
Abstract
High-resolution sonography is a valuable imaging technique to evaluate scrotal trauma. Scrotal injuries can be caused by both blunt and penetrating forces, causing harm to the testicles and other scrotal contents. This case study follows the diagnosis of a gunshot victim’s testicular injury and how the use of sonography plays a major role in both the diagnosis and surveillance of testicular rupture. The initial sonogram identified mild enlargement and an irregularity of the right testicle. Hemorrhage surrounding the right testicle, soft tissue emphysema, scrotal wall edema, and some echogenic debris and/or a foreign body in the scrotum were also identified. Testicular rupture is a rare but serious injury and prompt medical attention is necessary in such cases to reduce long-term complications, including, but not limited to, infection, disability, and loss of the testicle.
An estimated 327 citizens, in the United States, are shot every day and sustain traumatic or fatal injuries. 1 In the United States, firearm injury is currently the 12th leading cause of death, which is up from its 13th place ranking in 2020. 2 Although generally not life-threatening, traumatic injuries to the scrotum and testis are rare but occur most often after assault by a firearm. 3 A prompt diagnosis and intervention are critical to avoid complications such as infection, infertility, and testicular loss. 3
Diagnostic medical sonography is an imaging technique used to assess a variety of conditions and traumatic injuries affecting the scrotum and testes. In this case study, a rare instance is described, in which a scrotal sonogram revealed evidence of testicular rupture from a gunshot wound. This case study will be put into context by reviewing the existing literature regarding gunshot wounds, in general, as well as the scrotum and testis specifically.
Case Report
A young male presented to the trauma service department, of a level 1 trauma center, in acute distress after sustaining gunshot wounds to the right upper and lower extremities. The patient underwent a computed tomographic angiography (CTA) specific to his upper and lower right extremities, which showed a tibia fracture, tissue swelling, and multiple small, retained bullet fragments. The right scrotal area was partially imaged on the CTA and demonstrates evidence of a small bone fragment, located within the scrotum (see Figure 1).
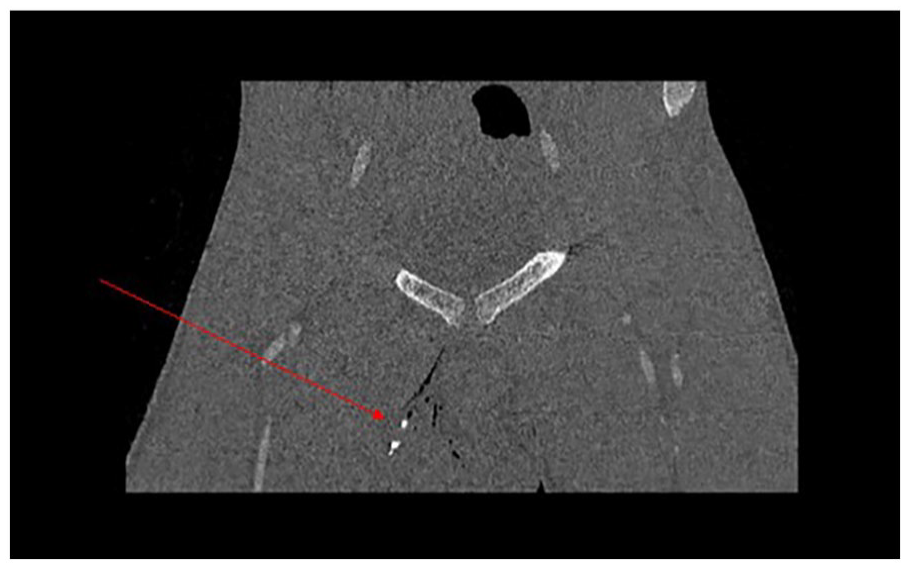
A coronal computed tomographic angiography image is provided, which showed evidence of a small bone fragment located within the scrotum (indicated with a red arrow).
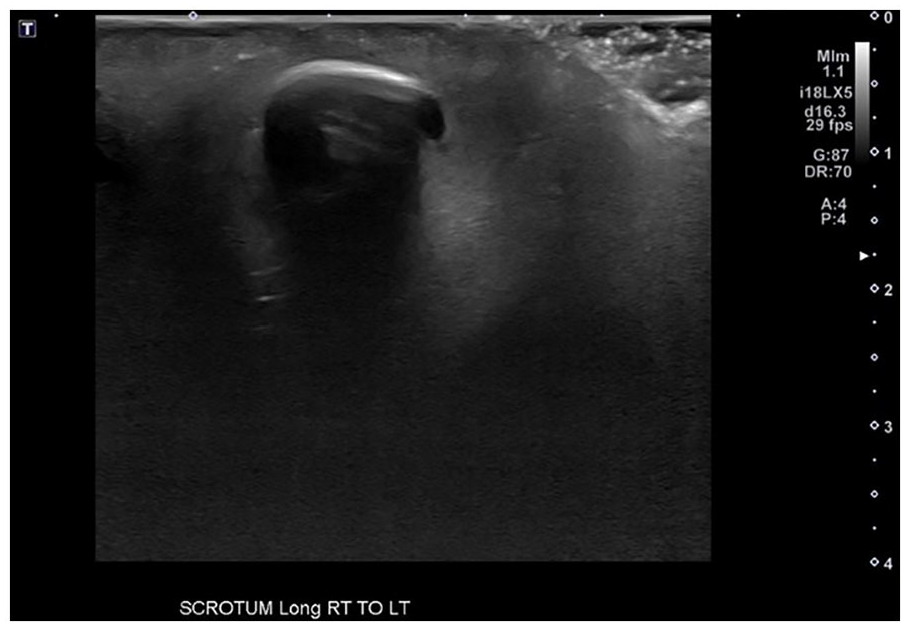
Next, a scrotal sonogram was completed. Multiple grayscale sonographic and color Doppler sonographic images of the scrotum were obtained utilizing an Aplio i800 (Canon Medical Systems, Tustin, California) ultrasound equipment system and a multifrequency i18LX5 linear transducer. The sonogram demonstrated no evidence of an obvious hematoma within the right testicle. However, the right testicle demonstrated an irregular contour (see Figure 2) and was measured to be mildly enlarged when compared with the left testicle. The testicles measured approximately 3.7 cm × 2.6 cm × 3.1 cm on the right and 3.6 cm × 2.2 cm × 2.6 cm on the left.
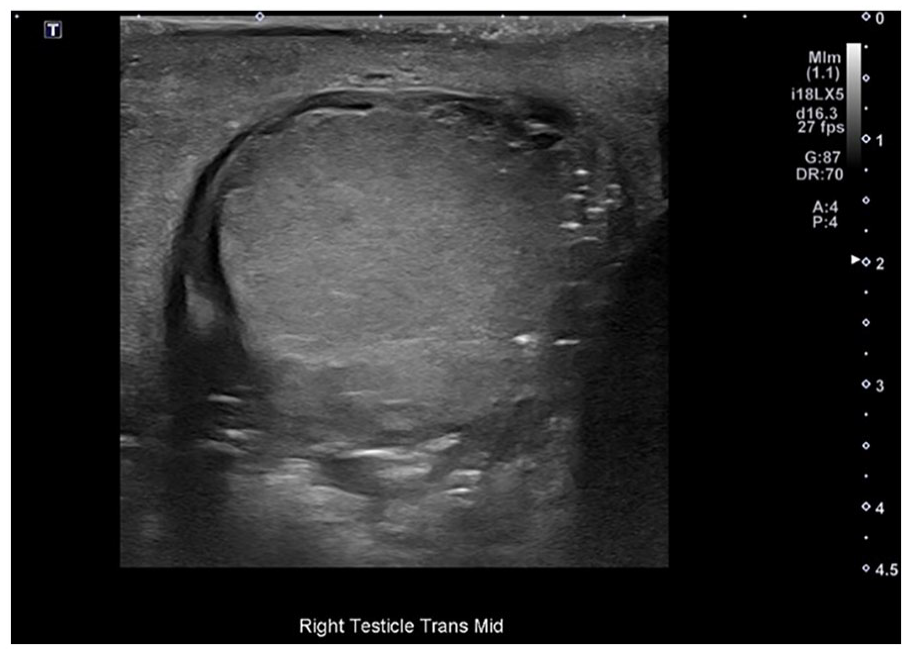
The right testicle is shown as it was imaged in the mid-transverse plane and demonstrated an irregular surface contour.
Both testicles demonstrated arterial and venous flow at the time of the sonogram, with the right testicle showing hypervascularity during color Doppler interrogation (see Figure 3). There was mild hemorrhage surrounding the right testicle as well as scrotal wall edema and soft tissue emphysema (see Figure 4). The sonogram also showed some echogenic debris and/or foreign bodies in the scrotum (see Figure 5). These findings raised concern for acute right testicular injury and the urology department was consulted.
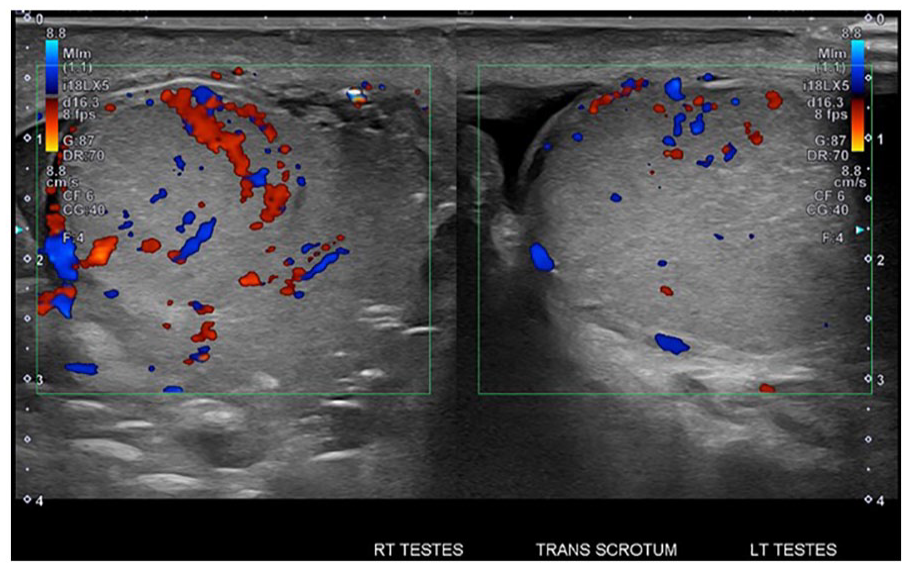
Dual transverse views with color Doppler allow for the comparison of vascularity in the right and left testicles. The right testicle demonstrated hypervascularity during color Doppler interrogation.
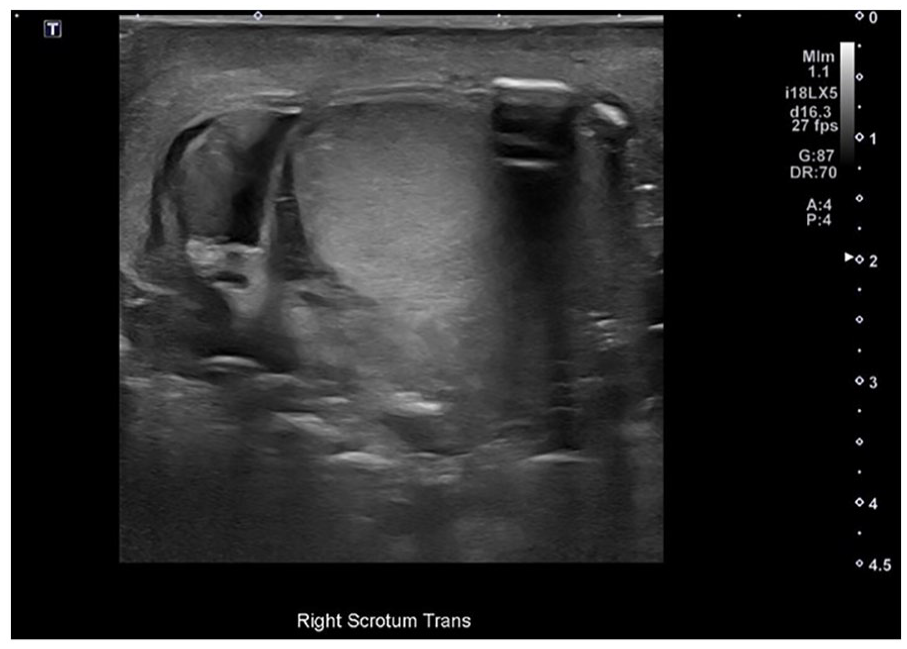
The right testicle was imaged in the transverse plane and showed mild hemorrhage surrounding the right testicle, as well as scrotal wall edema and soft tissue emphysema.
A grayscale sonographic image is provided that demonstrated evidence of a foreign body, within the scrotum.
The patient was assessed by a urologist and found to have a significant scrotal hematoma on the right side that was tender to palpation. The patient was brought to the operating room for emergent exploration surgery of the right scrotum to diagnose between right testicular rupture versus hematoma. Consistent with the sonographic findings, the exploration found significant disruption of the right tunica with extravasation of the testicular contents. The scrotum was copiously irrigated with saline/antibiotic irrigation, the redundant spermatic tissue was excised, and the tunica was sutured closed. Several skin injuries were copiously irrigated and sutured closed as well. The left side of the scrotum palpated healthy and normal and thus not explored surgically.
After approximately 6-week postsurgical intervention, the patient was assessed again with a scrotal sonogram. Unlike the previous acute sonographic finding, of right testicular enlargement, the subsequent examination showed that the right testicle measured smaller than the left. The testicles measured approximately 2.54 cm × 1.66 cm × 2.05 cm on the right (see Figure 6) and 3.53 cm × 1.82 cm × 2.42 cm on the left (see Figure 7). Normal arterial and venous Doppler waveforms were demonstrated in the right testicle. The left testicular images were considered unremarkable.

The right testicle was re-imaged in the sagittal plane, as a follow-up examination and included measurements of the maximum longitudinal and anteroposterior diameter.

The left testicle was re-imaged in the sagittal plane, as a follow-up examination and included measurements of the maximum longitudinal and anteroposterior diameter.
Discussion
The testicles produce sperm and testosterone, which make them a vital component of the male reproductive system. They are housed in the scrotum and are enveloped by a protective structure known as the tunica vaginalis, which is derived from the embryonic process. Each testicle is suspended within the scrotum by a spermatic cord that contains blood vessels, nerves, and the vas deferens, a tube that transports sperm from each testicle. The vas deferens joins with the seminal vesicle to form the ejaculatory duct. The paired ejaculatory ducts pass through the prostate gland, adding secretions from the prostate that are essential for sperm function, and empty into the urethra. 4
Scrotal and testicular injuries are most commonly due to penetrating trauma by firearm and account for < 1% of trauma-related injuries. 3 The patient in this case study underwent emergent exploration surgery due to the concern for acute right testicular injury from a gunshot wound. The utilization of CTA was crucial for assessing the injury and identifying bullet fragments, while scrotal sonogram played a vital role in diagnosing the extent of testicular injury and guiding subsequent management. The surgical intervention on this patient involved copious irrigation, excision of redundant spermatic tissue, and suturing of the tunica vaginalis. Postsurgical surveillance through scrotal sonography demonstrated a decrease in the size of the right testicle, which could be attributed to the resolution of acute trauma-related edema and swelling.
The presented case study detailed testicular trauma that resulted from a gunshot wound and offers a unique contribution to the field of trauma medicine and urology. It also provides insights into the diagnostic approaches for managing such injuries. An extensive search of the literature, within the last 5 years, indicated that while cases involving radiology and gunshot wounds have been documented,5,6 this case study stands out due to its incorporation of multiple diagnostic imaging techniques, surgical intervention, and surveillance, yielding a comprehensive understanding of the injury and its outcomes.
The uniqueness of this case study lies in the integration of CTA and scrotal sonogram to comprehensively evaluate the extent of injury. The initial CTA images revealed not only the ballistic trajectory of the bullets but also partial imaging of the scrotal area, raising concerns for potential scrotal involvement. A subsequent scrotal sonogram played a pivotal role in identifying testicular irregularities, hypervascularity, and the need for immediate surgical exploration. This thorough diagnostic approach distinguishes the current case from other reports, where the extent of scrotal involvement might not have been as rigorously assessed. This approach offers a more holistic view of the injury’s progression, surgical outcomes, and long-term effects.
In comparison with similar cases within recent years, where radiologic imaging was used to assess gunshot wounds, a collective review focused more on the preoperative imaging and immediate surgical interventions, without including the postoperative follow-up. The utilization of both sonography preoperatively and as a subsequent follow-up evaluation was another unique aspect of this case study.
A comparable case study published by Kadouri et al, detailed how scrotal gunshot injuries were managed with computed tomography (CT) and surgical intervention, without detailed sonographic imaging preoperative or postoperative. 7 The outcomes were reported in terms of surgical success, with no mention of subsequent size changes. In contrast, the current case study approach included not only immediate intervention but also detailed assessments of testicular size and preservation of arterial and venous flow. This diagnostic surveillance enhances our understanding of the functional outcomes and potential complications, from these types of injuries.
This case study does have several limitations that should be noted. First, the bone fragment that was noted on the CTA was not documented in either the surgical or follow-up report. It is possible that the bone fragment was removed via irrigation during the surgery; however, this was not specifically noted. Second, the patient did not receive a CT of the scrotum, which may have allowed for further insight into the injury. In addition, this case only focused on a single patient, so further research with larger sample sizes is needed to provide more definitive evidence for the management of scrotal gunshot wounds. Finally, there is limited existing literature regarding scrotal gunshot wounds specifically; as such, more research into this area is warranted to better understand treatment options and outcomes for these types of injuries.
Conclusion
This case study stands out in its comprehensive evaluation of testicular trauma resulting from a gunshot wound, employing both sonography and CTA, surgical intervention, and a diagnostic follow-up assessment. Early and thorough scrotal exploration is recommended by the American Urological Association in all patients suspected of testicular rupture to prevent infection, chronic pain, testicular loss, infertility, and altered self-image. 8 The uniqueness of this case contributes to our understanding of testicular trauma management by highlighting the importance of combining diagnostic imaging techniques and provides insights into postoperative outcomes.
Footnotes
Ethics Approval
The SIUC Institutional Review Board has reviewed this project and determined it does not meet the regulatory definition of human subjects’ research at 45 CFR 46.102.
Informed Consent
Informed consent was not sought for the present study because all case data were de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors Shannon Anderson and Amy Bro are JDMS Article Reviewers.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.