
Abstract
Objective:
This systematic review aims to determine the extent, scope, and nature of research using the sonographic measurement of intraneural blood flow within the median nerve and to identify, characterize, and compare image acquisition and analysis protocols that have been reported as potential candidate techniques for standardizing research and clinical applications.
Materials and Methods:
This systematic review summarizes image acquisition protocols and analysis methodologies from 52 current research studies using Doppler ultrasound to examine median nerve intraneural blood flow.
Results:
Four types of Doppler technologies were identified: power Doppler, color Doppler, spectral Doppler, and Superb Microvascular Imaging, but there were inconsistencies in how images were acquired and analyzed. Intraneural blood flow measurements were categorized into four types based on a combination of measurement level (e.g., binary, ordinal, continuous) and type of flow indicator (e.g., pixel count, intensity, velocity).
Conclusion:
Standardized imaging protocols and reporting guidelines are needed to improve consistency. Future studies should evaluate the accuracy and reliability of different image acquisition methods and analysis measurements.
With the advancement of ultrasound technologies, such as high-frequency linear-array transducers and software programs, there is an increase in the ability of Doppler ultrasound to detect low flow states in exceedingly small blood vessels. One area of such technology being adopted is in the evaluation of intraneural blood flow within the median nerve. Some studies have demonstrated that an increase in intraneural blood flow might be a sign of pathology in the median nerve, such as in carpal tunnel syndrome (CTS) and chronic inflammatory demyelinating polyneuropathy.1,2 In the case of CTS, the median nerve is vulnerable to compression while traveling through the carpal tunnel and may undergo pathological changes, such as nerve edema, ischemia, neovascularization, and demyelination. 3 Some studies have demonstrated that the presence of intraneural blood flow is associated with the early pathologic signs of CTS, which can be used to help identify CTS patients in the early phases.4,5
Given the promising use of Doppler ultrasound in detecting blood flow signals of small vessels, there is an increase in the number of studies examining the intraneural blood flow of the median nerve in the carpal tunnel area using Doppler ultrasound. A previous review article identified wide variability in the sensitivity of intraneural blood flow measurement for the diagnosis of CTS, ranging from 41% to 95%. 6 A potential explanation for the wide range of the sensitivity is that the studies examined in the previous review adopted various methods of image acquisition and analysis. Some of the studies used color Doppler, other studies used power Doppler, and a few studies evaluated diagnostic sensitivity using spectral Doppler. Moreover, the location of nerve evaluation differed across the studies. Finally, when analyzing the Doppler images, techniques ranged from counting the number of blood vessels to quantifying the intensity or velocity of the blood flow.
The inconsistency in image acquisition techniques and significant differences in the image analysis methods make it exceptionally challenging to compare results across studies and hinder the ability to use intraneural blood flow as a valid physiologic measure in research or diagnostic indicator in clinical practice. Given the increased use of this measurement, it is vital to identify a rigorous approach and establish a standardized imaging acquisition and analysis method that can ensure valid application of Doppler ultrasound in detecting peripheral nerve blood flow. Therefore, the aims of this systematic review were to determine the extent, scope, and nature of research using the sonographic measurement of intraneural blood flow within the median nerve and to identify, characterize, and compare image acquisition and analysis protocols that have been reported as potential candidate techniques for standardizing research and clinical applications.
Materials and Methods
This systematic review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guideline. 7 Searches were completed in PubMed and CINAHL for relevant studies that used ultrasonography to examine median nerve intraneural blood flow. A preliminary search of PubMed and CINAHL was conducted to identify MeSH (Medical Subject Headings) terms and keywords. Three constructs were explored, including “ultrasonography,” “median nerve,” and “blood flow.” The full search strategy was built by combining the identified search terms within each construct using the “OR” operator and subsequently combining the three constructs with the “AND” operator. Considering the limited ability of Doppler ultrasound technology to detect small blood flow signals in earlier years, the search reference period was set from January 1, 2000. There were no publication language or region restrictions. The full search strategy, as provided in Table 1, was performed on August 31, 2021. To identify any additional sources, a hand search was conducted of the reference lists of included articles or related review articles and the table of contents of two journals that had published the highest number of included articles (i.e., Muscle and Nerve and Journal of Ultrasound in Medicine).
Search Terms Used to Identify Articles Using Sonography to Measure Intraneural Blood Flow Within the Median Nerve.
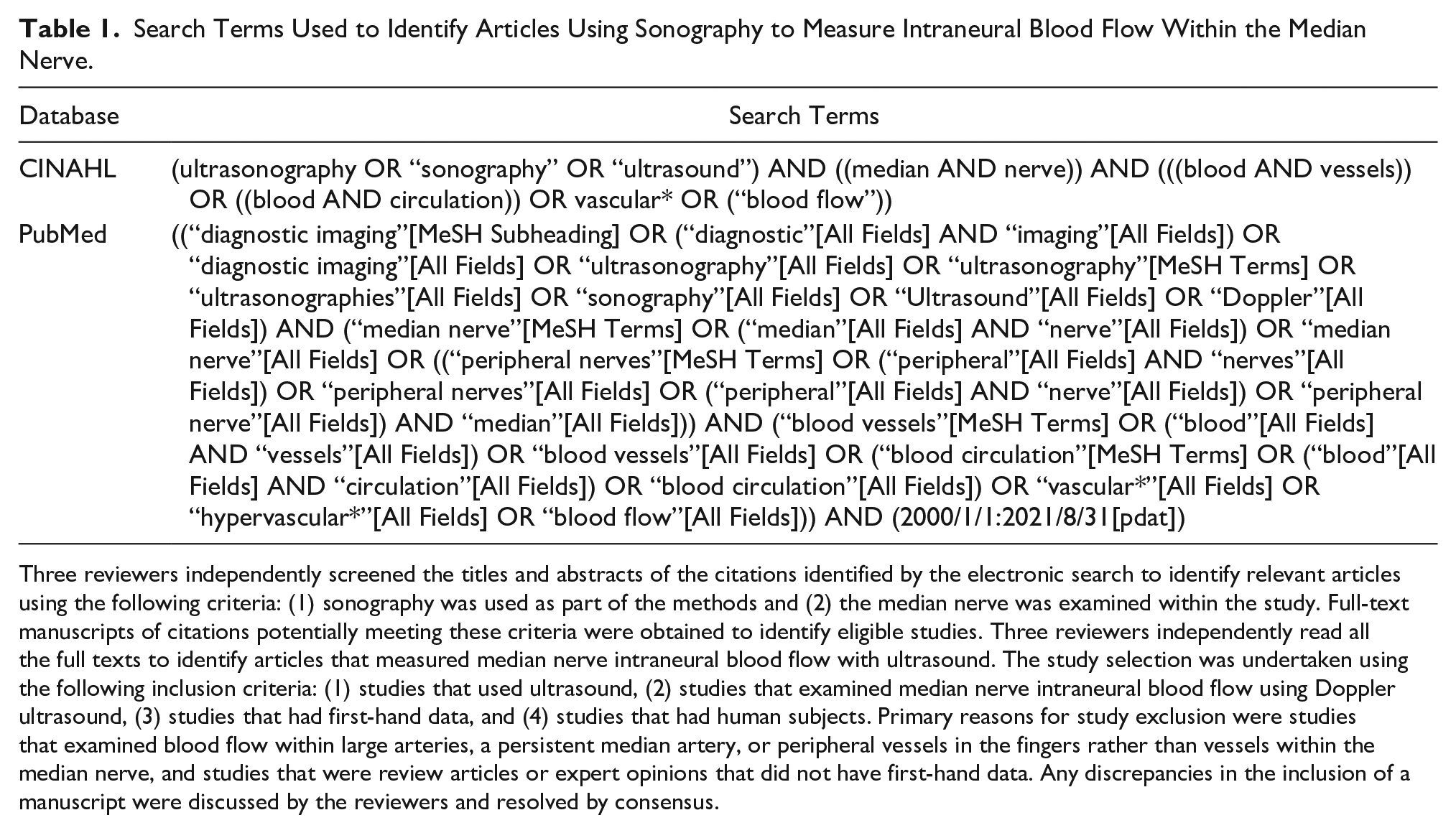
Three reviewers independently screened the titles and abstracts of the citations identified by the electronic search to identify relevant articles using the following criteria: (1) sonography was used as part of the methods and (2) the median nerve was examined within the study. Full-text manuscripts of citations potentially meeting these criteria were obtained to identify eligible studies. Three reviewers independently read all the full texts to identify articles that measured median nerve intraneural blood flow with ultrasound. The study selection was undertaken using the following inclusion criteria: (1) studies that used ultrasound, (2) studies that examined median nerve intraneural blood flow using Doppler ultrasound, (3) studies that had first-hand data, and (4) studies that had human subjects. Primary reasons for study exclusion were studies that examined blood flow within large arteries, a persistent median artery, or peripheral vessels in the fingers rather than vessels within the median nerve, and studies that were review articles or expert opinions that did not have first-hand data. Any discrepancies in the inclusion of a manuscript were discussed by the reviewers and resolved by consensus.
Two reviewers undertook data extraction to capture information on imaging acquisition, imaging analysis, and general study characteristics, such as author, journal, publication year, country, and study population. Studies were categorized by four types of Doppler imaging, including color Doppler, power Doppler, spectral Doppler, or superb microvascular imaging. Second, studies were categorized by the technique used to analyze the Doppler signals as (1) a binary outcome of the presence or absent of vascular signals within the region of interest without further grading, (2) an ordinal outcome of the grade of blood flow signals based on counting and scoring the blood flow signal numbers, (3) a continuous outcome of the amount of the blood flow that was measured as the pixel intensity of identified blood flow signals or the number of pixels, and (4) a continuous outcome of the velocity of the blood flow that was measured as the peak systolic velocity (PSV).
Since the purpose of this systematic review was to summarize image acquisition and analysis protocols that have been adopted by existing research to identify potential candidate methods, quality assessment of overall study methodologies or reporting was not completed. Instead, studies with similar image acquisition and analysis methods were summarized and compared. Specifically, iterative discussions among the authors were conducted to develop qualitative syntheses of the variability, strengths, limitations, and implications for clinical utility among studies within and across the acquisition and analysis categories.
Results
A total of 570 records with titles and abstracts were retrieved from the database search, and another eight studies were identified through the hand search. After removing the duplicated studies, a total of 520 records were screened, and a total of 361 irrelevant articles were eliminated. Thereafter, the full texts of 159 studies were reviewed, of which 52 studies met the eligibility criteria for inclusion in qualitative synthesis. An illustration of the study selection process is presented in Figure 1. Eight studies were conducted in the United States, five were conducted in India, five were conducted in Egypt, and Australia, Canada, Turkey, and Iran were each represented by four studies. Although studies published after 2000 were searched and reviewed, only three articles were published before 2010 with the remaining 49 studies being published since 2010 (Figure 2). Patients with CTS or clinically suspected CTS were included in a majority of the studies (67.3%, 35 of 52 articles); the details for these studies are included in Table 2. Other common populations being studied included patients diagnosed with diabetes, leprosy, and chronic inflammatory demyelinating polyneuropathy; details for these studies are included in Table 3.
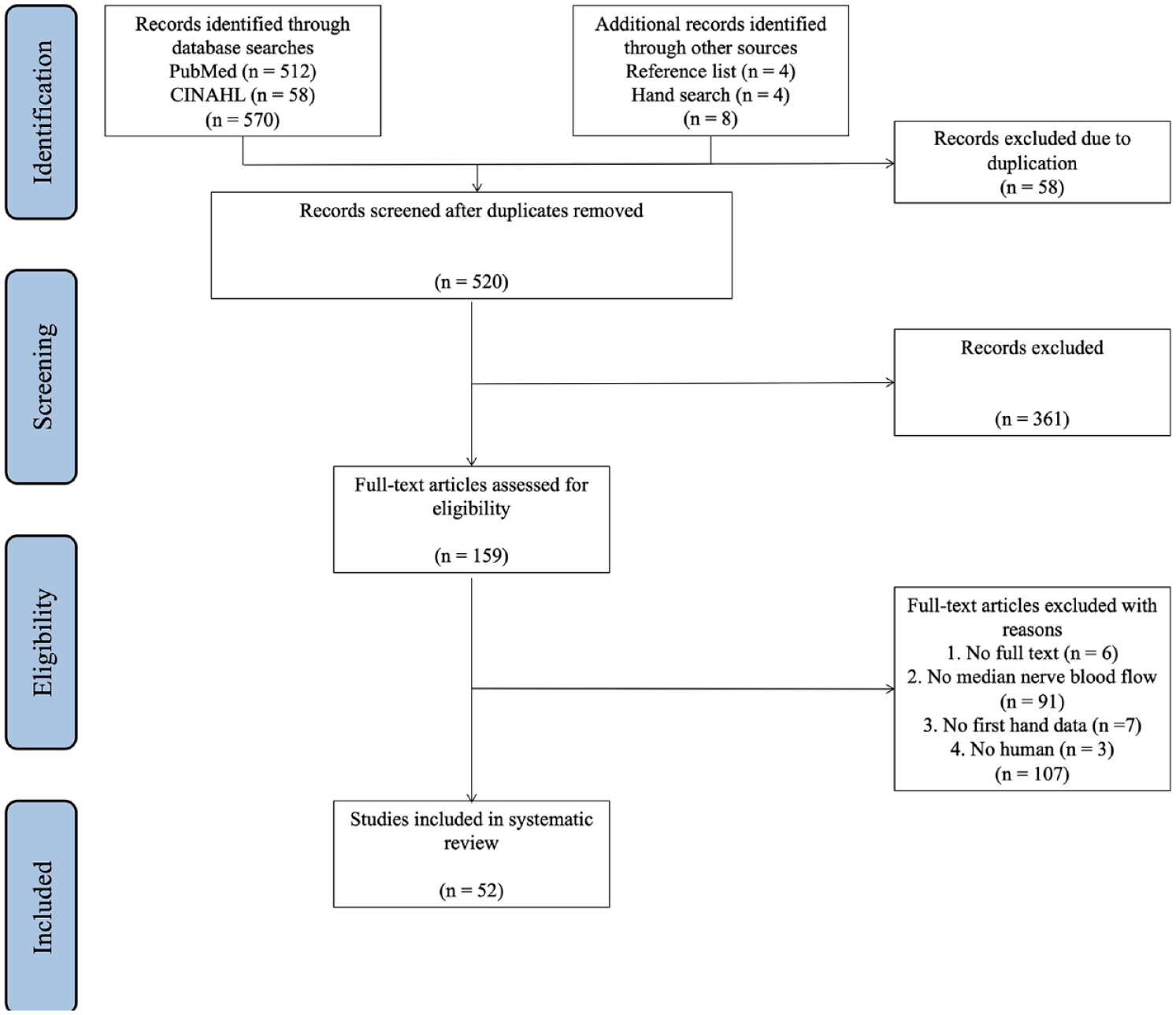
Flow diagram of the study review and inclusion process.
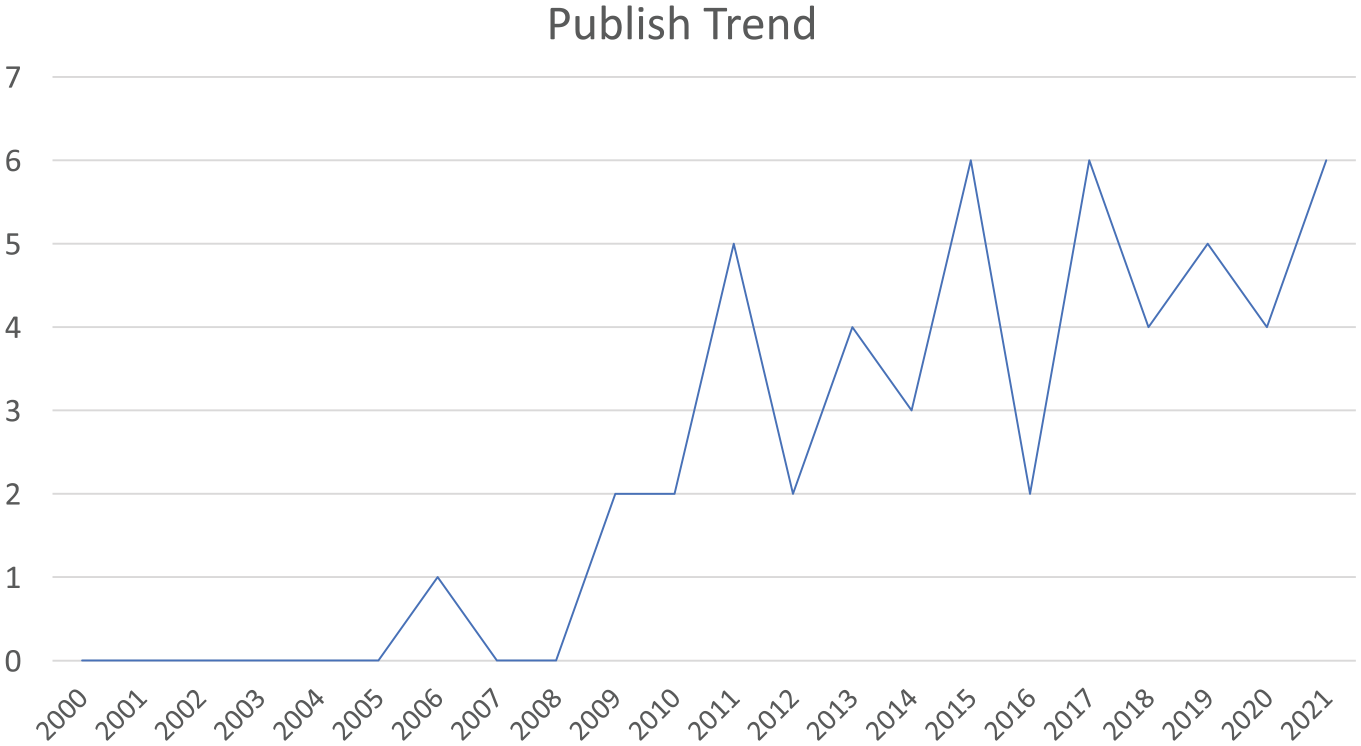
The publishing trend of studies on the topic of examining median nerve intraneural blood flow with sonography.
Descriptive Characteristics of Studies Examining Intraneural Blood Flow Within the Median Nerve Among Patients With Carpal Tunnel Syndrome (CTS, n = 35).
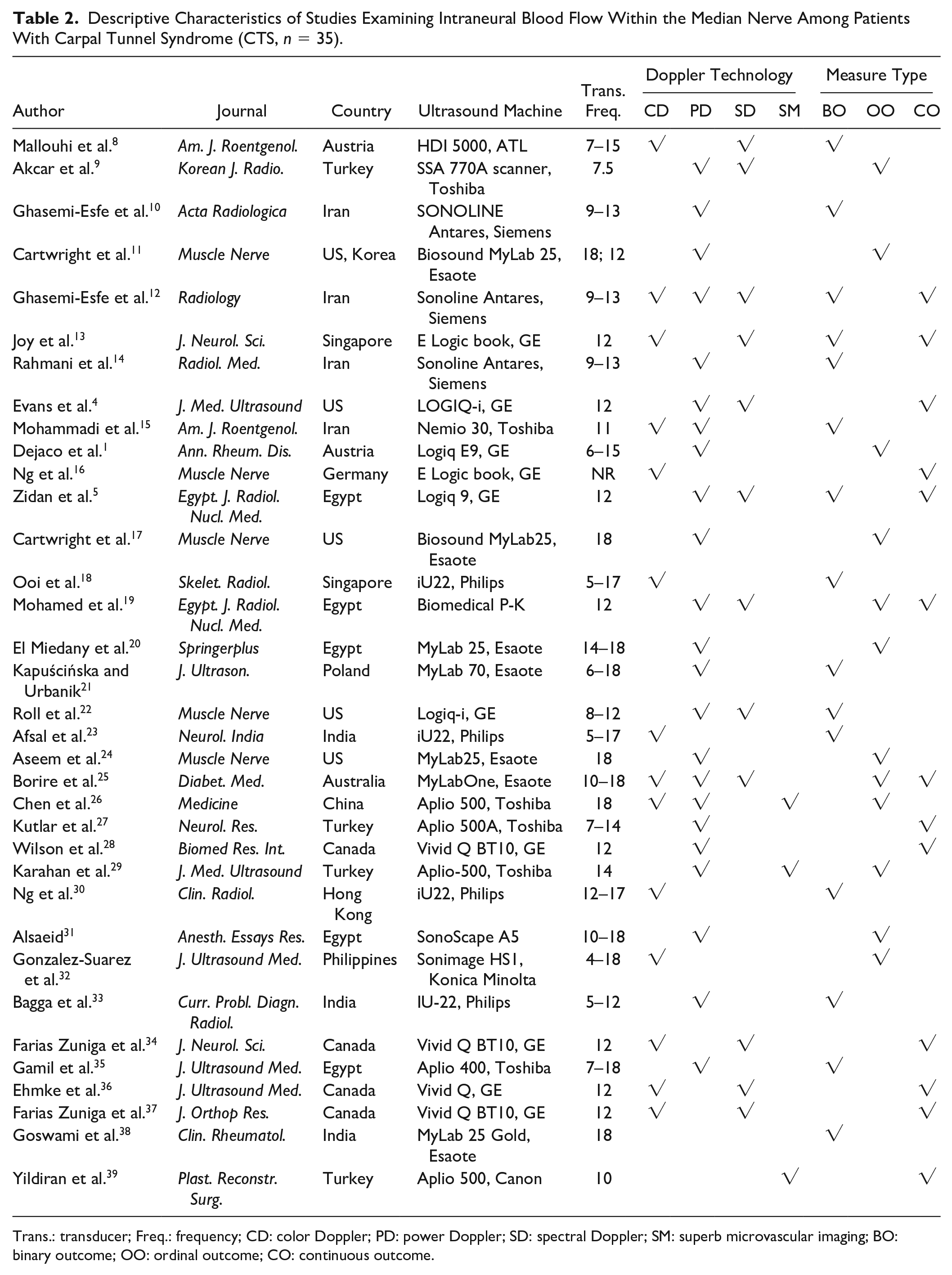
Trans.: transducer; Freq.: frequency; CD: color Doppler; PD: power Doppler; SD: spectral Doppler; SM: superb microvascular imaging; BO: binary outcome; OO: ordinal outcome; CO: continuous outcome.
Characteristics of Studies Examining Intraneural Blood Flow in Non-CTS Populations (n = 17).
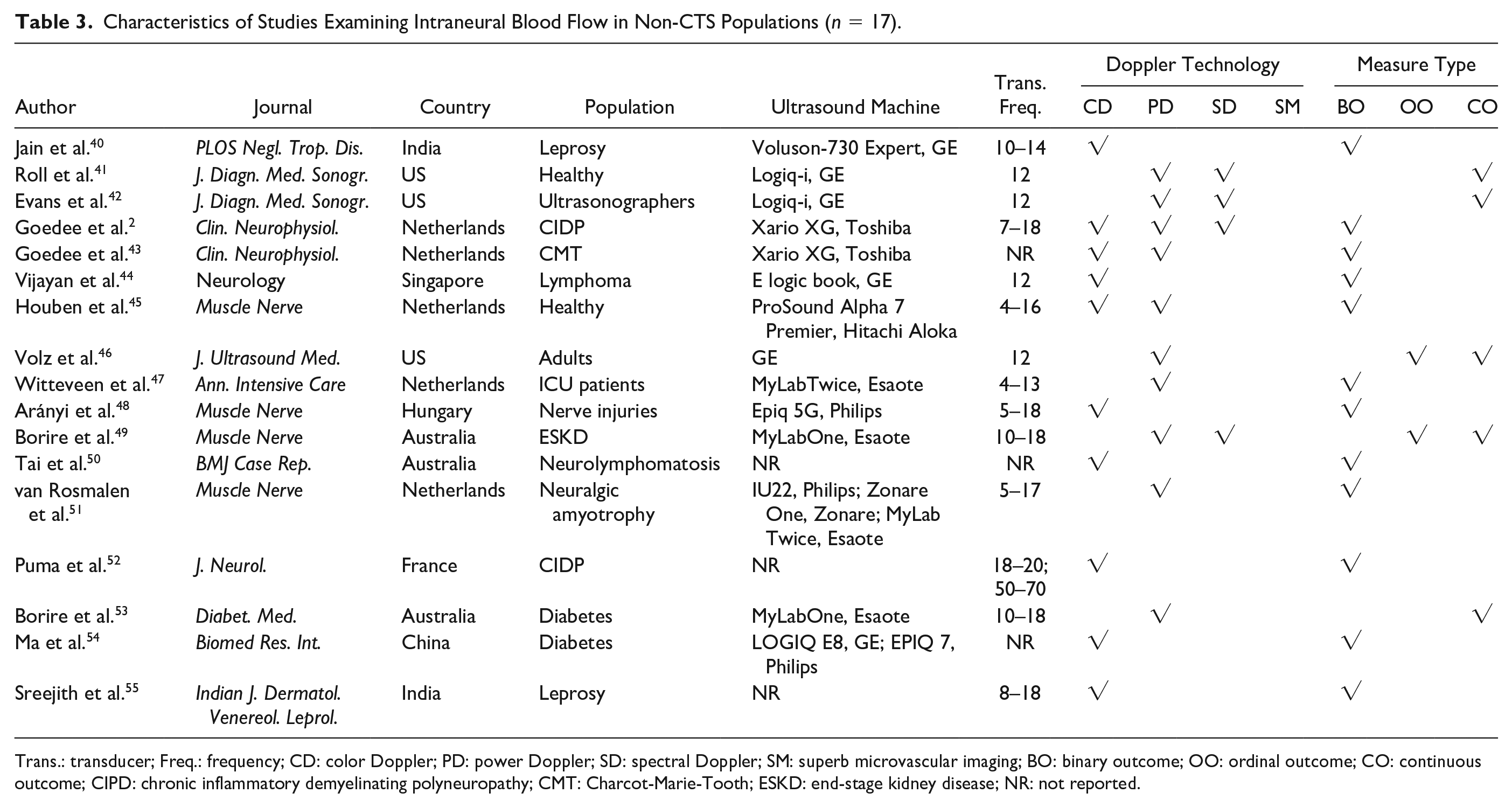
Trans.: transducer; Freq.: frequency; CD: color Doppler; PD: power Doppler; SD: spectral Doppler; SM: superb microvascular imaging; BO: binary outcome; OO: ordinal outcome; CO: continuous outcome; CIPD: chronic inflammatory demyelinating polyneuropathy; CMT: Charcot-Marie-Tooth; ESKD: end-stage kidney disease; NR: not reported.
Image Acquisition
The most frequently used imaging modality to detect blood flow signals within the median nerve was power Doppler (61.5%, 32 of 52), followed by approximately half of the studies using color Doppler (48.1%, 25 of 52), and spectral Doppler (i.e., pulse wave Doppler) appearing in 16 studies (30.8%).(Figure 3). Spectral Doppler was used in some studies to confirm that the pulsatile signals obtained from power Doppler were truly vascular due to its ability to display the blood flow velocity over time as a spectrum and to distinguish true arterial waveforms from artifacts. 49 Some studies also used spectral Doppler to quantitatively measure the PSV of the blood flow within the median nerve by obtaining the classic arterial waveforms. 49
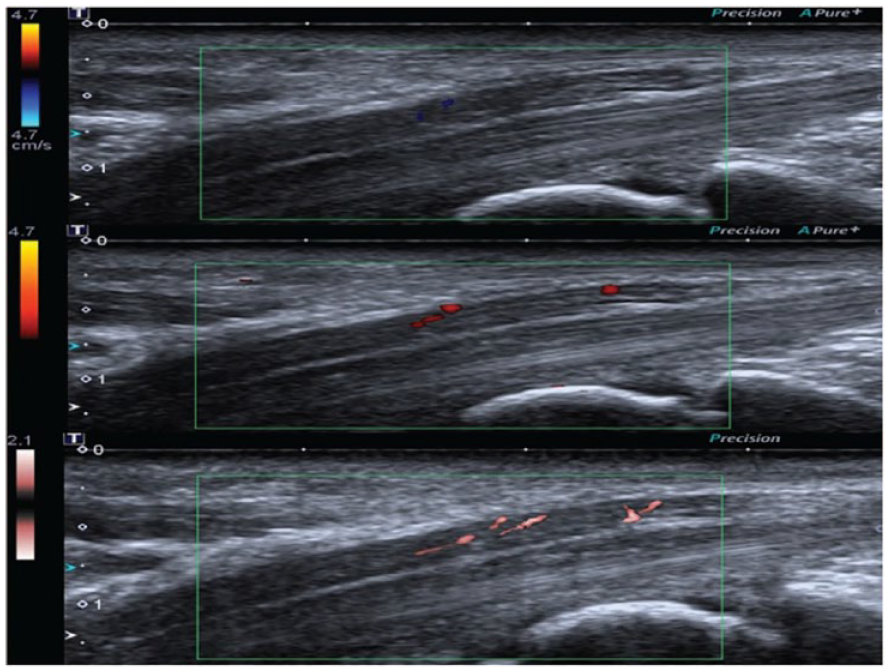
Ultrasound images of the MN at the same level from a 65-year-old female CTS patient, which shows score 1 by CDUS, score 2 by PDUS, and score 3 by SMI. CDUS = color Doppler ultrasonography, CTS = carpal tunnel syndrome, PDUS = power Doppler ultrasonography, SMI = superb microvascular imaging. Cited from Chen et al. 26
In addition to traditional Doppler methods, three studies used superb microvascular imaging to examine the vascularity within the median nerve.26,29,39 Superb microvascular imaging is a relatively new Doppler-based imaging method that has an advantage in eliminating the artifacts and can reveal low-velocity vascular signals more sensitively. 56 This technology was first published in 2016 to examine blood flow in thyroid tissues, 57 and the studies employing this technology in the median nerve were published in 2017, 2018, and 2021.26,29,39
The imaging planes and location of median nerve evaluation widely varied across studies. Among the included studies, 17 (32.7%) studies examined only in long axis (i.e., sagittal plane), 17 (32.7%) studies examined only in the short axis (i.e., axial plane), and 16 (30.8%) studies examined in both planes. Most studies did not provide clear or precise descriptions of the measurement locations. The lack of description was most frequently noted when examining the median nerve in long axis, leaving it unclear as to which part of the median nerve was examined. Among studies that reported anatomic landmarks or specific imaging locations, there was no consistency or predominate location. For example, Mohammadi et al. 15 examined the vascularity above the carpal tunnel region, while Ng et al. 30 examined the presence of vascularity from the distal forearm to the carpal tunnel outlet.
Across the studies, numerous different ultrasound machines were used, and the frequency of the transducers ranged from 7.5 to 50 MHz. Machine settings for power Doppler imaging were rarely provided, and the reported settings for spectral Doppler varied greatly in terms of frequency, pulse repetition frequency (PRF), wall filter, gate width, and angle adjusting. Given the lack of details provided for ultrasound settings, variability in the Doppler modalities used, and lack of standardization in the imaging planes and anatomic locations examined, the synthesis or comparison of findings across studies is limited, even among studies that applied similar analytic criteria.
Image Analysis
Among the four types of measures, the most frequently reported was a binary outcome that indicated the presence or absence of intraneural blood flow, which appeared in 27 studies (51.9%). Binary categorization is the most straightforward, and potentially the most reliable, method to analyze intraneural blood flow as it does not require software or extensive expertise. However, any assessment of reliability or recommended utility of this outcome is hampered by a lack of standardization in the criteria for validating the presence of intraneural flow. In fact, most studies (70.4%, 19 of 27) did not report the specific criteria used to initially determine or validate the presence of blood flow. Among those that did provide criteria, some studies specified that the signals required a pulsatile characteristic to rule out tiny artifactual colored pixels (e.g., Ghasemi-Esfe et al. 10 ). Other studies required the pulsatile signals to have at least five consistent cycles (e.g., Wilson et al.; 28 Ehmke et al. 36 ), and many studies used spectral Doppler to confirm the blood flow signals (e.g., Borire et al.;25,49,53 Ghasemi-Esfe et al. 12 ). Finally, Ooi et al. 18 specified that the vascular signals need to be greater than 1 mm in length to be counted as the presence of hypervascularity.
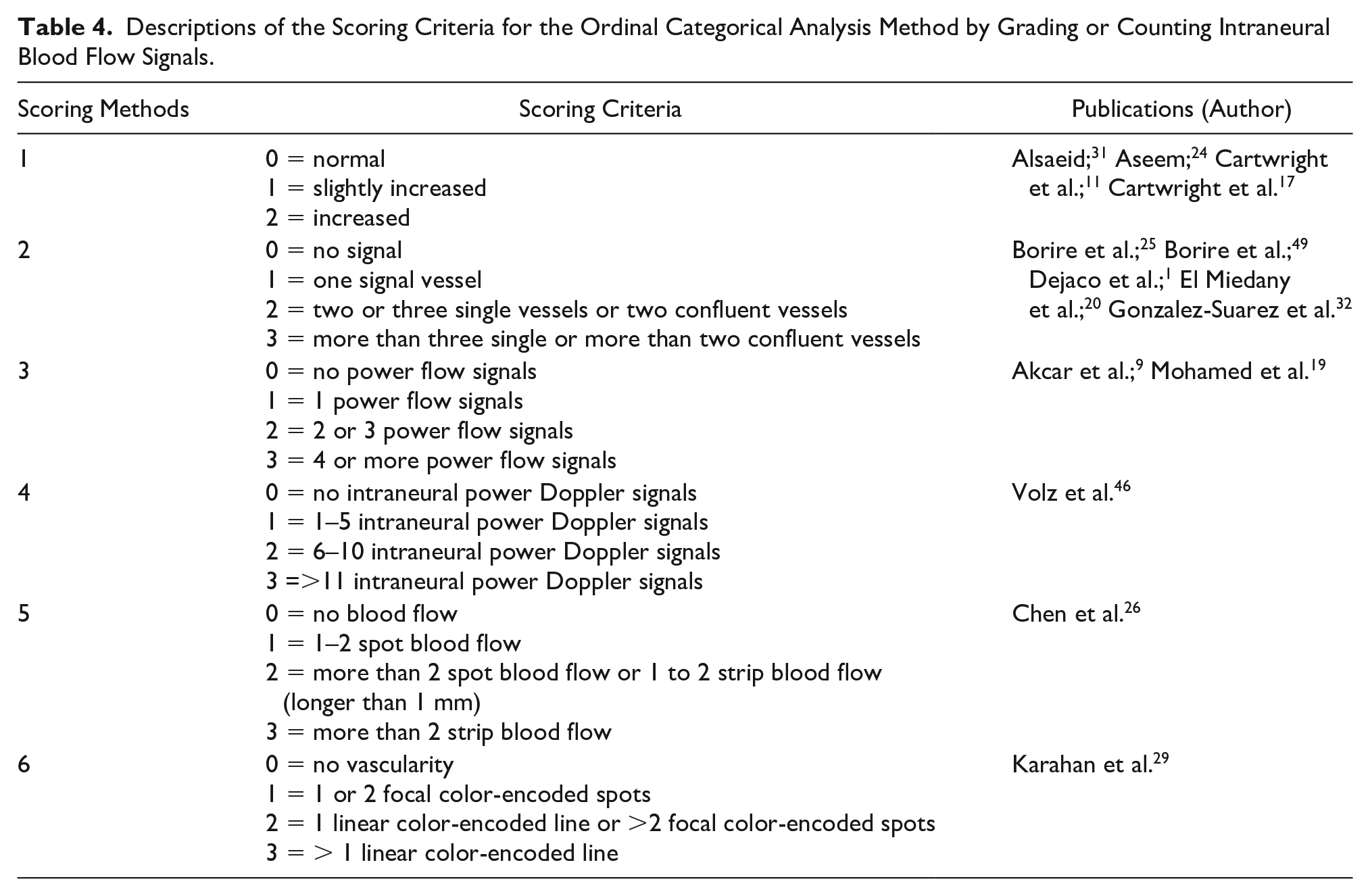
Expansion beyond general presence into an ordinal outcome based on the number of signals was used in 14 (26.9%) of the studies (see Table 4). These studies either counted the individual signals or used increasing frequency of signals within a region of interest to create categories. A four-level rating was the most common analysis method used in ten studies; however, there were slightly different descriptions of the scoring criteria across these studies. The most common criteria rated power Doppler signals from 0 to 3, in which 0 represented no signals, 1 represented a single vessel within the median nerve, 2 indicated two or three signals or two confluent vessels, and 3 indicated more than three signals or more than two confluent vessels. The remaining four studies categorize the amount of blood flow into three levels by indicating that vascularity was “increased,” “slightly increased,” or “normal,” where “normal” means no color Doppler signal in the nerve (Cartwright et al.;11,17 Aseem et al.; 24 Alsaeid 31 ).
Descriptions of the Scoring Criteria for the Ordinal Categorical Analysis Method by Grading or Counting Intraneural Blood Flow Signals.
There were 18 (34.6%) studies that adopted an image analysis method that generated a continuous outcome of intraneural blood flow. As shown in Table 5, eight studies (15.4%) analyzed power Doppler signals. Three studies reported the sum of pixels that included a Doppler signal within the median nerve in the long axis.12,16,27 Ghasemi-Esfe et al. 12 used a self-developed program in MATLAB to evaluate images obtained at the pisiform level of carpal tunnel, whereas Kutlar et al. 27 used Osirix open-source software to evaluate the median nerve at the entrance to the carpal tunnel. Ng et al. 16 reported the averaged sum of pixels of three time periods using National Institute of Health J software. Similarly, Yildiran et al. 39 reported a sum of Doppler pixels, but examined the nerve in short axis. While a sum of pixels can be useful for within study comparisons, variability in pixel size and other machine settings across ultrasound equipment and differences in the size of the region of interest limits comparison or generalizability of this measure. Borire et al.25,49,53 and Volz et al. 46 measured the maximum pixel intensity (MPI), which is a measure of quantity of flow within the region of interest. MPI is demonstrated by the color intensity of the pixel that has the maximum color intensity within the region of interests, and the measure is automatically derived by PixelFlux. These authors provided detailed descriptions of the machine settings used, such as frequency, PRF, gain, time-gain compensation, and harmonics, which can assist in comparing data between subjects and across studies.
Image Acquisition and Continuous Outcome Analysis Methods Used by Studies That Analyzed Power Doppler Signals.
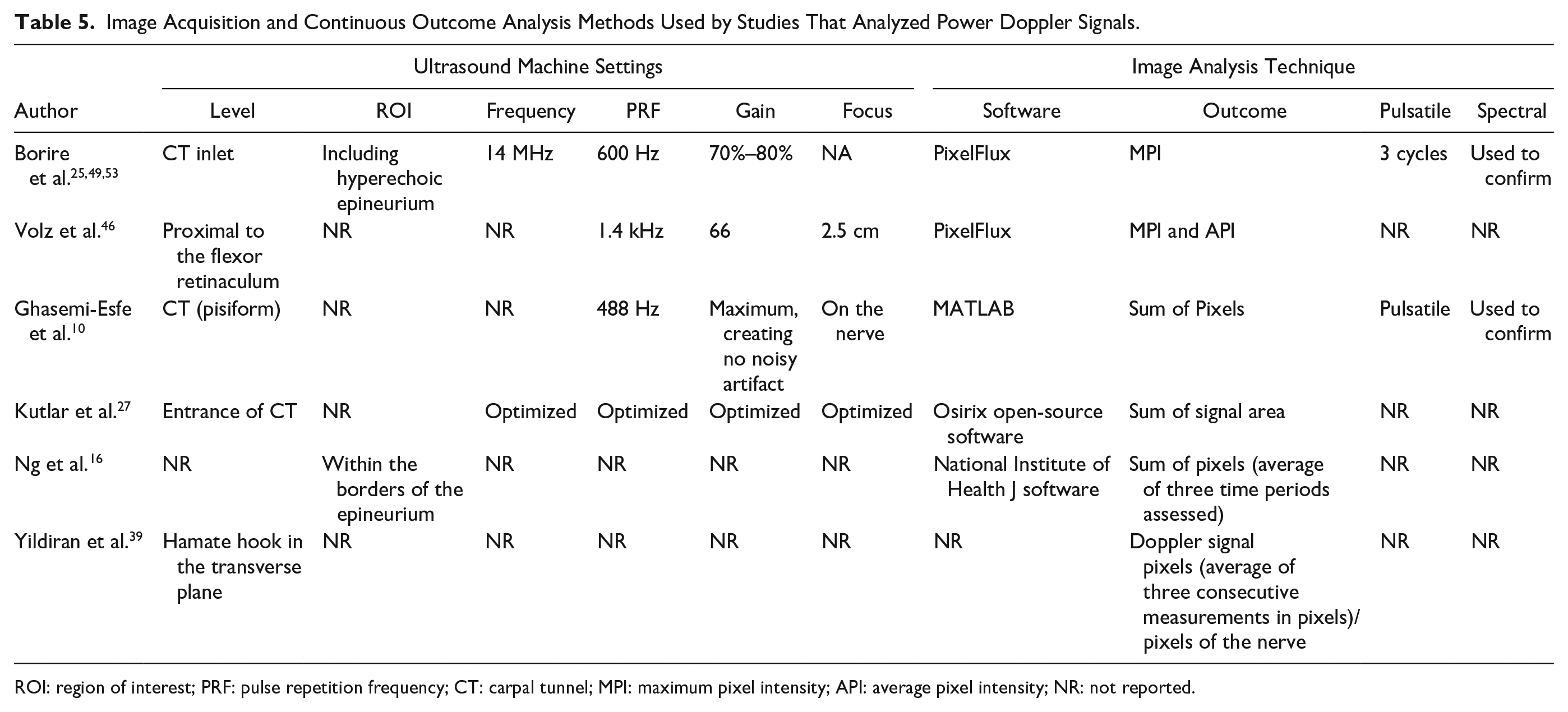
ROI: region of interest; PRF: pulse repetition frequency; CT: carpal tunnel; MPI: maximum pixel intensity; API: average pixel intensity; NR: not reported.
A total of 10 (19.2%) studies used spectral Doppler to examine the velocity of intraneural blood flow as the primary continuous outcome (Table 6). Peak systolic velocity was the most frequently reported measure, used by eight of the studies. Different criteria of analyzing the PSV were adopted by these studies. For example, Ehmke et al. 36 used the average PSVs across a serial of steady blood flow signals containing five cycles. 36 Evans et al. 4 used the average of two cycles. Wilson et al. 28 used the initial PSV of five stable cycles, while Farias Zuniga et al.34,37 used the average PSV of a serial of consistent blood flow signals over five seconds. Joy et al. 13 measured PSV, and Evans et al. 42 and Roll et al. 41 measured both PSV and end diastole velocity (EDV). Two of the eight studies used EchoPack software,28,36 one study used MAUI analysis software, 37 and other studies measured PSV using the ultrasound machine. As an alternative to using PSV, Zidan et al. 5 and Mohamed et al. 19 measured the pulsatility index, which is calculated as the PSV minus end diastolic velocity all divided by mean velocity.
Image Acquisition and Continuous Outcomes Methods Used by Studies That Analyzed Spectral Doppler Waveforms.
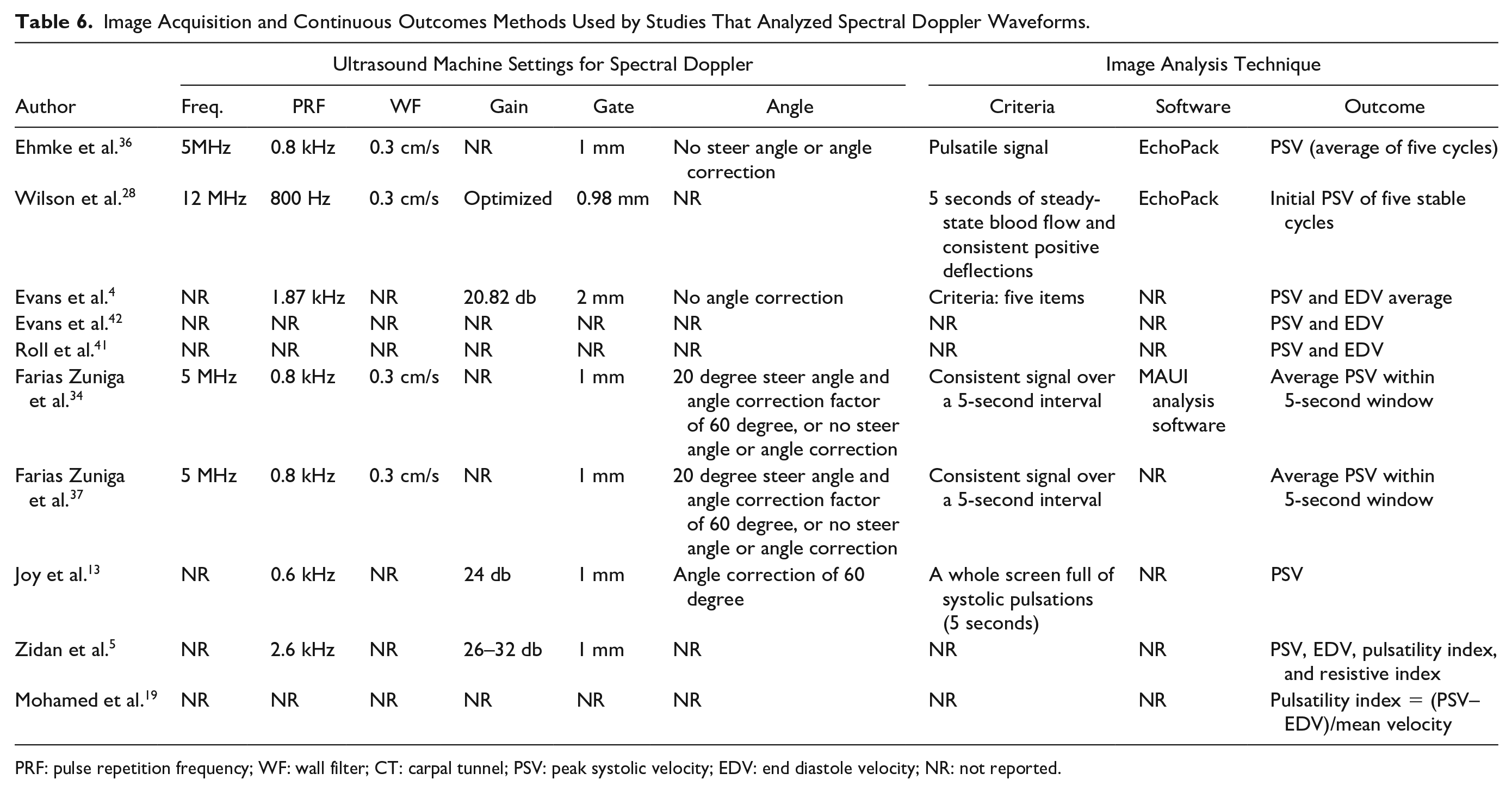
PRF: pulse repetition frequency; WF: wall filter; CT: carpal tunnel; PSV: peak systolic velocity; EDV: end diastole velocity; NR: not reported.
If conducted using a standardized acquisition protocol combined with signal validation criteria, these spectral Doppler measures have the strongest potential for reliable comparison across studies due to limited measurement bias. Among these studies, Evans et al. 4 was the only study to report detailed criteria for evaluating the validity or quality of spectral Doppler waveforms. Their criteria included five items regarding the quality of the spectral Doppler waveforms and the gray scale image.
Reliability of Image Analyses
Only 10 (19.2%) studies reported inter-observer and/or intra-observer reliability (Table 7). Three studies reported an excellent inter-reliability and intra-reliability for the binary measurement of intraneural blood flow, which ranged from 0.81 to 0.90 (kappa). Wider variability in reliability of the ordinal categorization was reported by Dejaco et al. 1 and El Miedany et al. 20 with weighted kappa for inter-rater reliability at 0.51 and 0.78 and intra-rater reliability at 0.65 and 0.85. Intraclass correlations (ICCs) reported in one study for the continuous measurement of MPI demonstrated excellent inter- and intra-observer reliability at 0.95 and 1.0, respectively. 25 Intra-observer reliability for the continuous measurement of PSV was widely variable and inconsistent when compared across measurements taken with the wrist in different positions. 28
Reliability for Different Types of Sonographic Measurements of Intraneural Blood Flow.
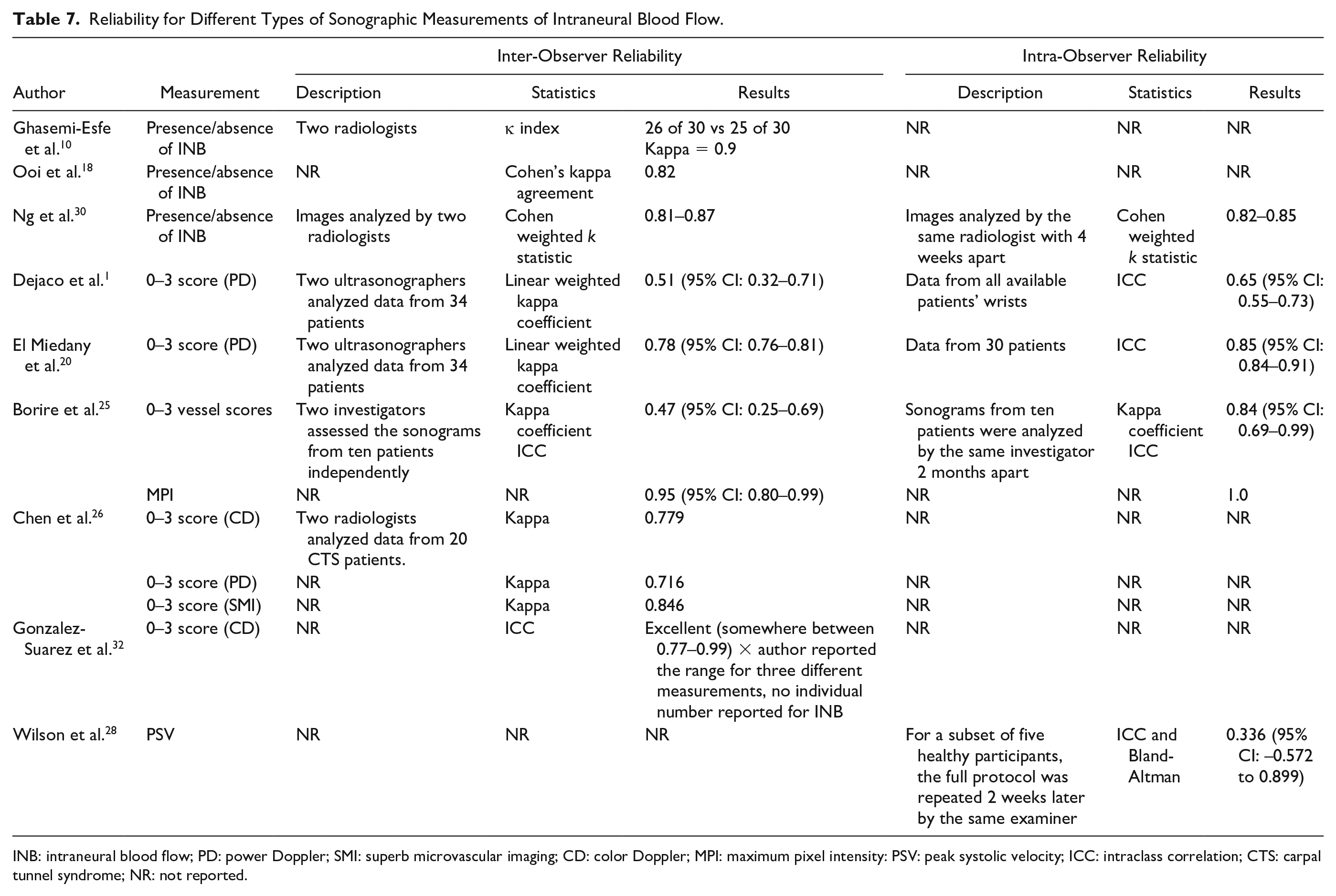
INB: intraneural blood flow; PD: power Doppler; SMI: superb microvascular imaging; CD: color Doppler; MPI: maximum pixel intensity: PSV: peak systolic velocity; ICC: intraclass correlation; CTS: carpal tunnel syndrome; NR: not reported.
Clinical Utility
The use of intraneural blood flow for the diagnosis of CTS was the most common clinical application explored. Six of the included studies reported the diagnostic value of the binary type of measurement of intraneural blood flow, demonstrating a wide range of sensitivity (4%–95%) and specificity (71%–100%).8,10,18,30,35,38 When using a score of two or more signals as a diagnostic cut point, the sensitivity and specificity for an ordinal categorization of blood flow ranged from 19.1% to 47.4% and from 89.8% to 96.6% when measured at different locations. 1
Rather than relying on one measure of intraneural blood flow as a diagnostic criterion, other studies proposed methods for combining blood flow with other clinical measures, or using blood flow as an indicator of severity. For example, Joy et al. 13 found that the combination of intraneural blood flow and cross-sectional area (CSA) of the median nerve may improve the diagnostic value of sonography in detecting CTS. This has been echoed by others who have demonstrated that any combination of median nerve CSA > 12 mm2, abnormal mobility, echogenicity, or vascularity, resulted in a sensitivity of 89%. 17 Mixed results have been documented relating vascularity to CTS severity, where some studies suggest there is an inverse relationship,4,5 and other studies finding the relationship to be positively related.12,15,19,27 Despite a need for further exploration, a scoring and severity grading system using vascularity as one of multiple sonographic and clinical measures has been suggested for diagnosing CTS. 22
Although most studies focused on the diagnosis of CTS, intraneural blood flow has been also used in other ways, such as evaluating treatment outcomes and predicting the prognosis of CTS treatments. For example, Yildiran et al. 39 documented that intraneural vascularity decreased in moderate and severe CTS patients after surgery decompression. More recent studies suggest that an ordinal score of more than 2 is a predictor of good outcomes in response to management, 20 and that intraneural blood flow velocity is a significant predictor of nerve sensory and motor changes at six months. 37
Discussion
This systematic review was undertaken to summarize the methods used in the literature to measure median nerve intraneural blood flow using Doppler sonography, and compare different imaging acquisition and analysis protocols as a foundation for identifying best practices. The final review included 52 studies, with 90% of the studies conducted within the past 10 years. Four Doppler technologies were used for image acquisition and four types of intraneural blood flow measurements were identified and compared. Due to the lack of a standardized method and reporting guidance, not enough evidence exists to conclude which image acquisition and analysis method is the most optimal for future research and clinical use. Although intraneural blood flow has been applied in many study areas, the most common area is to use intraneural blood flow as a biomarker to diagnose CTS.
Current Landscape of Intraneural Blood Flow Analysis
As can be seen in the results of this systematic review, there are many ways of acquiring images of intraneural blood flow using Doppler ultrasound, and there are significant inconsistencies in reporting across the studies. These inconsistencies include a lack of information on standardized machine settings across the different types of Doppler technologies used (i.e., power Doppler, spectral Doppler, superb microvascular imaging). Moreover, there is a lack of clarity as to where and how the blood flow signals should be detected. This includes which plane should be examined (transverse vs longitudinal), which part of the median nerve should be examined (at carpal tunnel or at distal forearm), and what length of the median nerve should be examined (just limited at carpal tunnel region or the whole wrist region from proximal carpal tunnel to distal carpal tunnel).
In like manner, there are also many different image analysis methods. In this systematic review, four types of measurements of intraneural blood flow have been compared and summarized (i.e., binary, ordinal, and continuous measures). Even within each measurement type, significant inconsistencies are noted in how the outcome measure is obtained. For example, there is a general lack of description for the best criteria for validating the presence of blood flow, along with variations in qualitative criteria and the grading scales used for ordinal categorization of blood flow, such as the discrepancies between using three or four levels for assessment. Even among continuous outcome measures, there is a lack of standardization regarding the way in which pixel area, MPI, and PSVs are analyzed. It is vital to develop and adopt standardized criteria not only for the measurement techniques but also for validating that that signal or spectral tracing is not an artifact.
Comparing the image acquisition protocols and image analysis methods used and identifying the best technique for measuring intraneural blood flow are difficult. First, some studies reported poorly on their imaging methods. For example, some machine settings are reported in some studies but not in others; some studies did not mention their criteria for the presence of blood flow, nor did they mention the plane, position, or parts of the median nerve that they examined. Second, for the studies that did report the imaging acquisition methods, the differences exist in the technical equipment and scanning protocol that could influence the detection of intraneural blood flow and make it difficult to compare their results.
In addition to wide variability in acquisition techniques and poor reporting of methods, very few studies have compared multiple imaging technologies or image analysis methods within their studies. Power Doppler is stated to be superior to color Doppler in that it is more sensitive for detecting low-velocity blood flow signals; 58 however, no studies have compared the sensitivity of the two technologies. Karahan et al. 29 was the only study to compare techniques, but this study examined the sensitivity of superb microvascular imaging and power Doppler imaging, and concluded that superb microvascular imaging is more sensitive. Borire et al. 25 compared two image analysis methods from data obtained with power Doppler, MPI and counting the number of blood vessels, concluding that MPI might have an advantage in having a better inter-observer reliability and providing more values as a continuous variable. More studies are needed in determining the sensitivity in different image acquisition protocols and the reliability in different image analysis methods.
Opportunities to Advance Intraneural Blood Flow Analysis
Given the variation in image acquisition and analysis that has made comparing the results very challenging, there is a demonstrated need for standardized protocols for using Doppler sonography in the examination of intraneural blood flow in the median nerve. Due to a lack of evidence regarding the best technique, multiple protocols may be most useful to account for differences in the resources, effort and time required in each method. The clinician’s time and effort, the ultrasound technology, machine, and hardware requirements, and the analysis software requirements vary across the different methods. For example, a simple binary outcome of identifying the presence of blood flow using power Doppler might be easy enough to complete in any clinical setting. This binary outcome of intraneural blood flow requires the least time and does not require any additional analysis. Conversely, a clinic or research laboratory that has access to specialized software for analysis may benefit from a protocol that examines continuous measures of blood flow from power or spectral Doppler images.
Regardless of the protocol being used, clear criteria should exist to maximize the rigor, validity, and sensitivity of the interneural blood flow measurement. Protocols should clearly define what counts as a true vascularity signal to rule out other artificial signals. A scoring of the number of vessels of the blood flow may serve as a measurement for a part of the standard in assessing the severity of CTS, and is more robust than the binary measurement of intraneural blood flow. More robust measurement of intraneural blood flow, such as the continuous measurement of PSV or the pixel intensity, might provide more information, and may be the most appropriate measurement to be used in academic settings. However, these measurements do require more time and manpower to conduct the image analyses, and usually require access to software or hardware that might not be available. For example, the superb microvascular imaging function only exists in certain ultrasound machines.
Once standardized protocols are established for each of the measurements (binary, ordinal, and continuous), more studies should examine the correlation among these types of measurements; the inter- and intra-observer reliability of each of the measurements should be reported. The results of these different types of measurements cannot be compared and summarized until the consensus of the correlation among these measurements has been achieved. A review article published in 2014 concluded that a wide range of sensitivity (41%–95%) and specificity (71%–100%) existed, and the results should be interpreted with caution due to potential bias and flaws in the study design. 6 This review article has compared and synthesized multiple intraneural blood flow measurements (binary, ordinal, and continuous outcome measures) collected by multiple technologies (color, power, and spectral Doppler). However, without a standardization of image acquisition methods and a consensus of the correlation among these types of measurements, the measurements detected by multiple technologies and methods are not comparable and the reported sensitivity and specificity range is not meaningful. Future review articles should differentiate the intraneural blood flow measurements and report the diagnostic value for these measurements separately.
Future opportunities also exist in exploring the clinical utility of these measurements. Currently, the reason that intraneural blood flow of the median nerve is altered in CTS patients is unclear. Some studies have theorized that the increase in intraneural blood flow is an early pathologic change of CTS, which can be used for early diagnosis or identification of preclinical CTS patients. The current examination of nerve conduction studies detects the changes in nerve conduction velocities, which is a late pathologic change of nerve demyelination. Thus, by detecting the early signs of median nerve pathology of increased vascularization, Doppler sonography can potentially complement the diagnosis of CTS. In addition, future opportunities exist not only for patients with CTS but also for broader populations, such as in individuals with diabetes who suffer from peripheral neuropathy.
Before the measurements of intraneural blood flow is widely used, multiple additional issues should be considered. First, there is a need to understand factors that might influence the measurements of intraneural blood flow. For example, a link between occupational risk factors, such as force and wrist flexion, and median nerve blood flow has been demonstrated. 36 More studies should be conducted to examine the stability of the measurements of intraneural blood flow under different conditions, such as body temperature, blood pressure, as well as wrist force and positions. Second, the terminology used in the current literature to describe the blood flow within the median nerve requires standardization. Some studies used the word “hypervascularity” to describe the phenomenon when blood flow signals were detected by Doppler ultrasound in healthy subjects, if blood flow should only exist in pathologic median nerves and the existence of blood flow in the median nerve is a sign of pathology. However, this might be problematic when a baseline value for the healthy population has not yet been established. Several studies have identified the blood flow signals within the median nerve in healthy subjects using Doppler ultrasound. In one study, 36% of the median nerves showed the presence of intraneural blood flow detected by power Doppler in an asymptomatic group. 45 However, other studies did not find any intraneural blood flow in the asymptomatic subjects.9,33 More evidence is needed to demonstrate what is the baseline value of intraneural blood flow in the healthy population.
Limitations
This study has several limitations. First, the main focus of this study was to identify, characterize, and compare image acquisition and analysis protocols in the current literature. However, due to the wide variability in study designs and methodologies adopted by the included studies, data synthetization and comparison was precluded. Also, the quality of included studies was not evaluated since data comparison and synthetization were not performed. Thus, the nature of this study inherently has subjective bias. Caution is advised when interpreting the results of the studies discussed in this review.
Conclusion
Doppler sonography has been used to examine the intraneural blood flow of the median nerve mainly related to the topic of CTS. However, no standardized imaging protocol exists, and the wide variety of image acquisition and image analysis methods makes interpretation of any intraneural blood flow findings difficult. This systematic review demonstrated a need for a standardized sonography imaging protocol for examining intraneural blood flow within the median nerve, and a need for the clarification of nomenclature used to describe intraneural blood flow. In addition, this systematic review illuminated an issue in the lack of rigor of the reporting of ultrasound machine settings and imaging protocols. Future studies may be designed to use and compare a combination of sonographic imaging methods described in this review. Future studies are needed to examine the accuracy and reliability of different image acquisition methods and intraneural blood flow measurements. A detailed description of a standardized imaging protocol as well as guidance on how to report the imaging methodologies is warranted. Additional review is also needed to summarize the diagnostic accuracy of different intraneural blood flow measurements in diagnosing median nerve pathologies such as CTS.
Footnotes
Acknowledgements
The authors thank Chen Gong for his contribution in screening titles and abstracts of this systematic review.
Ethics Approval
This study was reviewed and approved by the Institutional Review Board at the University of Southern California.
Informed Consent
Written informed consent was obtained from all subjects before the study.
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because no animals were used during the study.
Trial Registration
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Peer Reviewer Guarantee Statement
The Editor / Associate Editor of JDMS is an author of this article; therefore, the peer review process was managed by alternative members of the Board and the submitting Editor / Associate Editor had no involvement in the decision-making process.