
Abstract
Sarcomas are characterized by innumerable clinical presentations. Sarcoma tumors involving peripheral vessels are quite rare and not always easy to identify despite the availability of diagnostic tools such as sonography, computed tomography (CT), and magnetic resonance imaging (MRI). This case report discusses the imaging findings of angiography, sonography, and CT, which were the modalities used in this case. Initially, the patient underwent limited duplex ultrasound and CT imaging to evaluate a painful right groin area after right common femoral artery (CFA) angioplasty and laser atherectomy, with left groin access. Sonographic findings demonstrated a large, heterogenous, hypoechoic, and avascular mass surrounding the right CFA. CT imaging of the pelvis described a partially thrombosed pseudoaneurysm surrounding the CFA. Surgical evacuation of what was believed to be a hematoma was performed; a pathology report revealed sarcoma of the groin.
A 52-year-old African American man presented to the office complaining of right thigh and calf pain for the past year that had worsened in the past month. Medical history pertinent to peripheral arterial disease included diabetes mellitus, hypertension, hypercholesteremia, and previous smoking. Previous hernia repair of the right groin performed a couple of years prior was also noted. The patient initially presented with a lower extremity arterial duplex sonography report performed two weeks earlier at an outside facility. The report described a focal common femoral artery (CFA) high-grade stenosis with monophasic waveforms throughout; no images were available. The patient underwent laser atherectomy and balloon angioplasty of the right CFA with left groin access one week later. The patient presented to the office two weeks after his arterial intervention describing increased pain in the right thigh and groin after returning to work two days earlier. A limited right groin sonogram was performed using a GE Logiq P5 ultrasound machine and a L9 linear transducer (GE Healthcare, Waukesha, Wisconsin). Sonographic findings showed a patent CFA artery with persistent elevated velocities of 239 cm/s (Figure 1). A large heterogeneous, hypoechoic, and avascular structure with homogeneous borders was identified. It measured approximately 3.5 × 2.6 cm transversally and 3.0 longitudinally, suggesting a possible hematoma. The patient was recommended to continue warm compresses to the right thigh and groin and return for a two-week follow-up. A repeat arterial duplex sonogram of the CFA performed upon the patient’s return showed an unchanged heterogeneous, hypoechoic, avascular mass surrounding the CFA. A computed tomogram (CT) of the pelvis was ordered to further evaluate the mass and was performed at a different facility six weeks after the initial arterial intervention. The CT showed a large collection surrounding the right CFA, which was reported as a thrombosed pseudoaneurysm (PSA) measuring 3.6 × 3.7 × 3.5 cm. The patient had a second arterial procedure two weeks after the CT to address the persistent stenosis and potentially treat the partially thrombosed PSA and possible leak with a covered stent. No PSA or leak was found, and the patient had angioplasty at the stenosis site. One week after his second angioplasty, the decision was made to take the patient for surgical hematoma evacuation. Right groin exploratory surgery was performed, including a biopsy of the right groin mass, which was diagnosed as high-grade pleomorphic sarcoma.
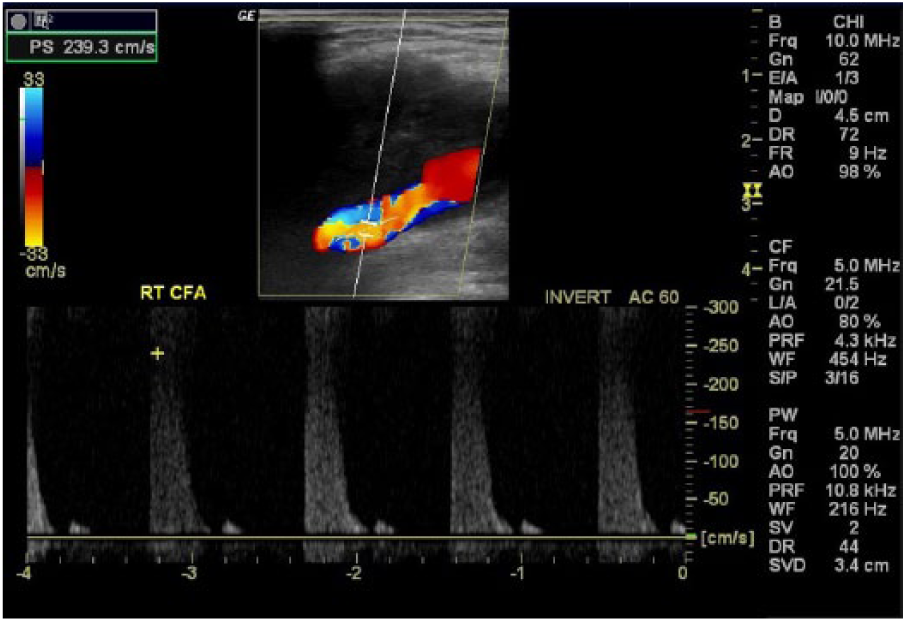
Longitudinal color and spectral Doppler image shows high-velocity and turbulent flow in the common femoral artery. No flow is seen within the adjacent mass.
Discussion
Sarcoma tumors constitute a rare and heterogeneous group of malignant tumors that originate from connective tissues embryologically derived from the mesenchyme.1,2 Sarcomas of large vessels usually present in the pulmonary arteries, aorta, and inferior vena cava. 3 Sarcomas in the peripheral arteries are extremely rare, and most peripheral arterial sarcomas are leiomyosarcomas or angiosarcomas. 3 However, more than 50 different subtypes of soft tissue sarcoma have been identified. 2 In the United States, sarcomas account for about 1% of all malignancies. 2 According to the literature, tumor involvement with an adjacent blood vessel may happen in 5% to 10% of cases. 2
Color duplex sonography, CT, and formal angiography have all been used in the diagnosis of soft tissue sarcoma involving vascular structures. 2 Magnetic resonance imaging (MRI) is considered the gold standard in imaging soft tissue sarcomas and should be used when malignant lesions are suspected. 2 In this particular case, the patient did not undergo MRI evaluation. The radiologic characteristics of sarcoma tumors and hematomas under color duplex sonography, CT, and angiography are discussed.
Sonography
Sonography is a readily available, noninvasive, inexpensive modality that can be used to initially determine cystic versus solid nature in soft tissue masses. In this case, the patient had an initial limited arterial duplex sonogram to evaluate a painful groin after an endovascular procedure. The arterial duplex sonogram showed a heterogeneous, mostly hypoechoic and avascular mass with homogeneous borders. The patient underwent a previous angioplasty procedure to address a suspected stenosis of the right CFA. Arterial access for the previous angioplasty was through the contralateral left groin; however, the patient’s symptoms were on the right side, which was not as easy to explain. The patient’s postprocedural pain was reported to be right sided rather than left sided. If a postprocedural hematoma were to develop, it would typically develop at or near the site of arterial access, which in this case was the left side. Hematomas may occur as a complication of peripheral endovascular procedures; the literature suggests an overall incidence of about 4.5%. The use of ultrasound guidance CFA access during peripheral vascular interventions (PVIs) may help reduce the rate of groin hematomas. 4 The possibility that a hematoma could have developed due to a small arterial injury at the site of treatment could not be completely excluded. Sonographic characteristics of a perivascular hematoma include the presence of a soft tissue mass with varying echogenicities adjacent to the artery 5 with little to no color or spectral Doppler seen. 5
Sonographic characteristics that may be present in malignant tumors include sizes greater than 5 cm, infiltrated margins, and a disorganized chaotic hyperemic pattern. 6 Most lesions are large at presentation, with sonographic features of varying echogenicity, composition, and degree of hyperemia that are mostly nonspecific. 6 While many sonographic characteristics in soft tissue masses may suggest malignancy, they may also appear in benign masses. Sonography alone cannot confirm malignancy and needs to be used in tandem with other imaging modalities. Figure 1 demonstrates a color and spectral Doppler longitudinal image of the right CFA at the area of stenosis and adjacent mass without internal color flow. Figure 2 shows a color duplex transverse image of the right groin avascular mass next to the artery. Note the absence of color flow within the mass or its periphery. Special attention should be placed on the color scale setting to be sensitive enough to detect microcirculation. In this particular image, the color scale setting may have been set too high to detect vascularity. However, angiographic imaging showed no flow within the mass. Figure 3 shows a gray-scale image of the right CFA and heterogeneous mass in longitudinal view.
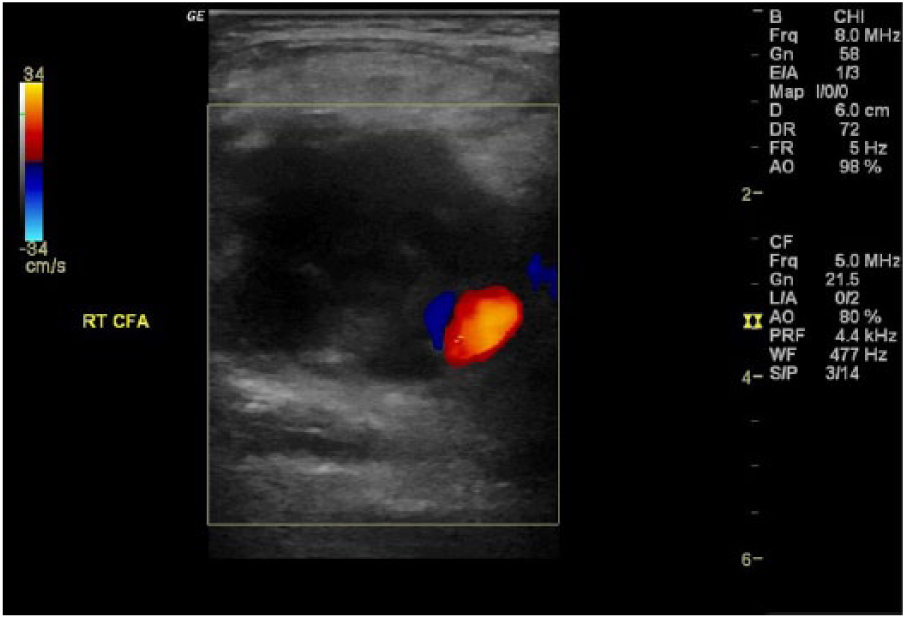
Color Doppler transverse image of right common femoral artery shows a hypoechoic avascular mass.
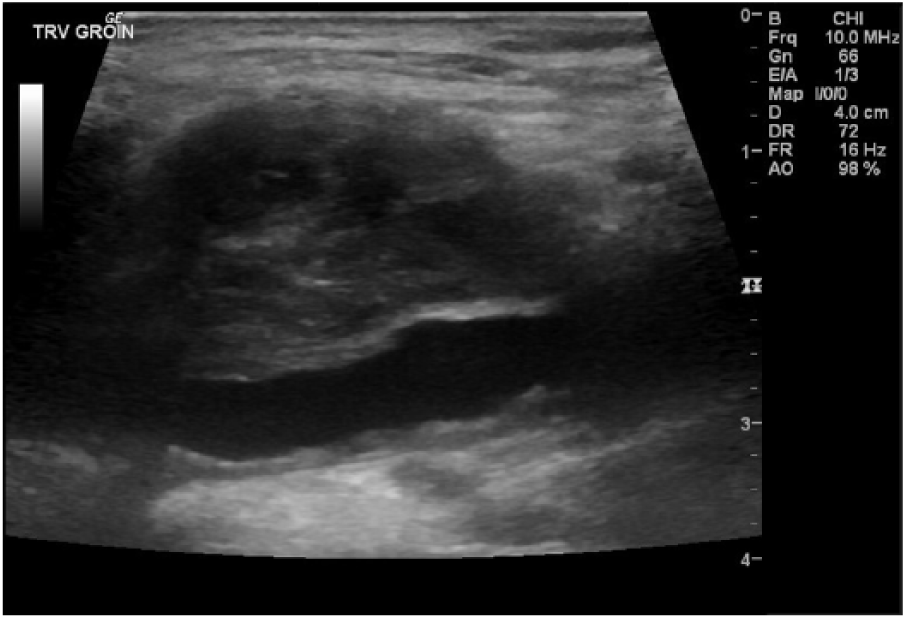
Longitudinal gray-scale image of the right common femoral artery and heterogeneous mass.
Computed Tomography
CT is also a widely available imaging modality that can be used to evaluate soft tissue masses. CT is used in cases where there is a contraindication for MRI or where CT may be better at delineating areas of periosteal bone formation, microcalcifications, and cortical destruction. 7 CT is a faster examination compared to MRI, and it may be better tolerated by claustrophobic patients due to the use of more confined space with MRI. There are limitations and contraindications such as ionizing radiation exposure, contrast reactions, and cost. CT alone cannot diagnose malignancy. As with the other imaging modalities, CT also has overlapping characteristics in malignant and benign masses and needs to be used in conjunction with other modalities such as MRI for further characterization of masses by providing additional tissue detail. A pelvic CT scan was ordered for our patient for further evaluation. According to the CT report, a groin collection surrounding the CFA measured 3.6 × 3.7 × 3.5 cm and was diagnosed as a thrombosed pseudoaneurysm. No pelvic lymphadenopathy was seen, and severe narrowing of the CFA was noted.
Regarding soft tissue hematomas, CT provides great anatomical detail and high diagnostic accuracy in detection, quantification, and localization of hematomas in different locations. 8 Contrast-enhanced CT can also be useful in the detection and further evaluation of active bleeding from a ruptured site. 9 Sarcomas appear hypodense to isodense in comparison to surrounding musculature on CT. 10 CT angiography of the lower extremities helps in the evaluation of masses and associated arteries as well as identification of the tumor’s origin and surgical planning. 7 According to Subhawong et al., 11 CT imaging can provide useful clues for the characterization of soft tissue tumors; they describe four distinguishing CT characteristics that include mineralization pattern, lesion density, bone involvement, vascular malformations, and/or vascular involvement.
Angiography
Conventional contrast angiography is regarded as the standard diagnostic modality for peripheral arterial disease (PAD) of the lower extremity. 12 Risks involved with angiography include radiation exposure, arterial puncture, and contrast nephropathy. 12 Initially, the patient presented with an abnormal arterial duplex from a different facility; based on those results, he underwent angiography to treat a hemodynamically significant stenosis of the right CFA. Angiography was useful to identify a high-grade stenosis in the artery, but the mass was not visualized as it was avascular (Figure 4). Angiography may also be helpful at delineating feeding arteries and overall tumor vascularity for potential treatment. The typical chaotic vascularized or hypervascularization pattern seen in most sarcomas was not present in this case. Under angiography, vascularized tumors show a “blush” caused by feeding vessels; unless a mass is vascularized, it will not be seen. Figure 4 shows a severe stenosis in the CFA; no tumor “blush” or tumor vascularity is appreciated.

Angiographic image of right common femoral artery stenosis.
Conclusion
Soft tissue sarcomas may present with imaging characteristics similar to hematomas under different imaging modalities. Radiologic characteristics may overlap between benign and malignant findings in all modalities; therefore, more than one imaging modality should be used when suspicious soft tissue masses are present. No one imaging modality alone can diagnose malignancy, and a pathological evaluation is needed to reach a true diagnosis of malignancy. The case presented was evaluated with angiography, CT, and sonography; their radiologic characteristics and findings as well as limitations were discussed. A patient’s symptoms and clinical presentation are paramount in avoiding misdiagnoses, as seen initially in this case report.
Footnotes
Acknowledgements
Special thanks to Professor T. Stearns at Adventist University of Health Sciences for her feedback and guidance in the completion of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.