
Abstract
Objective
To investigate the role of acromioclavicular joint morphology in the presence of subacromial erosion after hook plate fixation.
Methods
We retrospectively analyzed the clinical data of 36 patients (17 men, 19 women; mean age, 48.7 years; range, 21–76 years) treated with hook plate fixation for distal clavicular fractures (n = 20) or acromioclavicular joint dislocation (n = 16) from August 2011 to March 2013. The patients were divided into two groups: the subacromial erosion group (18 patients) and the normal group (18 patients). Differences in multiple anatomical parameters between the two groups were measured and compared.
Results
The distal clavicle–acromion angle was significantly larger in the subacromial erosion group (mean, 51.37° ± 5.59°) than in the normal group (mean, 44.20° ± 3.83°), as was the distal clavicle–coronal angle (mean, 25.44° ± 2.51° vs. 21.67° ± 4.06°, respectively). The thickness of the acromion was significantly different between men and women (9.72 ± 1.13 vs. 8.16 ± 1.89 mm, respectively).
Conclusion
The results of this study indicate that the distal clavicle–acromion angle and distal clavicle–coronal angle are closely correlated with the occurrence of subacromial erosion after hook plate fixation.
Keywords
Introduction
The hook plate has been used to treat distal clavicular fractures and acromioclavicular joint dislocations. 1 However, the literature has revealed the existence of certain complications after hook plate fixation, such as acromion impingement syndrome, subacromial erosions, and heterotopic ossification. 2 These applications have a negative impact on the final outcome of distal clavicular fractures and acromioclavicular joint dislocations. Some authors 3 have found that impingement of the hook against the rotator cuff caused omalgia because of inappropriate hook plate placement on the clavicle and acromion. However, the relationship between the morphology of the acromioclavicular joint and complications such as subacromial erosions remains unclear.
We believe that mismatch among the plate, distal clavicle, and acromion is specifically caused by the complex morphology of the acromioclavicular joint. To elucidate the relationships among these structures, we studied the anatomical morphology of the acromioclavicular joint by three-dimensional morphological analysis in patients treated with internal fixation using a clavicular hook plate. Specifically, we evaluated subacromial erosions caused by the hook plate.
Materials and methods
We analyzed the clinical and radiographic data of 16 patients with acromioclavicular dislocations and 20 patients with a distal clavicular fractures treated with internal fixation using a clavicular hook plate from August 2011 to March 2013. Approval from the Human Research Ethics Institutional Board was obtained for this study.
Patients with acromioclavicular dislocation were classified according to the Rockwood classification. 4 Distal fractures were assessed according to the Neer type classification. 5 All patients underwent open reduction and internal fixation without reconstruction of the coracoclavicular ligament. The duration of time until removal of the internal fixation device ranged from 6 to 16 months (mean, 11 months). Before removal, computed tomography (CT) scans of the shoulder with a slice thickness of 1 mm were obtained after all patients provided written informed consent for participation in the study. The diagnostic basis of subacromial erosion is the appearance of a bright belt around the tip of the hook. In patients without subacromial erosion, no bright belt is present around the tip on CT images (Figure 1; the bright belt in the red box represents subacromial erosion). The CT data were maintained in Digital Imaging and Communications in Medicine format.

Subacromial erosion (represented by bright belt in the red box).
Data acquisition and processing
The model was established in four steps.
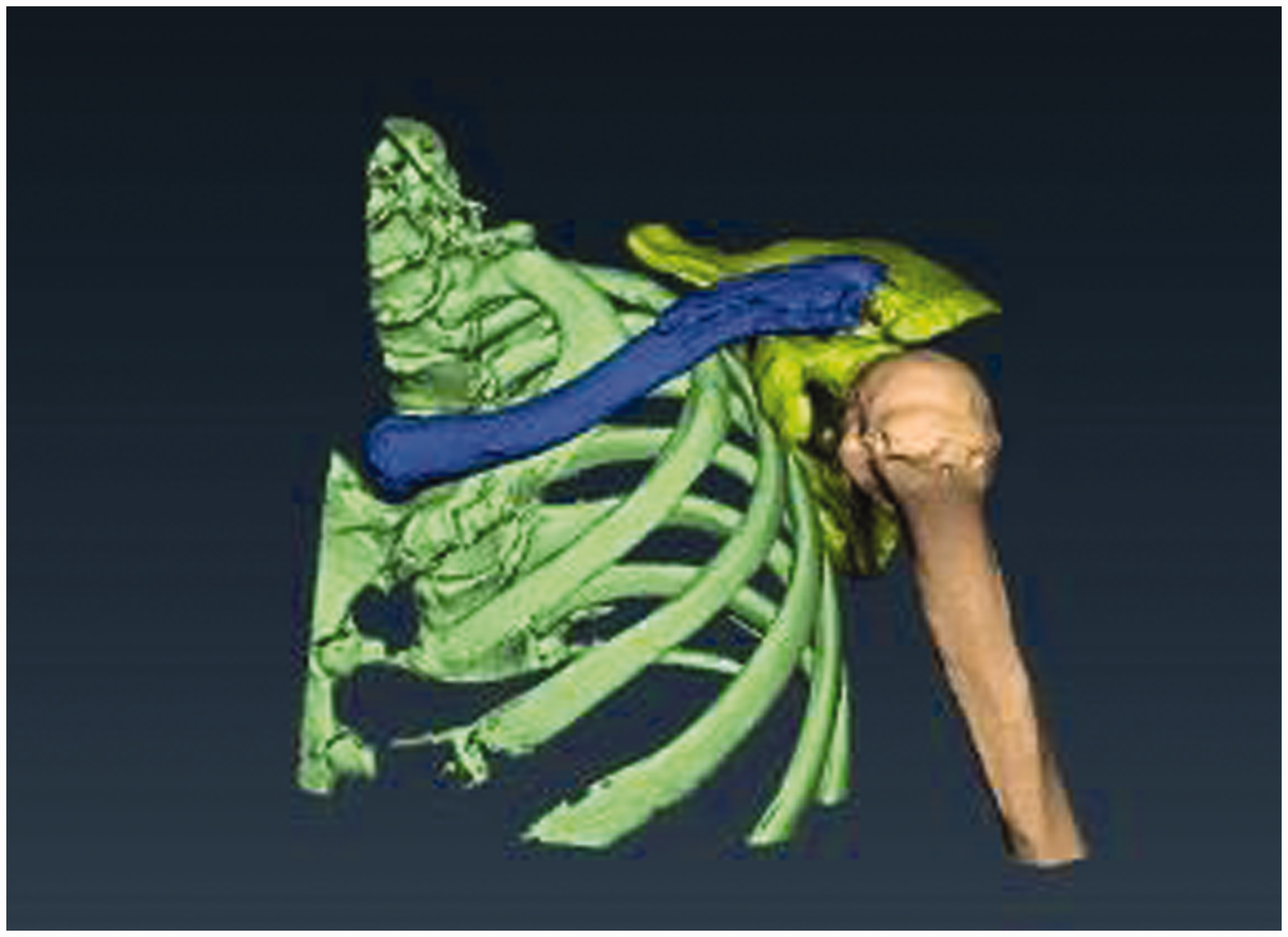
Step 1: Multilayer stack CT reconstruction of the data was performed using Mimics software (Materialise Mimics, version 10.01; Materialise, Leuven, Belgium). Step 2: Mimics software was used for image segmentation, gray-threshold processing, multi-layer editing, obtaining the three-dimensional (3D) point cloud format and the basic outline of the characteristic line, and obtaining the data format “.iges.” Step 3: Point clouds and contours were imported into the CATIA software environment for editing and patching. Block processing into sheet features was then performed to obtain computer-aided design data in “.iges” format (CATIA, version 5 R19; Dassault Systèmes SA, Vélizy-Villacoublay, France). Step 4: The computer-aided design data were imported into the ANSA software environment, cleaning up the model geometry and designing a discrete, finite element mesh model as shown in Figure 2 (ANSA version 13.0.1 software; BETA CAE Systems SA, Thessaloniki, Greece). Three-dimensional polygonal model of the clavicle and scapula after reconstruction
Measurements of morphological parameters
To measure the distal clavicle–coronal angle, we started by determining the surface. However, this was difficult because the surface of the clavicle is irregular. After reconstructing the CT data to fit the 3D model, we evaluated the horizontal plane in the building model first and then adjusted the horizontal plane until it appeared as a level, straight line. This maneuver ensured that the clavicle was seen in the same plane.
Distal clavicle–coronal angle
The distal clavicle–coronal angle was measured as the angle between the distal clavicle and the coronal plane. In this plane of the building model (as above), nearly two-thirds of the clavicle was in a relatively flat plane, fitted first to the central axis of the clavicle and then to the distal clavicular slope. The axial plane and the inclined plane angle were then measured (Figure 3).
Distal clavicle–coronal angle (α)
Acromion sagittal angle
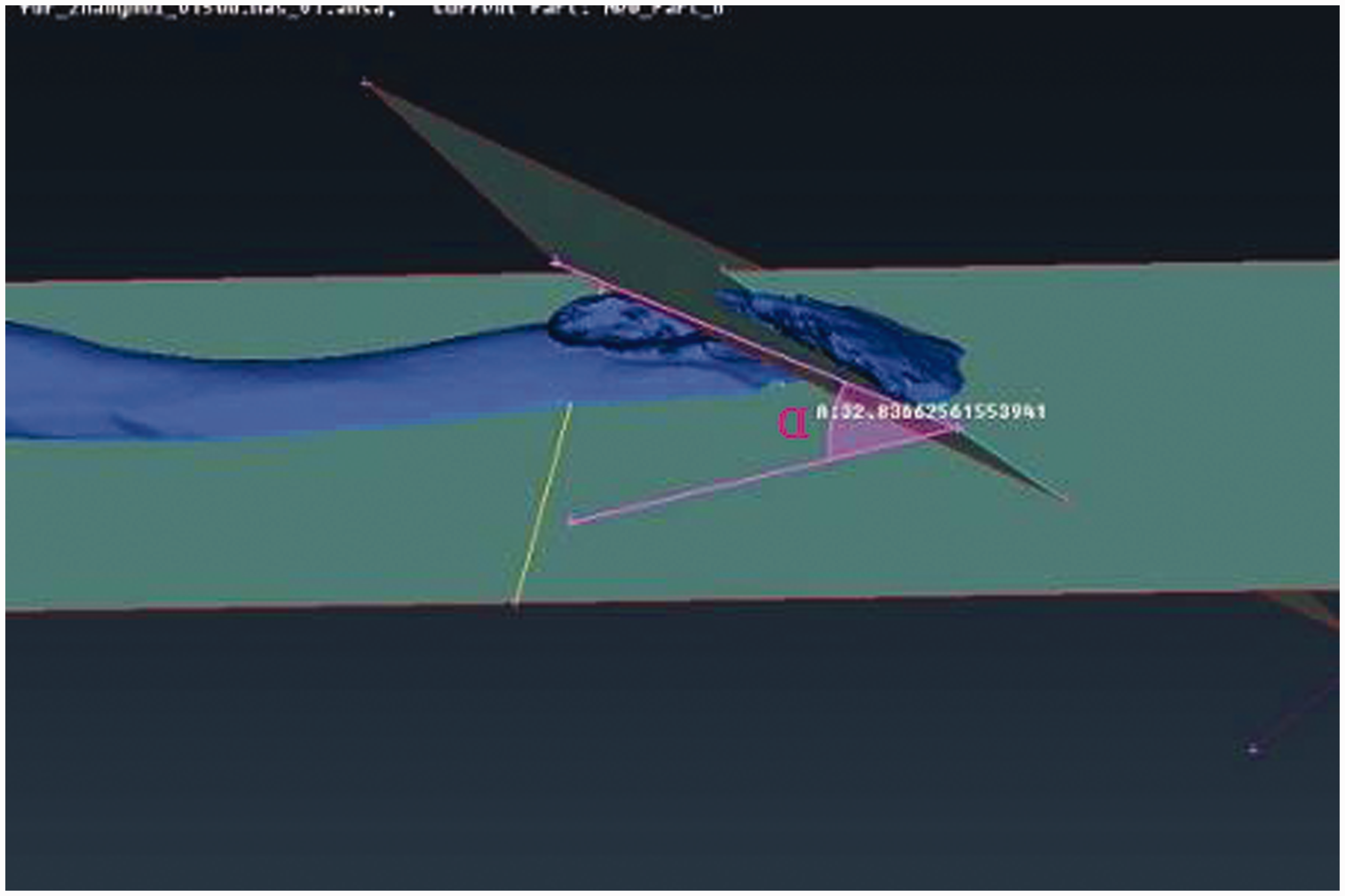
The acromion sagittal angle was measured as the incline angle of the lower surface of the acromion in the sagittal plane. To determine the acromion sagittal angle, we noted that the undersurface of the acromion was curved or appeared as an inverted triangle in the reconstruction model. The angle was chosen from the highest point of the acromion, after which we defined the minimum angle (i.e., the acromion sagittal angle) (Figures 4 and 5).

Acromion sagittal angle in the three-dimensional polygonal model (β)
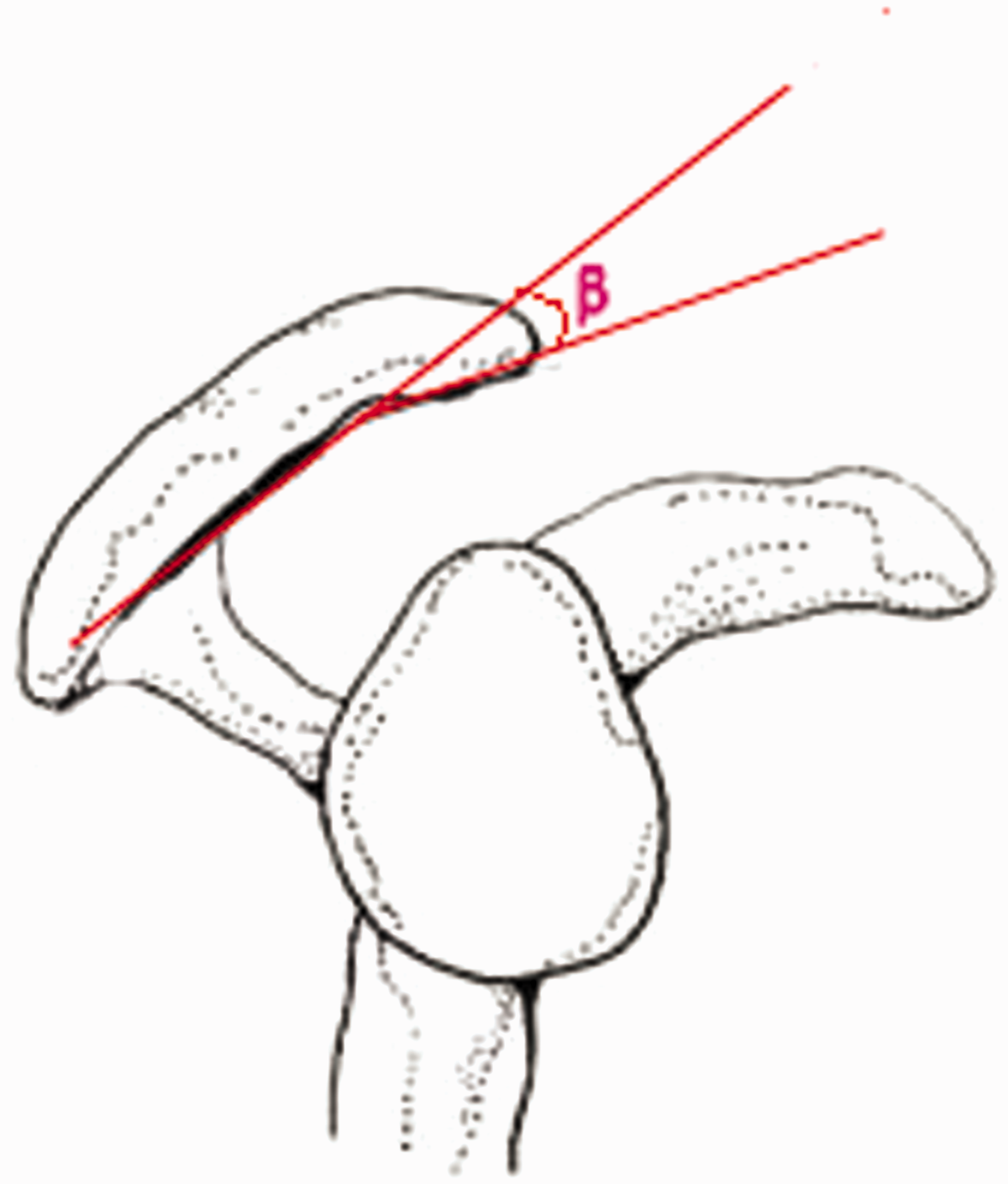
Acromion sagittal angle in pattern diagrams (β)
Acromion thickness and width
The width and thickness of the acromion were measured in the coronal plane where the tip of the hook plate contacted the acromion. The measurements of the width and thickness on the cross section showed the movement of the clavicular hook tip even more directly (Figures 6 and 7).

Acromion thickness (At)

Acromion width (Aw)
Distal clavicle–acromion angle
The coronal plane was built on the edge of the plate. The distal clavicle–acromion angle was then measured from the central axis of the distal clavicle and the acromion (Figures 8 and 9).

Distal clavicle–acromion angle in the three-dimensional polygonal model (γ)

Distal clavicle–acromion angle in pattern diagrams (γ)
Statistical analysis
SPSS 19.0 statistical software (IBM Corp., Armonk, NY, USA) was used to perform all statistical analyses. The above-mentioned morphological parameters were compared between patients with and without subacromial erosion using the t test. Sex was compared using the Mann–Whitney U test. A P value of <0.05 was considered to indicate statistical significance.
Results
Among 17 men and 19 women (mean age, 48.7 years; range, 21–76 years), 10 patients had type III and 6 patients had type IV acromioclavicular dislocation. All distal fractures (20 patients) were Neer type II injuries.
The distal clavicle–acromion angle in the subacromial erosion group (mean, 51.37° ± 5.59°) was significantly greater than that in the normal group (mean, 44.20° ± 3.83°; P < 0.05). The distal clavicle–coronal angle was significantly larger in the normal group (25.44° ± 2.51°) than in the subacromial erosion group (21.67° ± 4.06°; P = 0.026). However, no statistically significant differences in the acromion sagittal angle were present between the two groups (P = 0.37) (Table 1).
Various measurements in patients with and without bone erosion

Results are shown as mean ± standard deviation.
α: distal clavicle–coronal angle; β: acromion sagittal angle; γ: distal clavicle–acromion angle; Aw: acromion width; At: acromion thickness
P < 0.05 was considered statistically significant.
The thickness of the acromion was significantly different between men (9.72 ± 1.13 mm) and women (8.16 ± 1.89 mm; P = 0.02) (Table 2).
Various measurements according to sex

Results are shown as mean ± standard deviation.
α: distal clavicle–coronal angle; β: acromion sagittal angle; γ: distal clavicle–acromion angle; Aw: acromion width; At: acromion thickness
P < 0.05 was considered statistically significant.
The patients’ sex, age, and acromion thickness and width are compared between the two groups (with vs. without erosion) in Table 3.
Demographics and acromion width and thickness between patients with and without bone erosion

Results are shown as n (%) or mean ± standard deviation.
Aw: acromion width; At: acromion thickness
P < 0.05 was considered statistically significant.
Discussion
The clavicle is the only bone that supports the connection between the shoulder and the trunk; thus, it plays an important role in the stability of the pectoral girdle. Once the clavicle is fractured, surgeons are more inclined to repair it surgically to satisfy the need for early functional exercise and avoid malunion. 6 The shapes of the clavicle and acromion are irregular and complex. The hook plate currently used for this repair still does not perfectly match the anatomy of the distal clavicle and acromion 7 ; therefore, we performed the present study to determine whether a direct relationship exists between the acromioclavicular joint morphology and complications after internal fixation using a hook plate.
Currently, the main measurement parameter of the clavicle and acromion is their length, whereas the acromioclavicular angle is rarely measured. 8 Because the clavicle and acromion are irregular bones, the use of 3D analysis could allow for more accurate measurement of the required anatomical data than traditional measurement methods, thus providing a new way to investigate the causes of complications after fixation of the hook plate. In the past, the anatomical parameters of the clavicle were mainly measured on cadaver specimens, a practice that has the shortcomings of an inconvenient operation and inaccurate measurements.9,10 In the present study, 3D reconstruction software was used to reconstruct the clavicle using digital visualization to measure the related anatomical parameters. In 2010, Daruwalla et al. 11 used the 3D reconstruction technique for the first time for anatomical measurements of the clavicle, but the method has some disadvantages. The coordinate system he chose was based on the two ends of the clavicle, which may result in different measurement results. At present, the anatomical data for the clavicle are mostly obtained by measuring its length, width, thickness, and angle of flexion in the horizontal plane. Because the inclination of the distal clavicle in the sagittal plane was significantly greater than that of the middle of the clavicle according to the shape of the hook plate used with the current characteristics, the hook plate could not be simultaneously attached to the distal and proximal ends of the clavicle, forcing it to be attached to the hook tip and thereby resulting in excessive stress on the bone. This situation may promote the development of complications, such as subacromial erosion. 12
The incidence of osteolysis in the subacromial region may reportedly be as high as 25%. 13 The shape and position of the hook plate greatly influence the incidence of osteolysis. The depths of the currently used hook plates are 15 or 18 mm. We generally select the former. Intraoperatively, we often find that there is a greater distance between the proximal portion of the plate and the collarbone because of the anatomical structure of the clavicle itself. If the plate is forcefully attached to the bone surface, stress concentration occurs between the hook steel and hook tip, thereby leading to acromion bone dissolution.
In this study, we directly measured the anatomical angles of the acromion and observed the impact of the movement of the hook plate on subacromial erosion. This technique may be more intuitive for studying the impact of the anatomical angles on the degree of osteolysis. In addition to extending from high to low in the sagittal plane, the distal clavicle is low near the inner aspect and high near the outer aspect in the coronal plane. The presence of the acromion in both the sagittal and coronal planes may have an impact on osteolysis. Each patient’s CT angle is different, so the horizontal line cannot be used as the reference standard for the acromion’s coronary position. Based on the results of this study, an increased acromioclavicular angle promotes the occurrence of osteolysis. Therefore, when implanting a hook plate, we should use an appropriately precurved hook tip to increase the contact area between the tip of the hook and lower surface of the acromion; this will help to reduce the incidence of complications such as osteolysis and perforation of the acromion. In addition, as the distal clavicle–acromion angle increases, the risk of hook tip slippage may increase. According to the acromion width measured in this experiment, the length of the tip of the hook plate can be designed to meet the patient’s needs. A steel plate with a longer tip can reduce the risk of sliding out. In contrast, if the hook tip is too long to pierce the outside of the acromion, then the rotator cuff, joint capsule, or other soft tissue may be damaged. Hence, fluoroscopy is necessary during the operation.
With respect to the thickness of the acromion in this study (9.72 ± 1.13 mm for men, 8.16 ± 1.89 mm for women), the depths of the currently used clavicular hook plates (15 or 18 mm) are greater than the thickness of the measured acromion.2,14 If the hook depth is too great, the clavicle cannot be pressed into the appropriate position, resulting in an acromioclavicular joint that cannot be completely reset. This could affect the repair of peripheral ligaments. If we repair the coracoclavicular ligament and reset the acromioclavicular joint, the hook end would be farther away from the lower surface of the acromion, suspended in the gap underneath the acromion and resulting in internal fixation failure.
Because the distal clavicle (about 2 cm) is situated from high to low in the sagittal plane, the hook plate does not fit very well when placed on this section. Thus, if the rear portion of the hook plate is close to the clavicle, the front tip of the hook will become elevated, increasing pressure on the lower surface of the acromion and promoting osteolysis. Therefore, the variability of the clavicle’s anatomical structure promotes the occurrence of subacromial erosion.
Conclusions
We found that the distal clavicle–acromion angle and distal clavicle–coronal angle cause the hook plate to fit the clavicle and acromion with difficultly during the fixation. This imperfect fit may cause complications, such as subacromial erosion.
Footnotes
Acknowledgement
The present study was supported by the Hospital Funds of the First People’s Hospital of Wujiang (grant no. 201611).
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.