
Abstract
Objective:
Pregnancy can induce the slowing of blood flow in the lower extremity veins and associated complications such as varicose veins. The objective of this study was to report the hemodynamic alterations in uncomplicated pregnancies during second and third trimesters using spectral Doppler. The specific aim was to compare the venous diameter and mean flow velocities of maternal common femoral veins (CFVs) during second and third trimesters of pregnancy. This was designed to assess the extent of pregnancy-induced hemodynamic changes as well as to establish a normative range of these values.
Materials and Methods:
This cohort study was conducted with 230 women during second and third trimesters of pregnancy. Grayscale sonography and spectral Doppler were used to record the diameter and mean flow velocity of maternal CFVs bilaterally. An independent sample t test was performed for the comparison of these between women with second and third trimesters of pregnancy. Statistical significance was set a P ≤ .05, a priori.
Results:
There was significant dilatation and a corresponding decrease in mean blood flow velocities in the CFVs in the participants in their third trimester compared with the second trimester of pregnancy.
Conclusion:
In this large cohort of participants, the CFV demonstrated statistically significant distension and slowing of blood flow with the advancement of their pregnancies.
The venous system acts as the dynamic reservoir for 60% to 70% of a human’s total blood volume. 1 It undergoes adaptations under the influence of pregnancy-related hormones, in a similar manner as the other components of the cardiovascular system. These have been described as alterations in distensibility and compliance of the veins. 2 Multiple studies suggest increased diameter of the lower extremity veins reaching maximum diameter, as patients’ pregnancies come to term.3,4 In addition to the hormonal changes, mechanical factors (e.g., the gravid uterus and position of fetal head in the pelvis), increased plasma volume, and functional changes in smooth muscle tone can be contributing factors toward increased distensibility of veins in the lower limbs.3 –8 The decreasing velocity of blood in these vessels has also been observed by a few researchers who reported marked changes toward the end of pregnancy.9 –12 Venous dilatation and the slowing of blood flow velocity, due to pregnancy-associated hypercoagulability, can act as predisposing factors for the development of varicose veins and venous thrombosis.9,11,13
Sonography along with spectral Doppler can act as a valuable diagnostic tool for non-invasive assessment of the lower extremity venous hemodynamics. There has been research investigating the hemodynamic alterations, within the venous system of lower limbs, of healthy pregnant females; however, the studies were older and had a small sample size.8 –10,13,14 This present study was designed to fill out this gap in the literature and provide updated information. To that end, the objective was to investigate the common femoral vein (CFV), at the level of inguinal ligament during the second and third trimesters of healthy and asymptomatic pregnant volunteers and look for changes in the vein’s diameter and flow velocity, utilizing grayscale sonography and spectral Doppler. Spectral Doppler can be easily performed at the conclusion of a routine antenatal obstetrical sonogram, without further exposure of the fetus. A knowledge of the range of changes that occur in the CFV diameter and flow velocities could provide an alert to obstetricians and other providers in the identification of pregnancy-related venous complications.
Materials and Methods
Participation Criteria
This cohort study was performed on approval from the local Institutional Research and Ethics committee. A total of 230 female participants were enrolled in the study, after acquiring written informed consent. There were 115 participants divided into both the second and third trimesters (14–40 weeks) of pregnancy. All these pregnancies were single, uncomplicated, and the participants had no complaints or clinical findings of lower limb venous insufficiency. The participants were all confirmed to be non-hypertensive and non-diabetic, so as to avoid hemodynamic changes related to these conditions.
Duplex Sonographic Imaging
All the sonographic examinations were completed using a Xario 500 (Toshiba, Tochigi, Japan) ultrasound equipment system and a 7 to 12 MHz linear transducer. The CFV was located at the level of inguinal ligament, medial to the common femoral artery. A compression technique was applied as a first step to exclude the presence of venous thrombus. Anteroposterior venous diameter was then measured in both transverse and longitudinal scanning planes and using a leading-edge technique (See Figure 1). This was done by placing the transducer gently in order to avoid compression of the vein. The average of these recordings was recorded as the representative value. The insonation angle between the Doppler beam and blood flow was kept between 55° and 59° according to patient’s vascular anatomy. The cursor sample volume was positioned longitudinally, in the middle of the vein, and the mean flow velocity values were measured (see Figure 2). All the recordings were done with the patients in dorsal decubitus position, during normal quiet breathing, by a senior sonologist (B.S.) having more than 15 years of experience. The velocity measurements were recorded twice, and the average of those measures was retained. The same imaging and measurement procedure was followed on the opposite side.
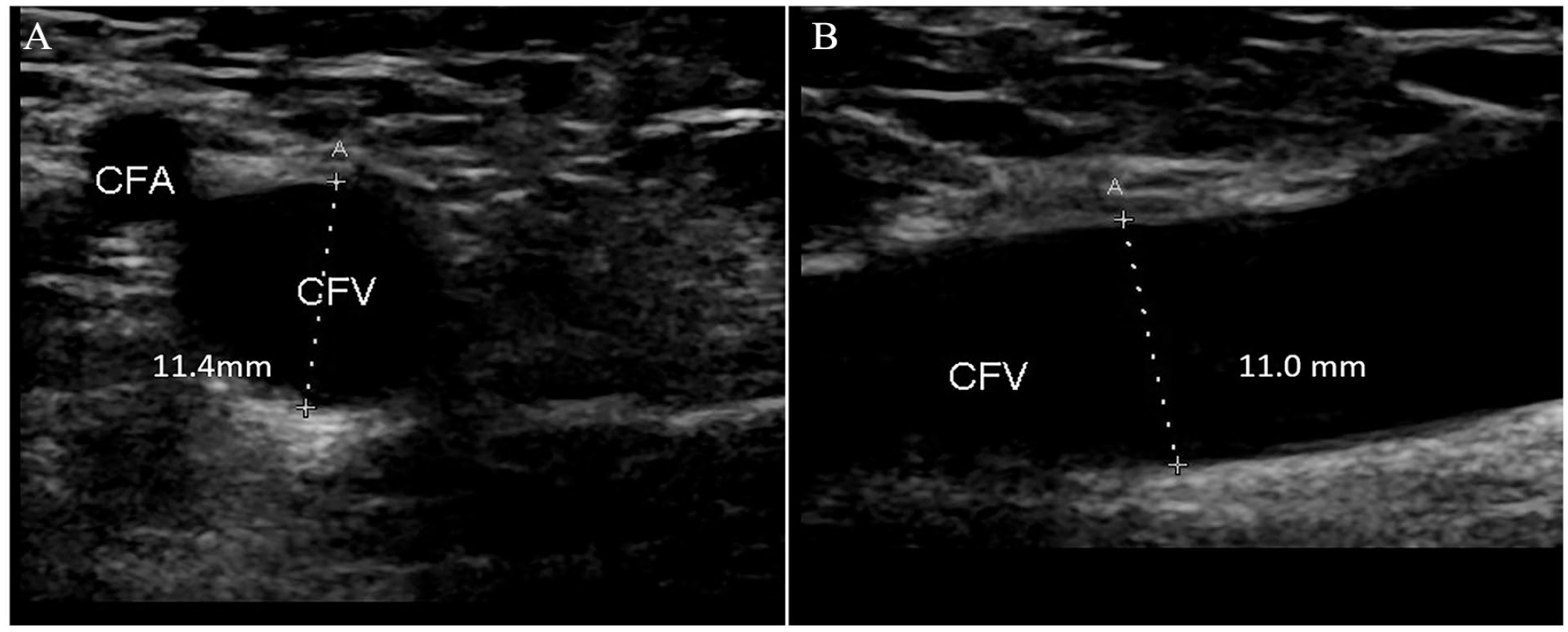
The anteroposterior diameter of common femoral vein was measured in both the transverse (A) and sagittal scan planes (B), using leading-edge method. CFV, common femoral vein.
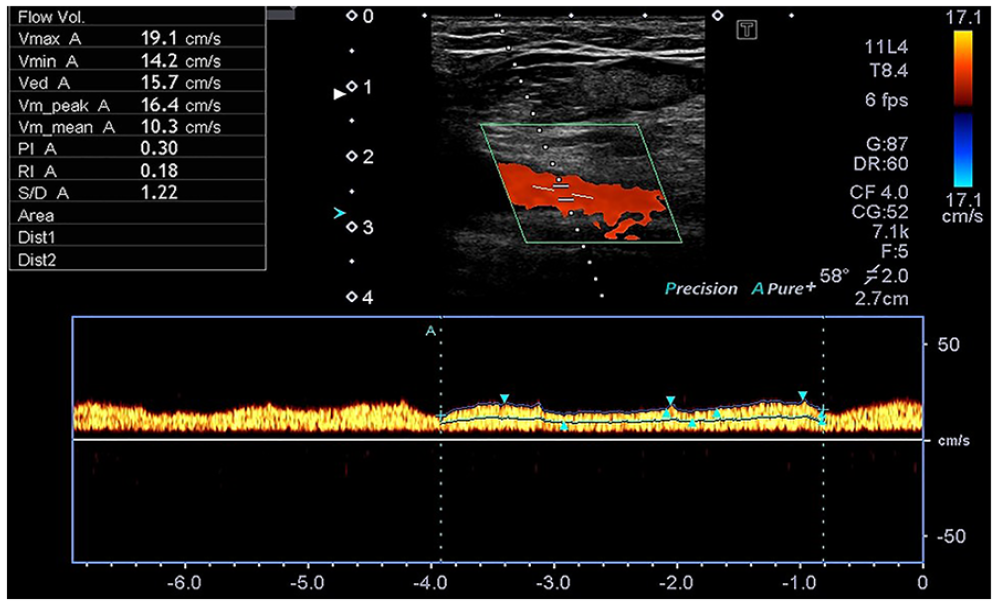
The duplex image shows how the cursor sample volume was positioned longitudinally, in the middle of the vein, to record mean blood flow velocities, in common femoral veins.
Statistical Analysis
Venous diameters and mean flow velocities in the left and right CFVs were compared among second and third trimester pregnant participants, using independent sample t test. A regression analysis was also performed between these values and gestational age (weeks). A comparison between right and left venous diameters and mean velocities were also performed using paired-sample t test. The statistical significance was set as P ≤ .05, a priori.
Results
A total of 230 women were examined as part of this cohort study. The age range for this cohort was 18 to 40 years and the mean age was 26 ± SD 4.54. In this cohort, none of the patients showed any evidence of thrombus formation. Monophasic flow pattern was recorded across all the patients in this cohort. There was significant vessel dilatation (P = .0001 and .0003) and a corresponding decrease in mean blood flow velocities (P = .0042 and .0011) in the left and right CFV, respectively, in participants in their third trimester compared with those in the second trimester, based on independent sample t test (see Table 1 and Figure 3). A regression analysis (see Figure 4) showed significant positive and negative correlation, respectively, with the CFV dilatation (P = .0001 bilaterally) and mean blood flow velocities (P = .0008 and .001) on left and right side, respectively.
Comparison of the CFV Diameters and Mean Flow Velocities Between Women With Second and Third Trimesters of Pregnancy.
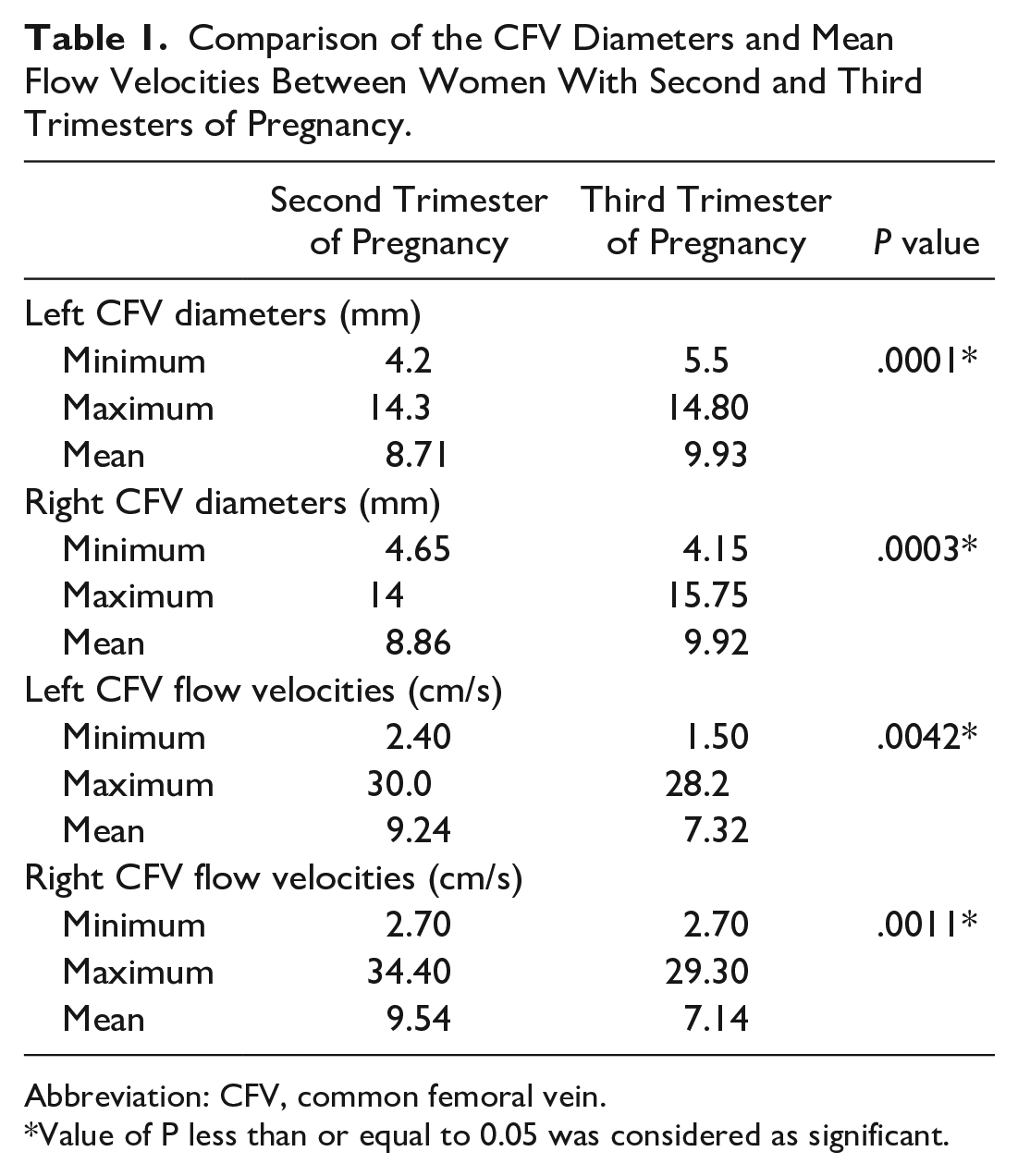
Abbreviation: CFV, common femoral vein.
Value of P less than or equal to 0.05 was considered as significant.
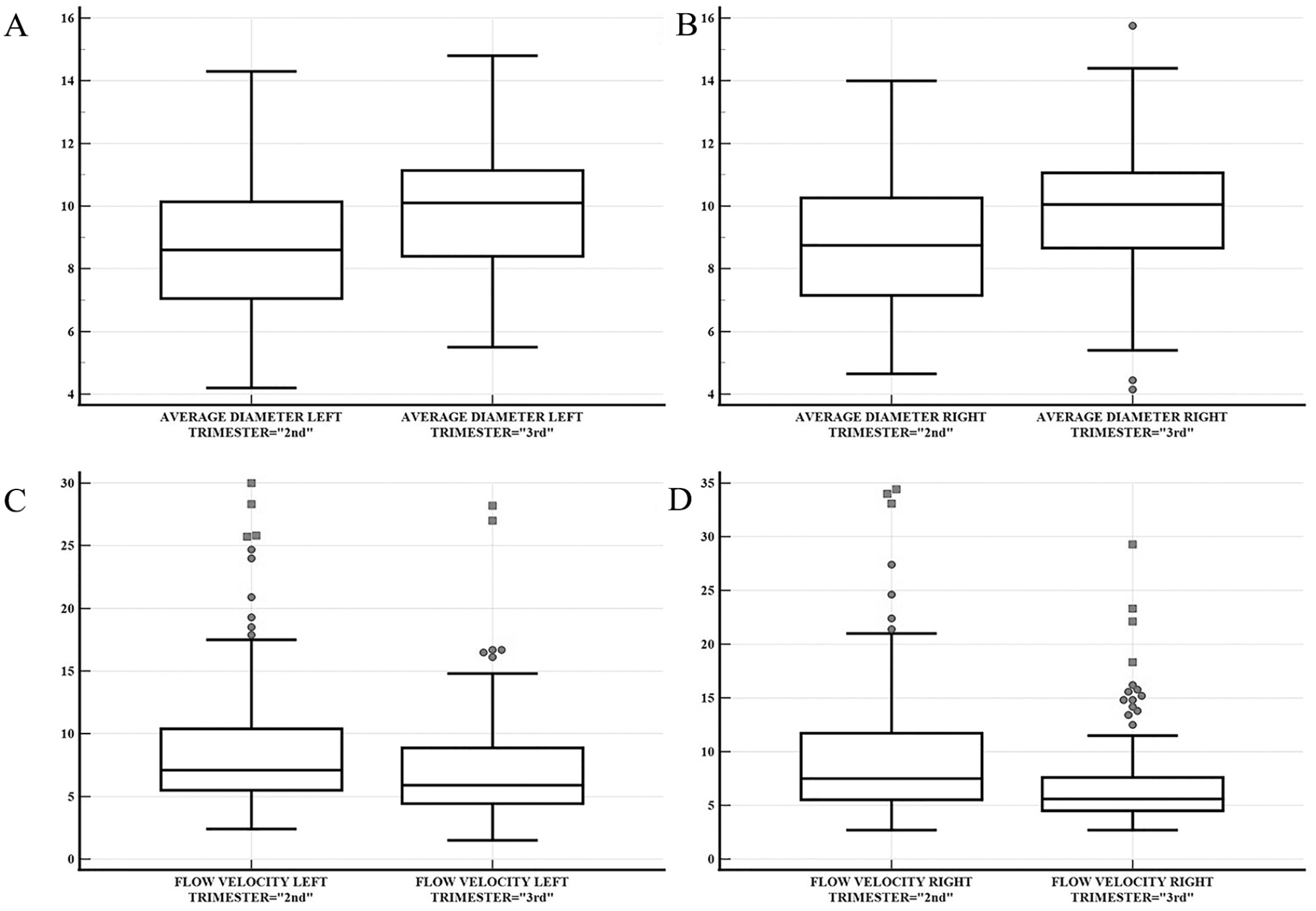
A box plot and whisker representation of comparison of common femoral vein average diameters (A and B) and mean flow velocity values (C and D), on left and right sides, respectively.
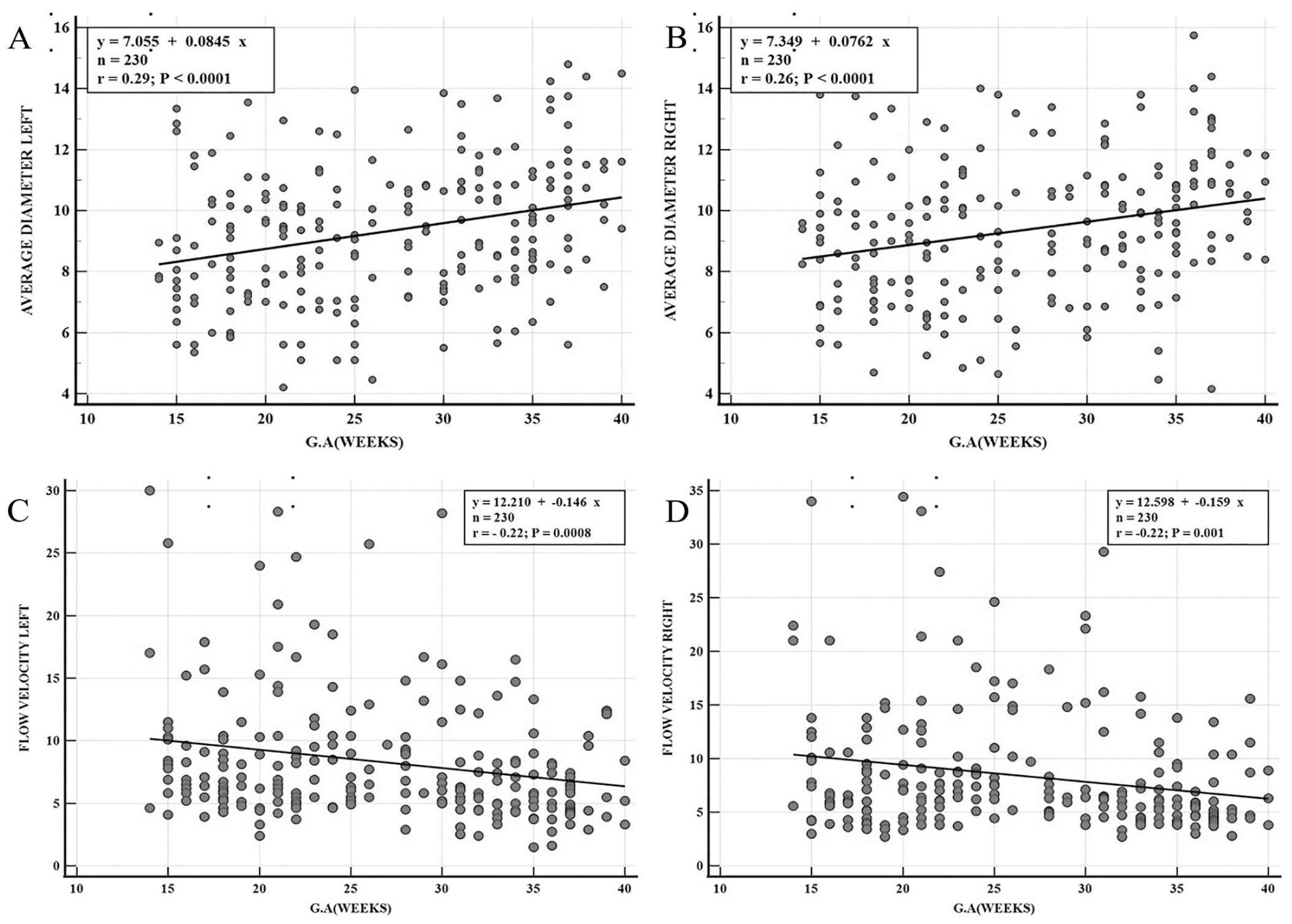
A graphical representation of correlation of common femoral vein average diameters (A and B) and mean flow velocity values (C and D) with advancing gestational age (weeks), on left and right sides, respectively.
Discussion
The CFV is a major lower extremity vessel, with a normal diameter of 11.22 mm and a mean flow velocity of 14.58 cm/s, in non-pregnant women. 15 There have been a few studies reporting the flow changes in the CFV along with the other veins in superficial and deep veins of the lower limb.10,13,14 However, none of these studies reported variations in both diameter and blood flow velocities in a large sample of patients. A longitudinal study was conducted by Sparey et al. 5 on 43 women from the 12th week of pregnancy until 6 weeks postpartum. The study reported significant dilatation in all leg veins, which returned to normal on the right side but not on the left side, during their study period. They, however, did not report exact measurements of the venous diameter, coupled with gestational age. Cordts and Gawley 6 noted mean CFV diameters during first trimester, 0.99 ± 0.25 cm and could increase up to 1.21 ± 0.25 cm in third trimester, based on six normal pregnant participants. Gardenghi et al. 14 also reported lower extremity venous dilatation in 20 pregnant women who did not have any clinical features of venous insufficiency. The latter reported the left and right CFV diameter range as 9.5 to 17.8 mm and 10.0 to 17.0 mm, respectively, in the second and 10.4 to 19.0 mm and 11.1 to 17.6 mm in the third trimesters. A similar study from Goulart et al. 16 reported a dilated CFV in primigravidae compared with non-pregnant women, even in the absence of any apparent venous insufficiency. They found the average diameter of CFV as 12.72 ± 2.27 mm during 22 to 36 weeks of gestation. Calderwood et al. 17 also noted progressively increased diameters of CFV while following pregnant women through their pregnancies. The maximum diameter was observed at 39 to 41 weeks, with a change from 8.11 mm at 15 weeks to 11.52 mm at 39 to 41 weeks. These studies reported values that, while slightly different from each other, were generally higher than the ones we found in the present study, except for the third trimester values reported by Cordts and Gawley, 6 which were lower than those found in the present study. The reason might be due to the ethnic differences in the studied population as have already been reported in the literature. 15 All of these previous studies, however, consistently reported significant dilatation of the CFV throughout pregnancy.
In addition to the diameters, the current study measured the mean flow velocities in this cohort’s CFV. Significantly decreased flow velocities in the present study and the advancement of gestational age matches the findings of Ropacka-Lesiak et al. 9 and Macklon et al. 18 The flow velocity measurements in these studies, however, were not in agreement with each other or with the present study. The earlier study stated much higher flow velocities (22.1, 21.2, and 19.8 cm/s in right CFV while 22.6, 20.6, and 18.7 cm/s in left CFV during first, second, and third trimesters, respectively) throughout the pregnancy. The latter study found a more profound decline in the velocities dropping to as low as 4.5 cm/s on right and 4.9 cm/s on the left. Ropacka-Lesiak et al., 9 however, did not propose any cause for this discrepancy in velocities.
Moreover, these changes have been described as more marked on the left side5,9,18 and even persisting longer in the postpartum period. 5 In the present study cohort, these changes were noted to be slightly increased on the left side, although the changes were significant in both right and left CFVs. The exact cause of this phenomenon remains unknown; however, it is believed to be linked to the compression of the left iliac vein by the overlying right iliac artery. This compression may explain why left-sided deep venous system thrombosis is more frequently observed than its right-sided counterpart, both in non-pregnant and pregnant individuals, with even a higher likelihood of left-sided involvement during pregnancy. 18
Dilatation of veins results in the release of tissue plasminogen activator into the venous lumen. 5 Moreover, venous distension causes endothelial damage leading to exposure of subendothelial collagen to the venous blood. This triggers the activation of the extrinsic pathway of coagulation. Among the affected veins, the CFV exhibits the most significant changes in both diameter and flow velocity. 8 Consequently, this combination of stasis and increased coagulability renders the CFV highly susceptible to the development of thrombosis. It has also been observed in the literature that the iliofemoral segment of the deep venous system is the most favorable site for thrombus formation in pregnant women in contrast to the non-pregnant state, where soleal sinuses of the calf are the site for the thrombus formation initiation.9,18,19 The choice of this vein for evaluation of venous system using spectral Doppler seems very reasonable for screening pregnancy-related changes at the early stage of venous insufficiency. Second, evaluation of the entire venous system of the lower limb is not practical as prolonged lying down in the supine position might cause inferior vena cava syndrome and due to difficulty of positioning required for adequate visualization of all the veins of lower limb.
Limitations
The major limitation with this study was the research design and the convenient sample of pregnant volunteers. Given the threats to internal and external validity, these results cannot be generalized. An added limitation was the failure to include females in post-partum period, so that the reversal of changes in CFVs could also be investigated. The inclusion of these results would have been more meaningful and highly impactful. A strength of the current study was a larger sample size compared with the previously published studies. Adding this additional evidence may provide more accurate mean values of CFV diameters as well as flow velocities in both second and third trimesters of pregnancy.
Conclusion
This cohort study’s findings have added to evidence that during pregnancy, the CFV likely undergoes statistically significant dilatation, along with a decrease in mean blood flow velocities. Importantly, this research establishes a possible baseline set of values for these natural hemodynamic changes occurring in the lower limb venous system, during pregnancy, in the absence of clinical signs of venous insufficiency. These reference values may be clinically valuable for assessing the extent of hemodynamic abnormalities, in cases of pregnancy-related venous insufficiency.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
This cohort study was carried out upon approval from Research Ethical Committee, Faculty of Allied Health Sciences, The University of Lahore REC-UOL-165-10-22.
Informed Consent
Informed consent was not sought for the present study because all case data was de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because no animals were used.
Trial Registration
Not applicable.