
Abstract
Objective:
To establish normative data on the width of the acromioclavicular (AC) joint space using sonography, based on a selected Nigerian cohort without any shoulder injury or pathology.
Materials and Methods:
A cross-sectional study was conducted on the normal AC joints of randomly selected Nigerians. A sonographer performed the examination and obtained all the width measurements of AC joint space, using a GE LOGIQP6 ultrasound system and a multiple-frequency linear transducer.
Results:
The width of the AC joint space was equal on both sides, measuring 5.6 ± 1.2 mm for the right and 5.6 ± 1.2 mm for the left (P = .701). The mean width of both joint spaces differed between men and women, with the men having a wider space (P < .05). Age had a strong negative predictive relationship, with the AC joint space width and both joint spaces decreasing with age (P < .001). Weight and body mass index had weak negative predictive relationships with both joint space widths (P < .001). Participant height had a very weak positive predictive relationship with both joint space widths (P < .05).
Conclusion:
Normative data on the width of the AC joint space, in a randomly selected Nigerian cohort, are provided and may be clinically useful in the ongoing sonographic assessment of the AC joint.
The acromioclavicular joint (AC joint) is a plane synovial joint formed by the lateral end of the clavicle and the acromion process of the scapula. 1 This joint is an integral part of the shoulder girdle. The shoulder girdle connects the upper extremity to the axial skeleton and works in concert to coordinate the movements of the upper extremity. 2 The acromial end of the clavicle articulates with the acromion of the scapula. The joint is reinforced by a capsule with a synovial lining consisting of an intrinsic fibrocartilaginous disk between the wedge-shaped articular surfaces of the bone. The AC joint disk is continuous with the capsule to cushion the joint and to correct for bone incongruences; however, the disk is very prone to degeneration. 3 Thus, the AC joint may undergo degenerative changes with age and function.
The AC joint has an intra-articular synovium and an articular surface. The joint is characterized by various angles of inclination in the sagittal and coronal planes, and by a disk. 4 Two types of disks have been observed. They are a complete disk, which is rare, and a meniscoid-like disk.5,6 With age, the articular disk between the clavicular and acromial end degenerates. After the age of 40 years, the disk undergoes significant degeneration but remains mostly asymptomatic. 7 The joint gradually narrows as the disk wears away because of the frequent use of the shoulder joint.
The function of the AC joint is to allow the scapula additional degrees of rotation on the thorax. 8 The joint serves as a link between the shoulder girdle and the axial skeleton and facilitates both gliding and rotational movements. 9 It particularly serves as a coordinating link between the scapulothoracic, glenohumeral, and sternoclavicular joints and allows for physiological movement. 10 The function of the AC joint may be hampered by trauma, pathological processes, and age-related narrowing that result in pain and reduced movement. The AC joint is frequently injured in traumas, affecting the shoulder girdle. About 10% of acute injuries to the shoulder girdle affect the AC joint, with joint separation accounting for 40% of injuries to the shoulder girdle in athletes. 11 Mazzocca et al 12 estimated that AC joint injuries can be as great as 9% of all shoulder injuries. The injuries mostly affect men involved in athletics, heavy manual workers, and military and paramilitary personnel.13 –16
The investigation of AC joints in this locality is mostly done by radiography, but musculoskeletal sonography could replace radiographs, as the facilities and expertise become more available. High-resolution sonography can reveal joint space splaying, offset, or joint space narrowing and bone–bone contact. Sonography is an effective diagnostic workup for lesions of coracoclavicular ligaments in the acute phase of AC injuries. 17 In addition to assessing joint alignment and integrity of the ligaments, sonography is economical and readily available in most locations. It is also a nonionizing radiation technique, easy to perform on patients, and has multiplanar imaging capability. 18 The real-time nature of sonography ensures that it can be used to identify the source of shoulder pain during a dynamic study. 19
The grading of traumatic injuries of AC joints is based on the extent of the widening of joint spaces and the extent of ligament injury. 20 Comparison of the joint space on the injured side with the uninjured contralateral side is also used to diagnose abnormal widening of AC joint space. Osteoarthritis of the AC joint is a pathological condition affecting the joint. It may occur due to prior trauma 21 or due to long-term degenerative disorder often coexisting with subacromial impingement. 16 The AC joint pathology, such as osteoarthritis, can be diagnosed during a sonogram of the shoulder girdle. Degenerative pathologies of the AC joint manifest on a sonogram as cortical irregularities or osteophytes, usually accompanied by intra-articular hypoechoic fluid displacing the joint capsule and joint space narrowing.22 –24
Sonography has become established as a diagnostic tool in musculoskeletal imaging because the targeted structures are superficial. 19 To effectively deploy sonography in the assessment of AC joint space size in a particular patient population, a range of normal values of the width of the AC joint space that is specific to that group is needed. There are no sonographically derived data on the AC joint space width that would apply to a Nigerian patient population. Therefore, this study was designed to establish normative data on the width of the AC joint space, using sonography in a selected cohort of Nigerians without any shoulder injury or pathology.
Materials and Methods
Subjects
A cross-sectional study targeting healthy individuals with normal AC joints was conducted in the ultrasound department of Esteem Diagnostic Medical Services Limited, Lagos, Nigeria, from June to December 2021. A minimum sample size of 384 subjects was calculated for the study, using the formula for estimating sample size for studies of unknown populations. 25

where,
n = the desired minimum sample size
Zα = significance level of 95% level (Zα = 1.96)
p = proportion of the population with similar attributes under study = 50% (0.5)
d = the margin of error tolerated or absolute error = 5% (0.05)
q = 1 – p = 1 – 0.5 = 0.5
A simple random sampling technique using a ballot system was used to select the participants who would be invited to the study from a pool of volunteers attending the imaging center. The words “yes” and “no” were written on an equal number of pieces of paper, folded, and thoroughly scrambled. Each volunteer was asked to pick one paper blindly. Participants selecting an affirmative ballot were included in the study and those who did not were excused. The volunteers included in the study satisfied the following inclusion criteria:
Must be at least 18 years old.
Must be healthy, without a history of shoulder injury or pathology.
Should be able to stand without external support for up to 15 minutes.
Was not pregnant at the time of the study.
Data and Image Collection
Ethical approval of the research design and protocol was obtained from the research ethics committee of the Faculty of Health Sciences and Technology, Nnamdi Azikiwe University, Awka, Nnewi Campus, before the commencement of data collection. Each subject consented to participate in the study before enlistment.
A Seca Mod-220 CEO123/2013 body mass index (BMI) Seca 769 digital personal height and weight scale was used to measure the height and weight of the subjects. Each consenting subject wore minimal apparel, was barefoot, and stood erect in the Frankfurt position without external support for the height and weight measurement. The age of each subject was obtained by direct questioning of the date of birth.
The LOGIQP6 ultrasound equipment system (GE HealthCare, Waukesha, WI, USA) was fitted with a multiple-frequency (6–15 MHz) linear transducer, This system was used to obtain the images of the right and left AC joints and measure the joint space in each subject. Each subject sat erect with the arms in an anatomical position. Acoustic coupling gel was applied liberally on each shoulder and examined individually. The ultrasound beam was directed vertically downward perpendicular to the tendon fibers to minimize anisotropy, which causes the tendon to appear artifactually hypoechoic. The choice of frequency was determined by the sonographer based on a subject’s size. The frequency used on the average-sized patients was 10 MHz, while 9 MHz was used on those who were larger. A longitudinal sonographic view was obtained to demonstrate the acromion, clavicle, and AC joint space (Figure 1). The joint space was recognized as a transonic area between the reflective lateral end of the clavicle and the acromion, and measured on the right and left sides. The measurements were carried out on a freeze-frame, with a diagnostically representative image (Figure 1).
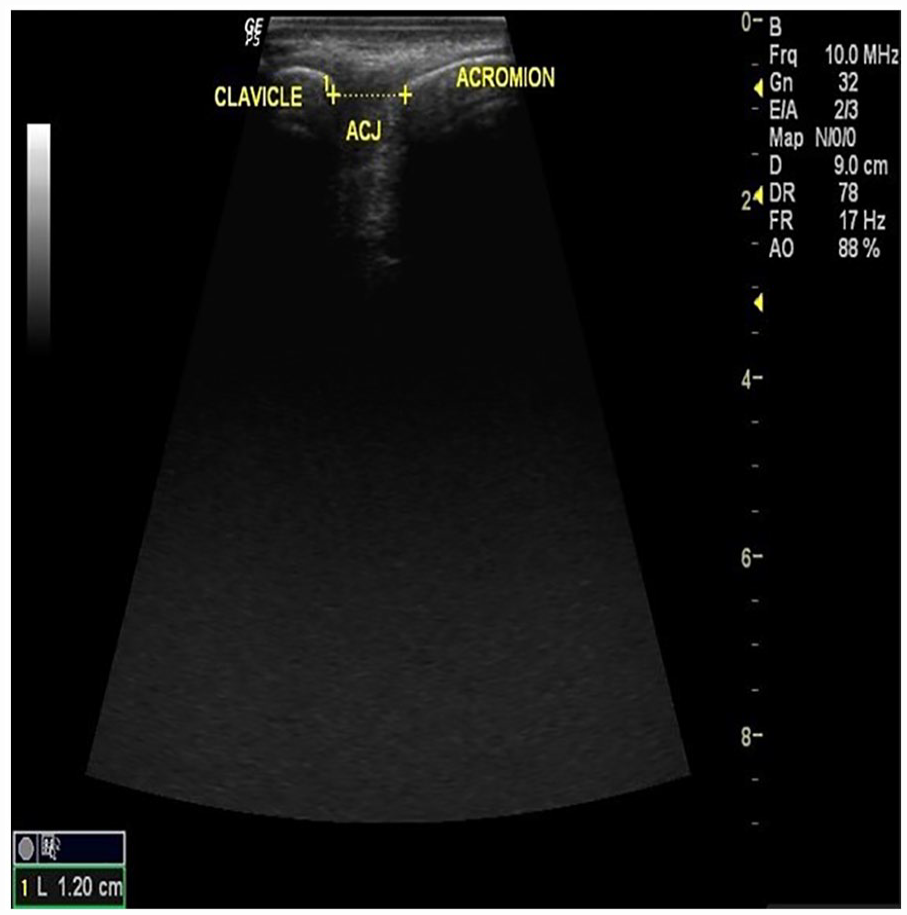
Sonographic recognition and measurement of acromioclavicular joint space. The joint space is represented by the separation between the electronic calipers (+ . . . +).
A single sonographer, with 15 years of clinical experience in musculoskeletal and high-resolution sonography, performed the examinations and obtained all the measurements of the AC joint spaces. To ensure the reliability of the technique and measurements, satisfactory intra-observer and interobserver reproducibility were obtained in a pilot study before the data collection commenced.
Data Analysis
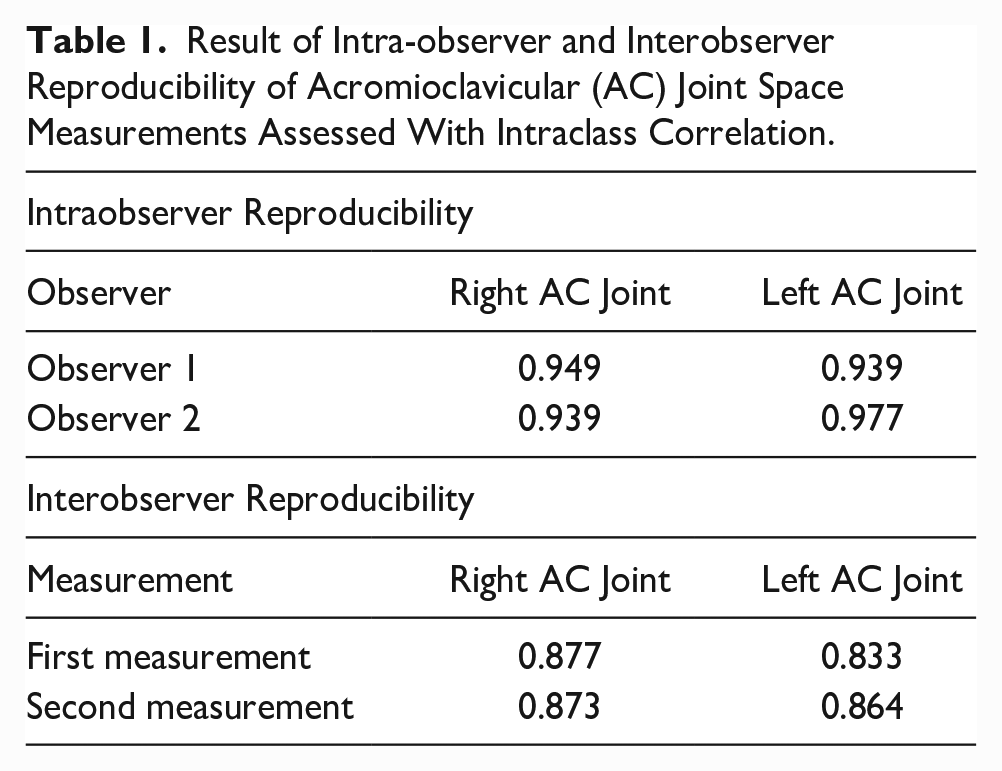
Interobserver reproducibility between the sonographer and a more experienced sonographer was assessed. Intra-observer reproducibility with the 2 sonographers was also assessed. Both assessments were carried out using intraclass correlation (ICC) analysis.
The BMI was calculated for each participant from the height and weight measurements, using the following formula:

The data collected from the main study were then categorized according to sex and age, and analyzed using MedCal Statistical Software Version 20.110 (MedCalc Software Limited, Ostend, Belgium; https://www.medicalc.org; 2022). Summary statistics for the age and anthropometric characteristics of the subjects were expressed as mean ± standard deviation and median values were inserted as all variables were non-normal in distribution according to the Shapiro–Wilk test for normal distribution. Non-normal distribution of a variable was confirmed if the P value for the Shapiro–Wilk test statistic was less than or equal to .05. The box-and-whisker plots of the variable distributions were also inspected to confirm their non-normal distribution.
The means of the age and anthropometric characteristics of the males and females were compared using the independent samples t-test and Mann-Whitney test. The mean of AC joint space width on both sides in all the subjects irrespective of age and sex were compared using paired samples t-test. Cohen’s d effect size was used to express the practical significance of relationships between variables. Cohen’s d effect size was interpreted as d=0.2 (small), d=0.5 (medium), and d=0.8 (large) in line with Cohen’s benchmarks. 26 The Kendall rank correlation coefficient (τ) was used to determine the relationship between the width of the AC joint space, age, and anthropometric variables. Predictive relationships between the width of the AC joint space on both sides, age, height, weight, and BMI were all investigated using linear regression. Statistical significance was established a priori at P < .05.
Results
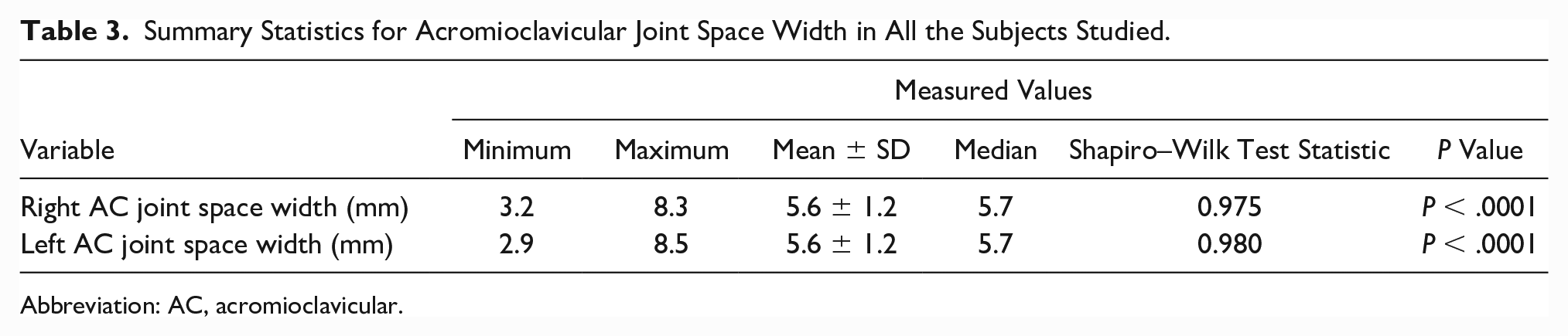
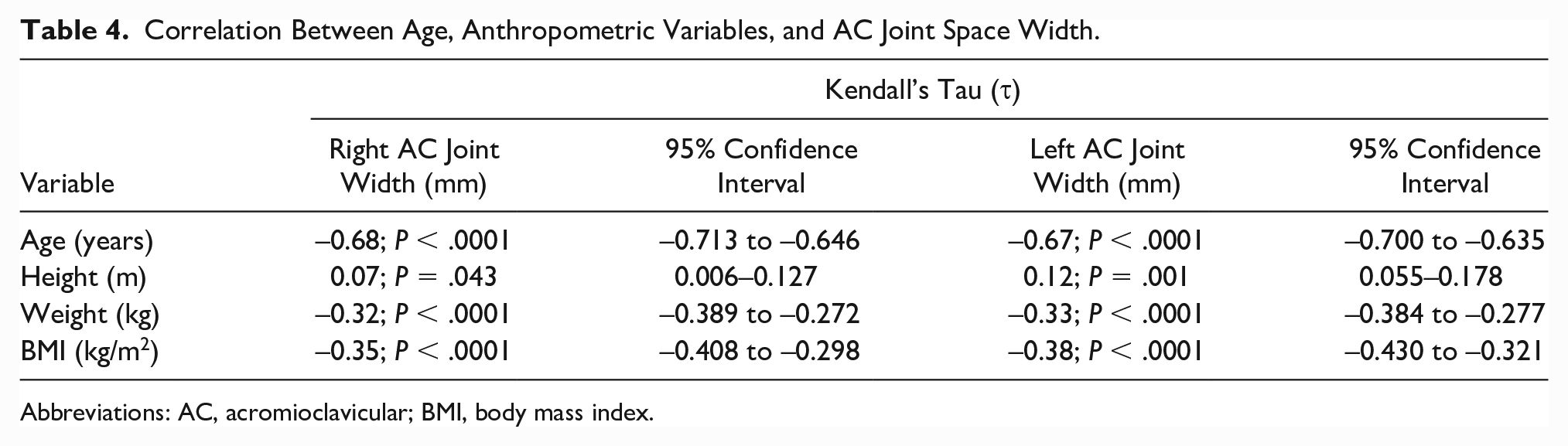
The data provided in Table 1 demonstrate a satisfactory intra-observer and interobserver reproducibility that was obtained during the pilot study, prior to the beginning of the main study. The age and anthropometric characteristics of the subjects are provided (Table 2). There was a significant difference between the mean ages of the men and women (26.7 ± 7.8 years vs 28.3 ± 7.8 years; P = .049). However, the difference was of no practical significance as Cohen’s d was calculated at 0.195 (95% confidence interval [CI], 0.311–0.335). There were no differences in the mean values of height, weight, and BMI between the men and women. Table 2 and Figure 2 both demonstrate that the data collected were non-normal in distribution. Table 3 shows the means of the width of the right and left AC joint spaces width across all the subjects. There was no difference in the means of the width of the right and left AC joint spaces (5.6 ± 1.2 mm vs 5.6 ± 1.2; P = .701). The Cohen’s d effect size was small (0.010; 95% CI, –0.051 to 0.054). The correlation between age and anthropometric variables and the width of the AC joint spaces is provided (Table 4). There was a moderate negative correlation between age and AC joint space width on both sides (τ=–.68; P < .0001; 95% CI, –0.713 to –0.646 for the right, and τ=–.67; P < .0001; 95% CI, –0.700 to –0.635 for the left). There was no correlation between height, weight, and BMI, and the width of the AC joint spaces, bilaterally (P > .05).
Result of Intra-observer and Interobserver Reproducibility of Acromioclavicular (AC) Joint Space Measurements Assessed With Intraclass Correlation.
Summary Statistics for the Subjects’ Age and Anthropometric Characteristics.
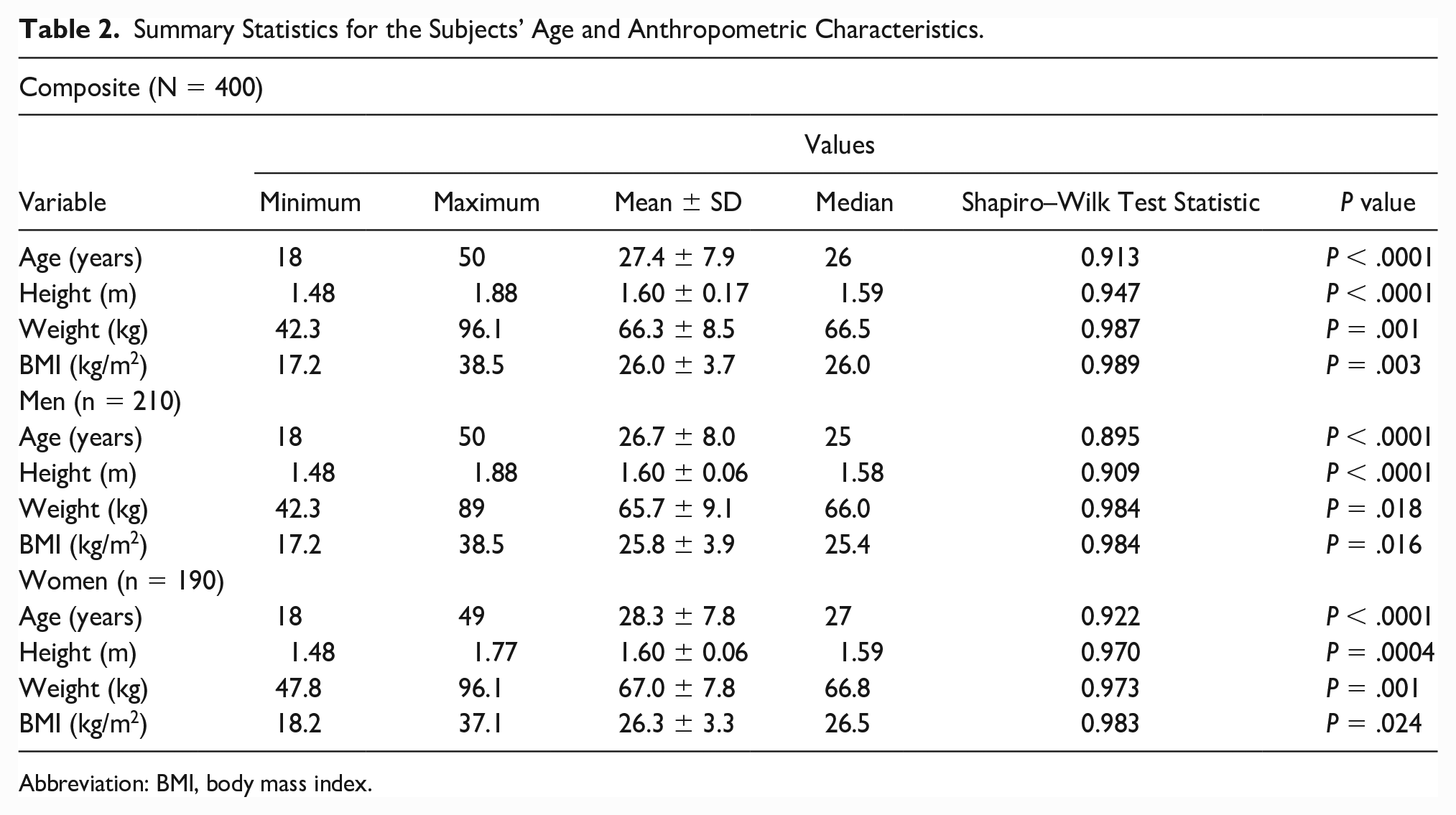
Abbreviation: BMI, body mass index.
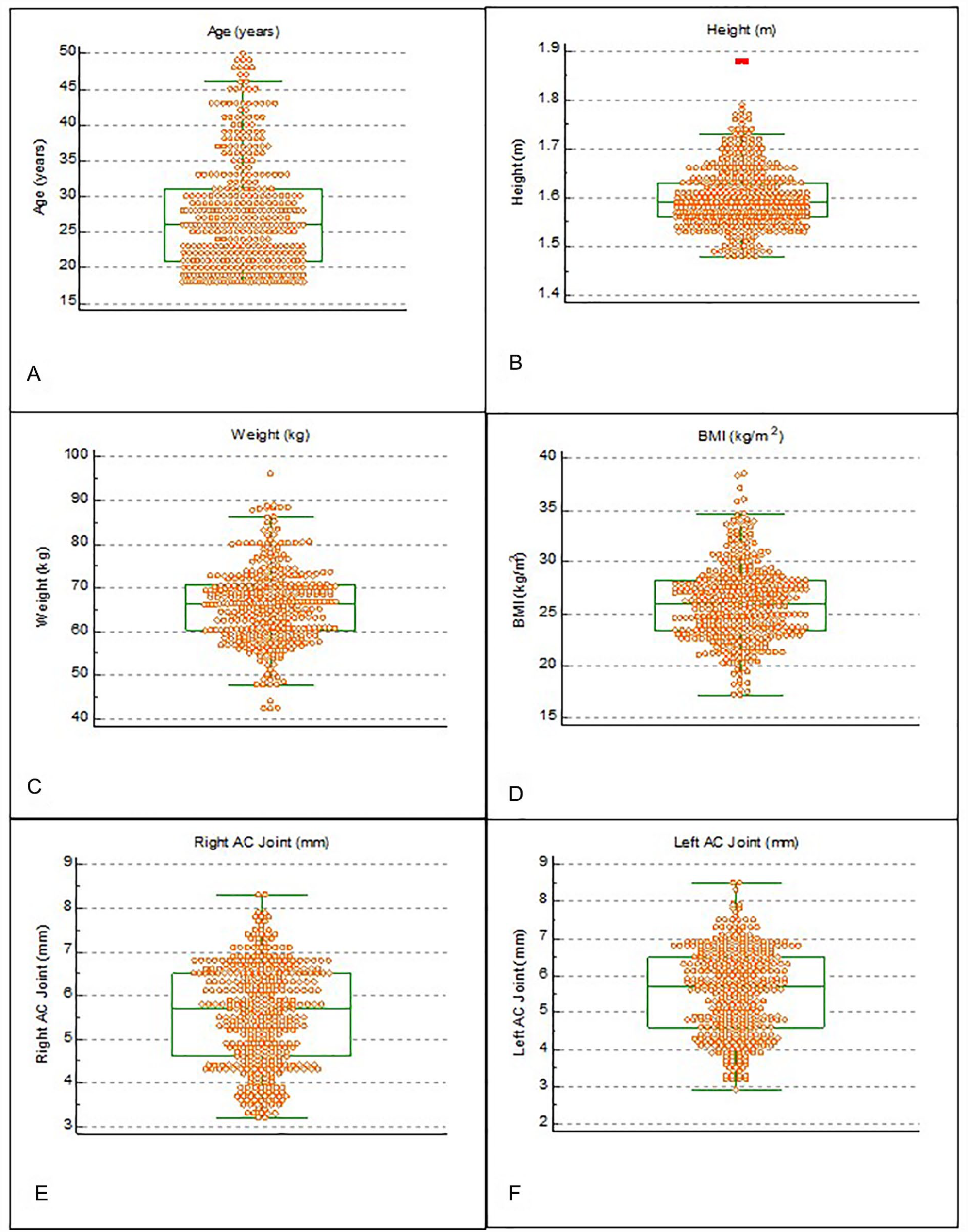
Box-and-whisker plots illustrating the distribution of: (a) the age, (b) height, (c) weight, (d) BMI (e) right AC joint width, and (f) left AC joint width, of the participants.
Summary Statistics for Acromioclavicular Joint Space Width in All the Subjects Studied.
Abbreviation: AC, acromioclavicular.
Correlation Between Age, Anthropometric Variables, and AC Joint Space Width.
Abbreviations: AC, acromioclavicular; BMI, body mass index.
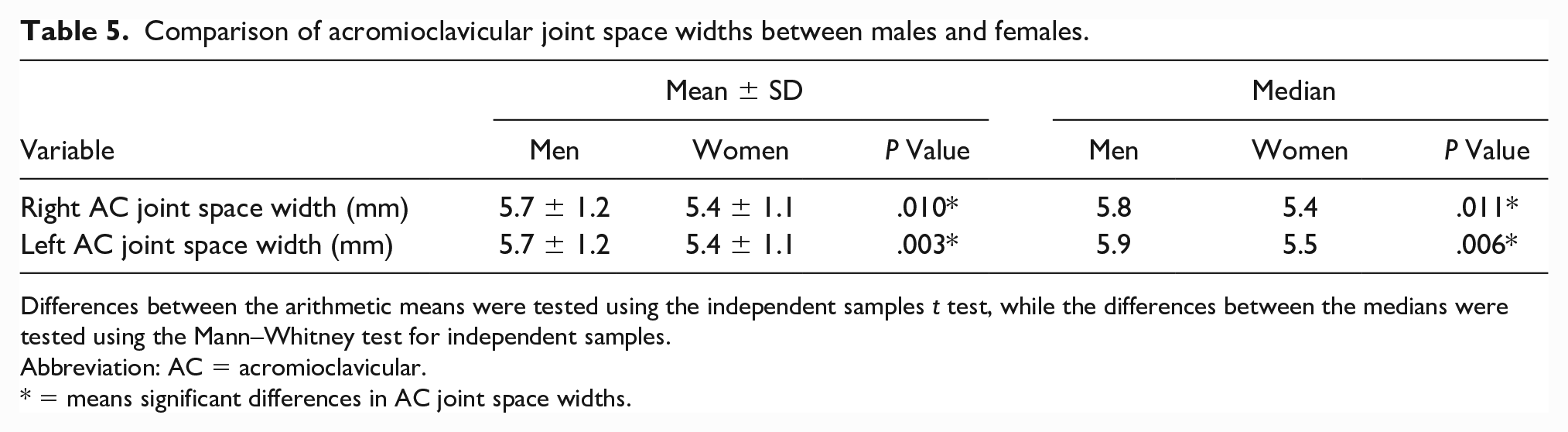
The mean width of the width of the right AC joint space differed significantly between men and women, with the men having a wider space as shown in Table 5 (P = .01). Similarly, the mean width of the left AC joint differed significantly between men and women, with the men having a wider space as shown in Table 5 (P = .003). The Cohen’s d effect sizes for the differences between male and female AC joint space widths were near moderate (d=0.264, 95% CI, 0.168–0.168 for the right and d=0.311, 95% CI, 0.184–0.164 for the left).
Comparison of acromioclavicular joint space widths between males and females.
Differences between the arithmetic means were tested using the independent samples t test, while the differences between the medians were tested using the Mann–Whitney test for independent samples.
Abbreviation: AC = acromioclavicular.
= means significant differences in AC joint space widths.
The following predictive relationships were established between the widths of the AC joint spaces (dependent variable) and anthropometric parameters (independent variables):
Relationship with age (years):

Relationship with height (m):
Relationship with weight (kg):
Relationship with BMI (kg/m2):
NB: y = dependent variable (AC joint width) and x = independent variable (age, height, weight, and BMI)
The participant’s age showed a strong negative predictive relationship with the width of the AC joint spaces, with both joint spaces decreasing with age as shown in Figure 3 (P < .001). Weight and BMI had weak negative predictive relationships with both the width of the AC joint spaces (P < .001; Figure 3). Height had a very weak positive predictive relationship with the right AC joint width (P = .025) and the left AC joint width (P = .005; Figure 4).
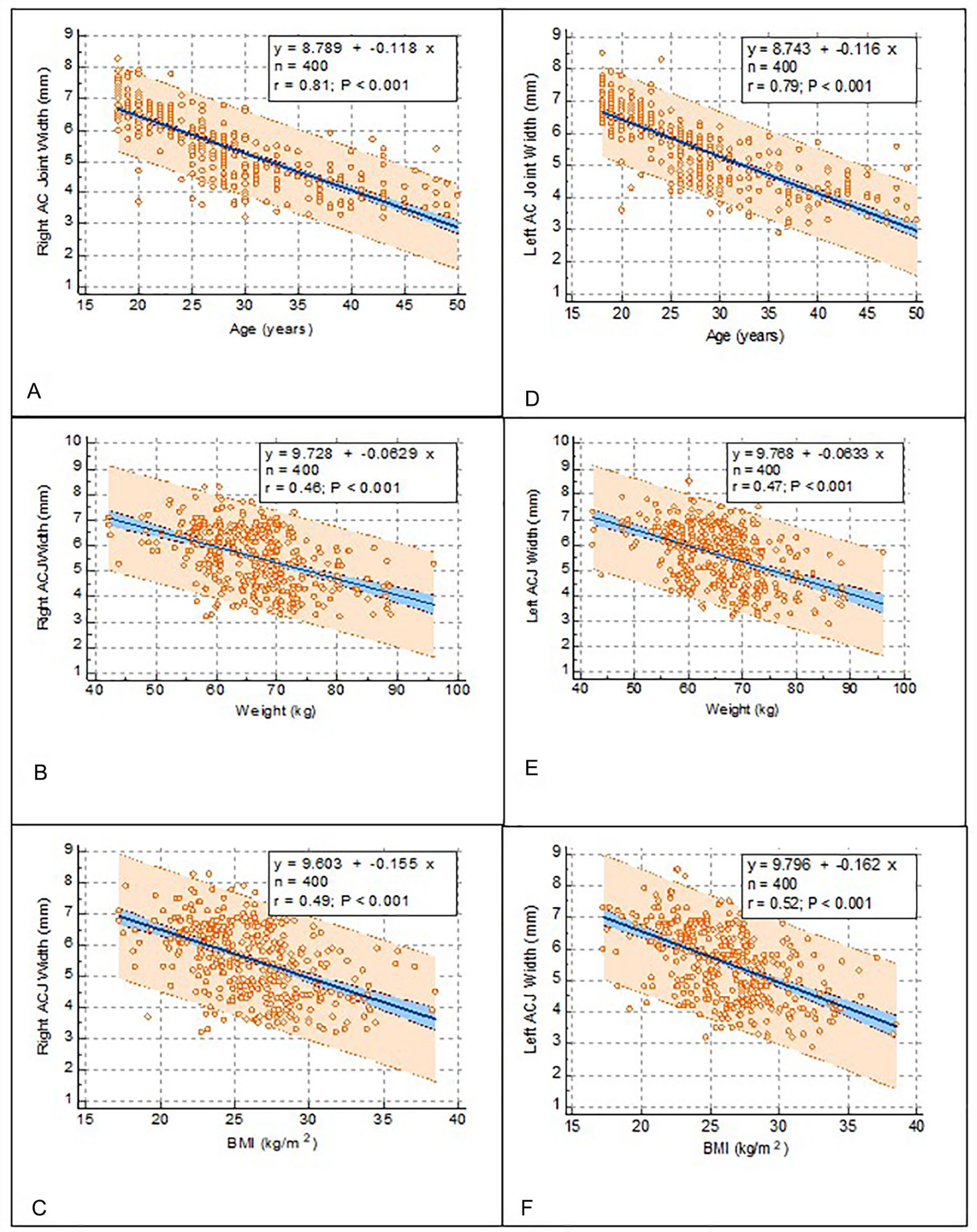
Linear regression graphs of the right AC joint space width with: (a) age, (b) weight, (c) BMI, and the left AC joint space width with: (d) age, (e) weight, and (f) BMI, of the participants.
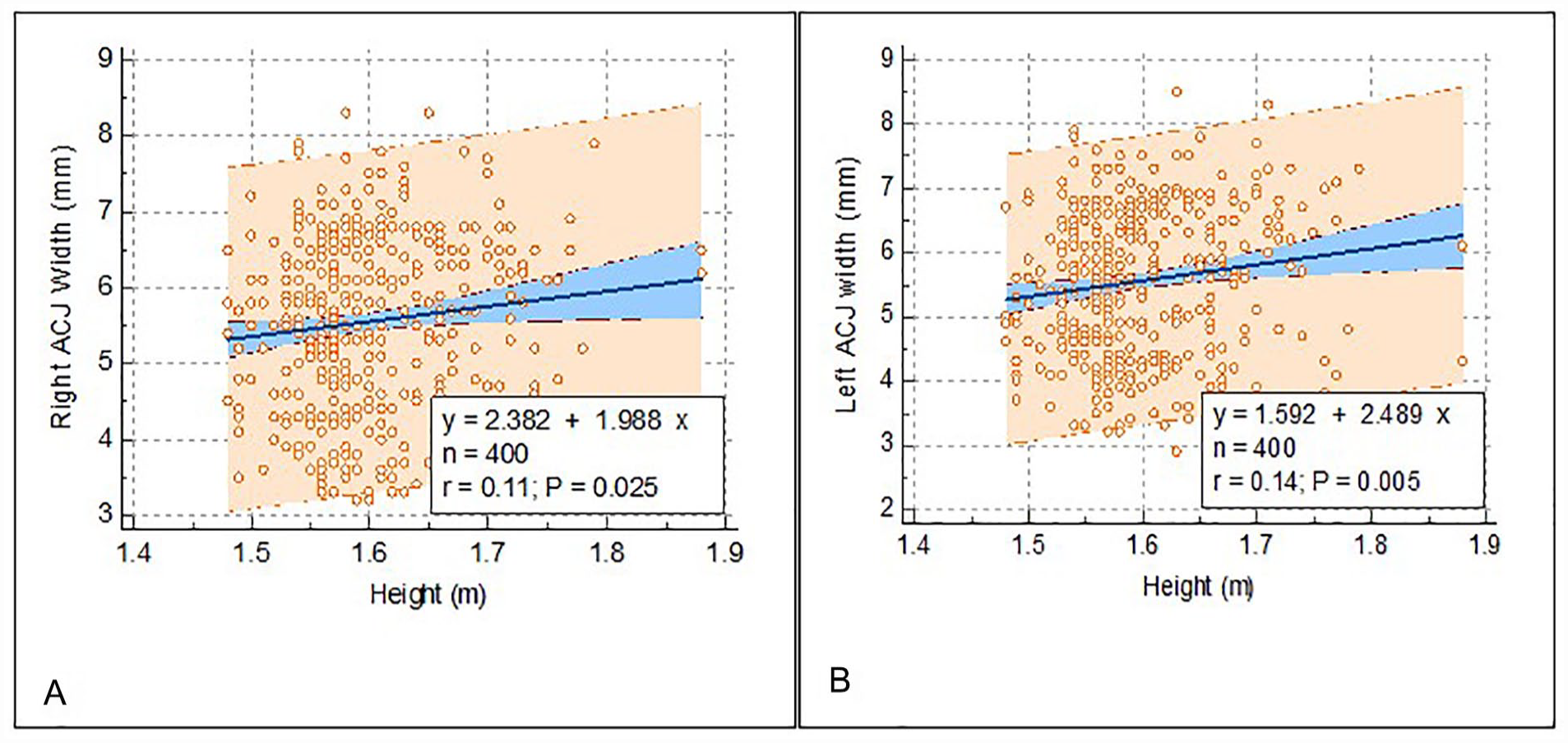
Linear regression graphs of (A) the right acromioclavicular (AC) joint space width and (B) the left AC joint space width, with the height of the participants.
Discussion
The AC joint is a part of the shoulder girdle, a complex structure that connects the upper extremity to the axial skeleton and works in concert to coordinate the movement of the upper extremity, ensuring fluid arm motion.2,9 The joint is multiaxial and allows movements in 3 degrees of freedom, namely, pronation-retraction, elevation-depression, and axial rotation. The movement at the joint is entirely passive as there are no muscles that attach to it directly. The function of the acromioclavicular joint may be hampered by a pathological process or trauma and therefore would require ultrasound evaluation to assess the degree of disease or injury.
This study was designed to provide normative data on sonographically measured normal AC joint space based on a Nigerian patient population. The study was undertaken because of a lack of reference values to make diagnostic decisions as pathological processes or injuries cause diminution or splaying of the joint. Sonography has the advantage of demonstrating soft tissue injuries, which a radiograph may not be able to demonstrate as well as osseous details of the joint.
A total of 800 AC joint spaces, based on 400 Nigerian adults with apparently normal shoulders, were measured in the study. The result showed that the mean width of AC joint space was 5.6 ± 1.2 mm for the right and 5.6 ± 1.2 mm for the left. The results also demonstrated that the widths of the right and left AC joint spaces are equal. This may suggest that in any examination of the AC joints, for pathology or injury, the contralateral side should be examined for comparison. The mean width of the AC joint spaces on the right and left obtained from a similar sonographic study in the adult Sudanese population was 5.01 ± 0.61 mm. 27 A sonographic cadaveric study also reported a significantly smaller width for the AC joint space. 28 The smaller width of AC joint space may be attributed to changes occurring post mortem. The study equally noted a significant difference between the sonography measured AC joint width and an anatomically determined width. 28 This may be a result of the imprecision associated with imaging as no diagnostic imaging technique can replicate the exact anatomic details of the body. This limitation should always be taken into consideration whenever interpreting a musculoskeletal sonogram.
This study’s results also showed that the mean width of the AC joint spaces on the right and left sides were equal across all the subjects aged between 18 and 50 years. The approach to determining separately the normal width of the AC joint space on the right and left was to check for differences in width, between the sides in a healthy state. Previous researchers in this area of research had averaged the widths, of the joint spaces, bilaterally.27,28 The implication of equality of the joint spaces on both sides is that during assessment for injury or pathology dissimilar sizes can be confirmatory of an abnormality. Given the equality of the width of the AC joints, between the sides, it is proposed that a comparison of the painful and non-painful shoulders should be undertaken, especially in individuals aged between 18 and 50 years with an AC joint injury or suspected pathology.
There were significant differences between the widths of the AC joint spaces between men and women. The men had a wider joint space and this may be attributed to their propensity for engaging in manual labor that required movement of the joints, in the shoulder girdle. It is important to take note of these sex differences during an assessment of the AC joint. The result of this study also revealed a significant progressive decrease in the width of the AC joint on both sides with age. The results of this study are in agreement with the findings in previous studies.7,29 –31 The implication of progressive narrowing with age is degenerative arthropathy with resultant reduced movement and pain. Hence, older persons are more likely to be diagnosed with AC joint diseases. The result of the study showed that body height alone was not a significant influence on the width of the AC joint space. However, body weight and BMI were found to significantly influence the width of the AC joint space. With the BMI having an influence on the width of the AC joint space, the height by implication is indirectly involved since BMI is derived from body weight and height.
Limitations
The main limitation to this cohort study was the research design and purposive participants who were included. Random selection was a strength of the work; however, the sample size would need to be increased to be properly generalized to a population. Nevertheless, this work is important in the global use of sonography to evaluate diverse patient populations and specifically for the width of the AC joints.
Conclusion
In summary, this study provided normative data on the width of the AC joint space, utilizing sonography, based on a selected cohort of Nigerians. The data may be helpful in the sonographic assessment of the shoulder and the AC joint in particular. Larger studies and comparison with other ethnic groups would further enhance this line of inquiry and translate to clinical practice.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of the article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval was obtained from the Research Ethics Committee of Faculty of Health Sciences and Technology of Nnamdi Azikiwe University before the commencement of data collection.
Informed Consent
Informed consent was not sought for the present study because all case data were de-identified and/or aggregated and followed ethics committee or institutional review board (IRB) guidelines (also referred to as the Honest Broker System).
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study.
Trial Registration
Not applicable.