baseline pinch gauge (Patterson Medical, Bolingbrook, IL) following the American Society of Hand Therapists Clinical Recommendations. 11 Next, the Novel Pliance-X sensor mat was secured to the larger C5-1 transducer using Micropore medical tape (3M, St. Paul, MN). (Figure 3). The hand sensor was mapped based on the specific grip of each individual sonographer. To accomplish this, a series of data recordings were collected to determine baseline force and pressure that each digit applied when the sensor was wrapped and taped around the transducer.

Photograph of the large transducer (C5-1) wrapped in the Novel Pliance-X capacitive sensor.
With the Pliance program running, each sonographer scanned the volunteer patient’s right and left kidneys in the longitudinal plane with the C5-1 transducer using her dominant (right) hand. The sonographers conducted four longitudinal scans of each kidney that were determined to be of diagnostic quality by an experienced sonographer and professor of diagnostic ultrasonography. Qualitative comments made by the sonographers before, during, and after scans were recorded throughout the study by the researchers. After completing the right and left kidney scans with the large transducer, the Novel Pliance-X sensor was secured to the smaller S5-1 transducer. At this time, the sonographers had a 15- to 30-minute recovery period, determined adequate to regain hand steadiness after heavy lifting. 12 Following the rest period, the sonographers performed the same four longitudinal kidney scans using the small transducer. After all the scans were complete, the sonographer participants completed a postscan questionnaire.
The data analysis for this study was divided into two parts. The quantitative data were gathered from the Novel Pliance-X sensor system and the FPS completed by the sonographers, while the qualitative data were gathered from the comments made during scanning and from the pre- and postscan questionnaires. The Pliance program provided values for average force, maximum force, and maximum pressure throughout the duration of each scan. Average (mean) values were then calculated from these data across time for each scan. These descriptive statistics were organized into tables for further review. Concurrently, qualitative data were compiled from the responses described above. Triangulation was used to promote accuracy when analyzing the qualitative data to determine the themes and subthemes to promote validity and reliability of the data analysis. Trustworthiness of the qualitative data was established through crosschecking of the data obtained during the study. Intercoder agreement was established and codes were documented to ensure accurate communication among researchers. These data were then combined with quantitative data following the mixed-methods approach to the study. 13
Results
Baseline Grip and Pinch Strength
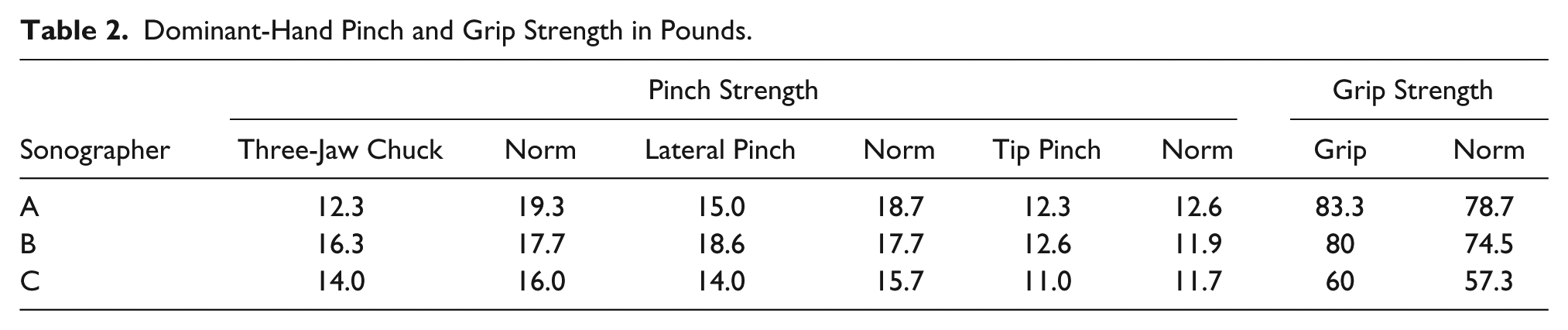
The grip and pinch strength measurements of each sonographer were compared with the age-related norms established by Mathiowetz et al, 14 as displayed in Table 2. Two of the three sonographers displayed pinch strength within one standard deviation of the age-related norm across all prehensive grasping patterns. Sonographer A, the only sonographer experiencing pain before the scan began, exhibited decreased strength of more than one standard deviation from the mean during the three-jaw chuck and lateral pinch strength measurements. All three sonographers had greater grip strength than the corresponding age-related norms; however, all values were within one standard deviation of the mean.
Dominant-Hand Pinch and Grip Strength in Pounds.
Pressure and Force Exerted While Scanning
Table 3 compares the full sensor pressures and forces exerted based on the size of the transducer. The maximum pressure and maximum force are the highest recorded values during the scan. The average force is the average of each recorded value collected during the scan. The results are displayed as maximum pressure and maximum force for each scan completed by each sonographer. All sonographers exerted a higher maximum force while scanning the right kidney with the small transducer versus scanning with the large transducer, and two of the three sonographers exerted a higher maximum force while scanning the left kidney with the small transducer versus the large transducer. When comparing right versus left kidney scans, the data varied without any consistency in pressure or force exerted for all three sonographers.
Maximum and Average Pressure and Force Based on Transducer Size.

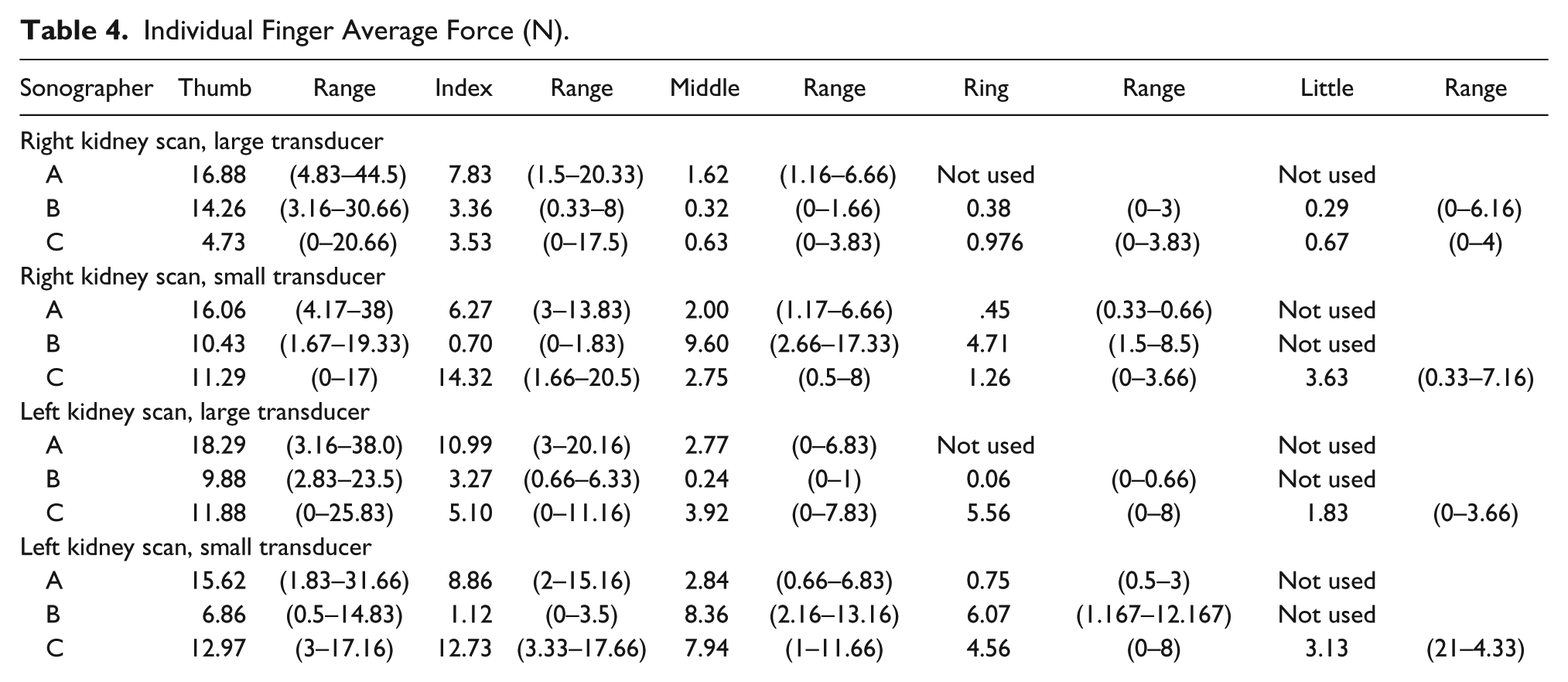
There was a variation between the force and pressure values obtained from each sonographer’s trial; however, the researchers noted that the thumb produced the greatest average force across the sonographers and trials, with the exception of sonographer C when scanning the right kidney with the small transducer and sonographer B when scanning the left kidney with the small transducer. During those trials, sonographer C produced the greatest average force with her index finger (14.32 N), while sonographer B produced the greatest force with her middle finger (8.36 N) (Table 4). Evaluating specifically the pressure exerted while scanning, the thumb produced the greatest maximum pressure (range 0–190 kPa) for the sonographers across transducer size and type of kidney scan, except for a single instance for sonographer B when scanning the left kidney with the small transducer. For that particular scan, the ring finger produced the greatest maximum pressure (76.67 kPa) (Table 5).
Individual Finger Average Force (N).
Individual Finger Maximum Pressure (kPa).
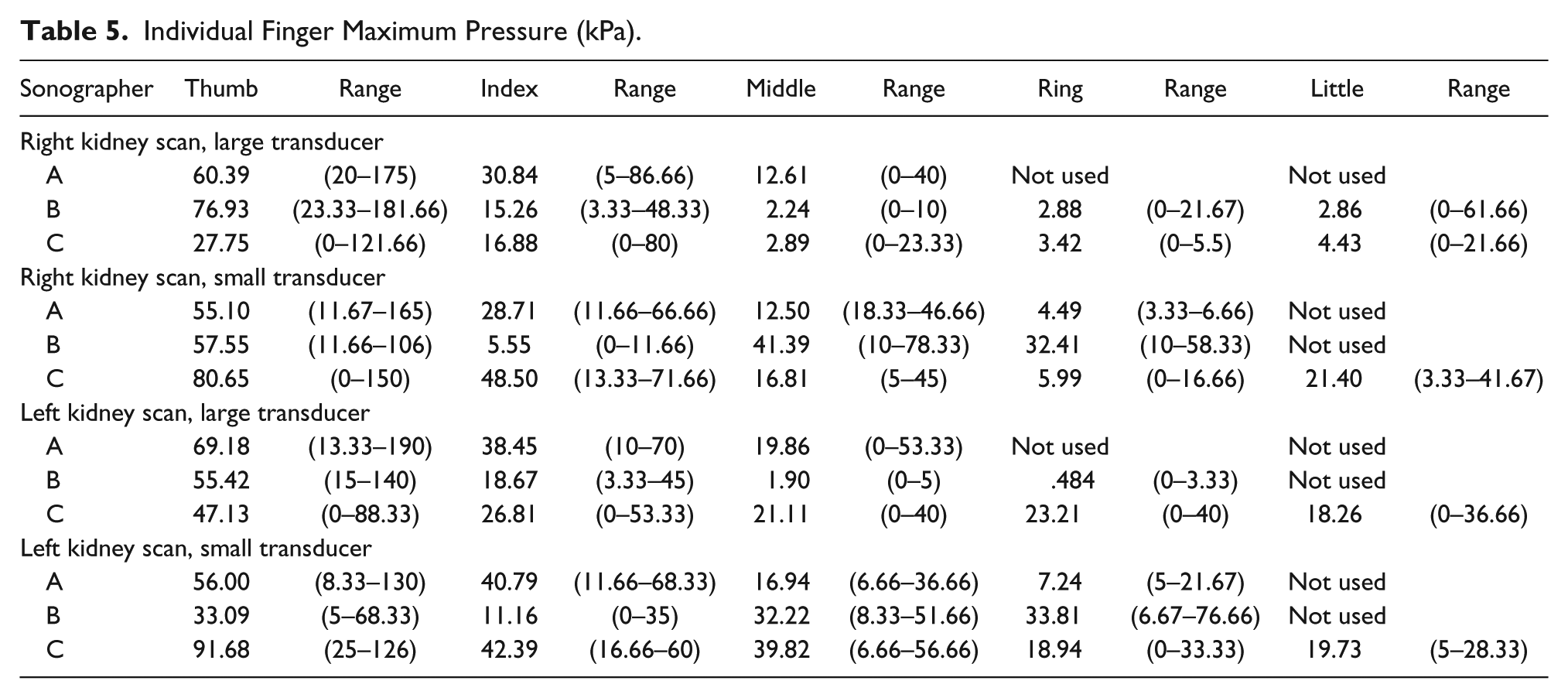
Table 3 compares the overall maximum pressure and maximum force and the average force between the large and small transducers for all kidney scans. These data indicate that the maximum pressure and average force exerted trended higher when scanning with the small transducer compared with the large transducer.
Level of Pain
The subjective level of pain rated using the FPS varied for each sonographer. While scanning, sonographer C rated pain at level 1, sonographer B rated pain at level 2, and sonographer A rated pain at level 4. The perceptions of pain increased after the sonographers scanned the volunteer patient in all cases except for sonographer B, who indicated no change in pain. There were no marked differences between sonographers with regard to scan quality, posture, force, pressure, or body size. All sonographers also reported an increase in pain while performing scans in their workplace and during leisure activities. Furthermore, all sonographers, except for sonographer B, indicated increased pain during activities of daily living (ADLs). All sonographers reported an increase in pain during work tasks and leisure activities such as yoga, typing, and swimming (Table 6).
Demographics and Perceived Level of Pain During Various Occupations.
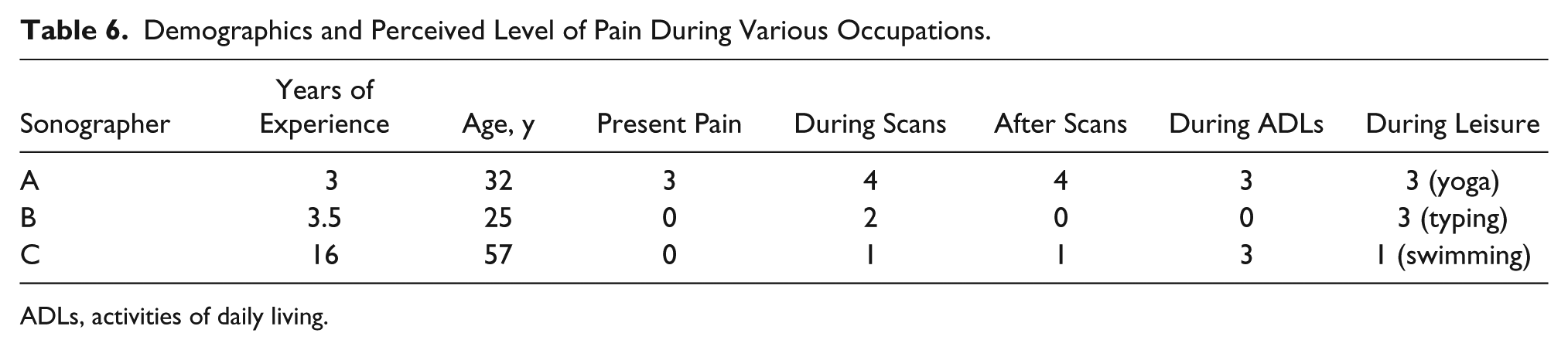
ADLs, activities of daily living.
Qualitative Results
When analyzing the pre- and postscan questionnaires and field note comments, two main themes arose: pain and scanning experience.
Theme 1: pain
All three sonographers in this study reported some type and level of pain. Three subthemes emerged when coding was performed on the pain data and included (1) pain while scanning, (2) varied physical locations of the pain, and (3) the type of activity inducing pain while performing regular functions outside of work. Pain was most commonly reported in areas of the neck, shoulder, and back; however, one sonographer reported pain in the legs. Pain occurred while performing scans and also in ADLs, such as dressing and gripping objects, and in leisure activities, such as yoga and swimming.
Theme 2: scanning experience
The scanning experience was defined as the time spent with the transducer in contact with the patient volunteer while images of internal organs were being collected. This included the types of patients, the interactions with the patients, and the types of transducers used. The three subthemes collected were (1) challenging patients, (2) sonographer behavior (a technique or method used during scanning), and (3) transducer preference.
Overall, the three sonographers had similar scanning experiences. All three characterized challenging patients as immobile, obese, and pregnant. The sonographers reported moving to accommodate patients unable to move when requested to obtain better quality scans. Furthermore, it was found that adaptive equipment, which may aid in reducing pain, was not used in the sonographers’ typical scanning experiences.
The three sonographers for various reasons reported a preference for one of the transducers. The sonographers often preferred the larger transducer due to comfort. Sonographer B stated, “The larger transducer had a better grip than the smaller transducer.” Two additional statements made by the sonographers regarding handle preference were by sonographer A (“I rarely use the small transducer”) and by sonographer C (“I’m not sure how to hold the small transducer”). Many of the responses were similar; however, sonographer A, who reported more pain and had a weaker pinch strength overall, stated that she felt that the smaller transducer was easier to angle when trying to obtain an image through narrow spaces, such as when scanning in between the ribs.
Comparison of Quantitative and Qualitative Results
The qualitative and quantitative data are correlated in many ways. The researchers used the concurrent procedures method to converge the qualitative and quantitative data for analysis. Triangulation was used during this analysis to facilitate further validity. 13 Sonographer B had the highest baseline tip, lateral, and three-jaw chuck pinch strength of the three sonographers and also indicated that she did not feel any pain while scanning the volunteer patient. She reported that typically she only feels pain in her left wrist due to simultaneous keyboard data entry (left hand) while scanning (right, dominant hand). The researchers speculate that her lower pain perception may be due to her higher pinch strength as measured at baseline.
Sonographer A had the highest overall grip strength and exerted the highest maximum pressure on the sensor as a whole during almost every scan, with the exceptions of sonographer B, who exerted a higher pressure when scanning the right kidney with the large transducer, and sonographer C, who exerted a higher pressure when scanning the right kidney with the small transducer. Sonographer A had the highest overall force for all scans of the right kidney and reported the most pain while scanning. The researchers question whether her higher exertion while scanning could potentially be causing her more pain, possibly due to higher co-contraction of upper extremity musculature. She also reported a previous injury to her back during a motor vehicle accident, which could be causing her to compensate and adjust her posture during the scanning.
In this study, the maximum pressure and average force exerted was higher when scanning with the small transducer compared with the large transducer. The recorded pressure and force of each of the individual digits showed that, on average, the thumb typically exerted much greater pressure and force on the transducer than any of the other digits. Furthermore, the sonographers reported pain during the scan trials, as well as throughout their typical workdays, leisure pursuits, and ADLs. All three sonographers reported that obese, pregnant, and immobile patients often create a difficult work environment. This study is unique in that it explored the pressure applied directly to the transducer grip throughout scanning rather than generalizing the results through force matching on a dynamometer.
Discussion
Past studies have reported an increase in WRMSDs and upper extremity pain within the field of sonography. However, research that takes into account the actual pressure and force that the hand places on the transducer during scanning has been lacking. This study used the Novel Pliance-X hand sensor program, which measured the pressure and force applied directly to the transducer grip during a simulated renal scan to determine how applied force and transducer design affect the experience of sonographers during and after scanning.
Past research has concluded that the specific work tasks of scanning contribute to 80% to 81% of general sonographers experiencing musculoskeletal pain or discomfort in the upper body.15,16 It was surprising to the researchers that the sonographers in this study did not report any pain in the fingers or thumb, especially in relation to the large amount of force produced by the thumb during scanning. The force applied to ultrasound transducers during scans did differ based on transducer grip design, and the differences varied greatly (large transducer, 37.09 N vs small transducer, 54.33 N). The sonographers in this study had varied opinions regarding transducer preference, each preferring the large or small transducer for different reasons, including the qualitative results of comfort, familiarity, and grip.
Overall, the results of this study are consistent with previous research. The study found that the amount of pressure exerted by the hand increased with the small handle transducer compared with the large one, which is consistent with Sancho-Bru et al, 17 who determined the optimal diameter for a cylindrical-shaped handle to be 33 mm as it requires the least amount of grip force. Furthermore, the participants of the present study also reported pain during and after scanning at work, especially when scanning obese or pregnant patients who require more pressure to be exerted on the abdomen to retrieve a quality scan, which is consistent with the findings of Brown and Baker 4 and Evans et al. 18
The present study’s questionnaire results were mixed, showing preference for both sizes of transducers for varied reasons. The large transducer was preferred for ergonomic reasons as it provided more comfort with a more familiar and natural grip than the small transducer; however, the small transducer potentially affected study quality as it allowed for better angles to obtain images through limiting spaces, such as the ribs, when conducting a renal scan.
For all three participants, the maximum pressure exerted while scanning was produced by the thumb across both transducer sizes and across right and left kidney scans, with one exception. Sonographer B exerted more pressure on average with her ring finger while scanning the left kidney with the small transducer. The sonographers mainly used the index, middle, and ring fingers. The small (fifth) finger was seldom used. The average force and pressure produced by the thumb was typically greater than the average force and pressure of the other fingers combined. One possible reason why the thumb produced the highest maximum pressure is that, during pinch and grasp, the thumb provides intrinsic stability and strength to resist the forces applied by the other fingers involved to hold onto an object. 19 The researchers were surprised that thumb pain was not mentioned by the subjects. Pain was more commonly reported in the neck, shoulder, and back.
Limitations
The limitations of the study include the participant sample size, the atypical scanning environment, and the addition of the Novel Pliance-X sensor. This study used a sample of convenience that was not large enough to generalize (N = 3). Hand size, sonographer age, previous injury, order of transducers used, and individual scanning preferences (i.e., sitting vs standing and/or altering the patient vs altering the sonographer’s posture to retrieve scans) were variables that were not addressed that may have an influence on the pressure exerted in this study and the pain reported. It would also be beneficial to explore this research question further in a nonobese population and to evaluate pain level after each scan.
Future Research
The study offers a supplement to previous evidence for the impact of transducer design and scanning procedure on WRMSDs and pain experienced by sonographers. Future research should focus on determining correlations between the angles of the arm, the contractions of the muscles, and the pressure exerted by sonographers while scanning. It may be beneficial to correlate pain experienced and pressure exerted in a larger sample of sonographers to explore whether there is a relationship between extreme thumb pressure and upper extremity–related pain and injury. The results of this study also require further validation, including a larger sample that takes into account the naturalistic work environment and workload of sonographers.
Footnotes
Acknowledgements
We thank Lynn Carlton, MSRS, RDMS, RT(R)(M), and Rick Carlton, MS, RT(R)(CV), FAEIRS, for their assistance with planning this project, recruiting sonographers, and providing professional input into the field of sonography.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.