
Abstract
Objective
To identify risk factors associated with postoperative shoulder joint dysfunction in patients who underwent surgical intervention for acromioclavicular (AC) joint dislocation, with the aim of enhancing preoperative counselling, surgical planning, and postoperative management to optimize functional outcomes.
Methods
Patients who underwent surgery for AC joint dislocation between January 2018 and January 2023 at a hospital orthopaedic centre were enrolled into this retrospective study. Inclusion criteria were patients aged ≥18 years with a documented AC joint dislocation who underwent surgical treatment and had a minimum follow-up period >1 year. Patients with pre-existing shoulder conditions, prior shoulder surgeries, or incomplete medical records were excluded. Visual Analog Scale pain score ≥5 and Constant-Murley Score ≤70 was considered indicative of shoulder joint dysfunction. Statistical analyses included univariate and multivariate logistic regression to identify independent risk factors for postoperative shoulder joint dysfunction.
Results
Among 208 included patients, 56 (27%) exhibited shoulder joint dysfunction at the final follow-up. High-energy injury mechanisms, combined coracoclavicular ligament injuries, and lack of coronal plane congruity were identified as significant predictors of postoperative dysfunction. Specifically, high-energy injuries (odds ratio [OR] 5.493, 95% confidence interval [CI] 2.068, 14.590), combined coracoclavicular ligament injuries (OR 0.118, 95% CI 0.032, 0.432), and lack of coronal plane congruity (OR 2.540, 95% CI 1.197, 5.387) were associated with an increased risk of poor shoulder function postoperatively. Other factors, such as age, injury mechanism, and postoperative exercise compliance also contributed to the outcomes. Level of evidence: iv.
Conclusions
Injury mechanism, ligamentous injuries, and joint congruity are important in determining postoperative shoulder function. Accurate joint reduction and diligent postoperative rehabilitation are crucial for optimal recovery. These findings provide valuable insights for improving patient care and surgical outcomes in AC joint dislocation treatment. Further research is needed to validate these findings and explore additional factors that may influence postoperative shoulder function.
Keywords
Introduction
Acromioclavicular (AC) dislocation, characterized by the separation of the acromion and clavicle, is frequently encountered in orthopaedic practice.1,2 This condition can result from various mechanisms, including sports injuries, falls, and direct trauma to the shoulder. In a Danish study, the incidence rate of AC dislocations was observed to be 19.3 cases for every 100 000 person-years at risk. 3 Surgical intervention is often indicated for severe cases or recurrent dislocations, where conservative management has failed or is deemed inappropriate due to the patient's age, activity level, or specific occupational requirements.4–6
Despite advances in surgical techniques and a better understanding of shoulder biomechanics, postoperative complications, such as shoulder joint dysfunction, can impede the patient's functional recovery.7–9 Shoulder joint dysfunction refers to a range of issues that may arise after surgery, including pain, weakness, stiffness, and a decrease in the range of motion. These complications can significantly affect the patient's quality of life and ability to return to their pre-injury activities.10–12 Therefore, understanding risk factors that contribute to postoperative dysfunction is crucial for optimizing treatment outcomes and patient care.
Recent studies have highlighted the ongoing challenges in achieving optimal functional recovery following AC joint dislocation surgery. For instance, research has indicated that, despite technical advancements, a significant percentage of patients continue to experience functional limitations post-surgery. 13 Similarly, another study emphasized the variability in postoperative outcomes and the need for standardized rehabilitation protocols. 14
The current literature lacks a detailed investigation into the long-term functional outcomes and specific risk factors contributing to postoperative shoulder dysfunction. Most studies have been limited to short-term follow-ups or have not adequately stratified patients based on injury severity, surgical technique, or rehabilitation adherence.15–17 The aim of the present study was to address this gap by providing a comprehensive, multifactorial analysis of postoperative outcomes in a well-defined patient cohort, with a follow-up period extending to 18 months.
By identifying the key predictors of postoperative dysfunction, the study aims to contribute to the development of more effective treatment strategies for patients with AC joint dislocations. The findings are expected to enhance the understanding of how injury mechanism, ligamentous injuries, and joint congruity affect long-term outcomes, ultimately leading to improved patient care and functional recovery.
Patients and methods
Study design and patient population
Patients who underwent surgical intervention for AC joint dislocation and subsequent follow-up assessments at a single centre between January 2018 and January 2023 were sequentially enrolled into this retrospective study. Inclusion criteria were as follows: patients aged ≥18 years who had a documented AC joint dislocation and underwent surgical treatment; patients with a minimum follow-up period >1 year; and patients who underwent postoperative computed tomography (CT) scans to assess the integrity and congruity of the AC joint. Patients who met one or more of the following criteria were excluded: pre-existing shoulder conditions, prior shoulder surgeries, or incomplete medical records. The study was conducted in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki), and was approved by the Ethics Committee of Tongji Hospital, Tongji University. Written informed consent was obtained from all of the included patients. The patient data were collected from the database of Tongji Hospital Orthopaedic Centre and all patient information was de-identified. The reporting of this study conforms to STROBE guidelines. 18
Surgical procedure
Patients were administered surgical treatment within 48 h of hospital admission. Following successful anaesthesia, aseptic techniques were rigorously adhered to, including routine draping and disinfection. The surgical management of AC joint dislocations was standardized and involved either open reduction and internal fixation (ORIF) with hook plates or suture anchors, depending on the Rockwood classification of the dislocation and the presence of associated injuries. 19 The choice between ORIF using hook plates or suture anchors was determined by the operating surgeon (XFZ, ZYW, HFL or JF) based on the severity of the AC joint dislocation, patient-specific factors, and concomitant injuries. Hook plates were generally removed 6–8 months postoperatively. In cases with significant ligamentous injury, refixation of the coracoclavicular ligaments was performed using suture anchors to ensure joint stability. Haemostasis was meticulously achieved to ensure the reliability of internal fixation. Passive mobilization was performed to confirm satisfactory joint stability. The surgical field was irrigated with physiological saline, and the incision was closed layer by layer. The operation was conducted by a single, consistent surgical team (XFZ, ZYW, HFL and JF) to standardize procedural techniques.
Within 24 h postoperatively, prophylactic antibiotic therapy was routinely administered to prevent infection, comprising 2.0 g cefuroxime, intravenously, twice daily for 24 h. Additionally, to improve microcirculation and reduce postoperative oedema, 20 mg escin sodium was administered intravenously, once daily, and 40 mg parecoxib was administered intravenously, twice daily, for analgesia, with the duration determined by the patient’s pain level and clinical recovery course. On postoperative days 1–2, patients began with finger flexion and extension exercises, as well as fist clenching to promote circulation and prevent stiffness. From postoperative days 3–4, active and passive range of motion exercises for the shoulder joint, including flexion, extension, and internal and external rotation, were initiated to enhance joint mobility and muscle strength.
Sutures were removed on postoperative day 14. A graduated weight-bearing program for the shoulder joint was then commenced from postoperative week 4–6, with progression to activities of daily living by postoperative week 12. This systematic approach to postoperative care is designed to optimize functional recovery while minimizing the risk of complications following AC joint dislocation surgery. Patients operated on in 2018 were followed up for a minimum of 18 months postoperatively. This extended follow-up period allowed the capture of a broader range of outcomes and complications, providing a more comprehensive assessment of the surgical interventions.
Assessment of shoulder function
Shoulder joint function at 1 year postoperatively was assessed by a Visual Analog Scale (VAS) for pain and Constant-Murley Score (CMS). 20 The VAS, a commonly used simple and reliable method for assessing a patient's pain intensity, comprises a straight line, typically 10 cm in length, where one end represents ‘no pain’ (scored as 0) and the other end represents ‘worst imaginable pain’ (scored as 10). Patients mark a point on the line corresponding to their current level of pain, with lower scores indicating less pain and higher scores indicating more severe pain. The CMS is a comprehensive assessment tool used to evaluate shoulder function that consists of four parts: self-reported evaluation of pain (15%), activities of daily living (20%), range of shoulder joint motion (40%), and muscle strength (25%). The total score ranges from 0 to 100, with higher scores indicating better shoulder function and lower levels of pain or disability. A score closer to 100 reflects minimal impairment and near-normal shoulder function, whereas a lower score signifies greater impairment and dysfunction. A VAS score ≥5 and CMS ≤70 was considered indicative of shoulder joint dysfunction.
Data collection and definitions
Data on demographic characteristics, injury mechanisms, Rockwood classification, and postoperative outcomes were collected from the hospital database. Injury mechanisms were categorized as low- or high-energy, based on the nature of the trauma. Low-energy injuries were defined as those occurring from incidents such as falls during walking, which are commonly associated with less severe trauma. In contrast, high-energy injuries, indicative of more severe trauma, included events such as motor vehicle accidents and falls from a significant height, which often result in greater tissue damage and complexity in treatment.21,22 The presence of combined coracoclavicular ligament injury and rotator cuff injury, as well as the AC joint coronal and sagittal plane congruity, were assessed using preoperative and postoperative imaging.
Age and body mass index (BMI) were stratified to allow for a nuanced statistical analysis that accounted for their influence on the risk of postoperative shoulder joint dysfunction following AC joint dislocation surgery, according to the following criteria.
Age criterion: patients were categorized into age groups according to the World Health Organization definition of older adults as individuals who are ≥60 years of age. 23 BMI criterion: patients were classified based on their BMI, where a BMI >24 was considered to be overweight, according to the reference standards for BMI in China. 24
Hypertension was defined as having been diagnosed by a cardiologist prior to study inclusion or, in the absence of a prior diagnosis, having two consecutive blood pressure measurements exceeding 140/90 mmHg upon hospital admission. 25
Diabetes mellitus was defined as having been definitively diagnosed by an endocrinologist prior to study inclusion. The diagnosis of diabetes was based on established diagnostic criteria, which includes fasting plasma glucose levels, oral glucose tolerance test results, or glycated haemoglobin (HbA1c) levels, as per the International Diabetes Federation and the American Diabetes Association standards. 26
The coronal plane congruity of the AC joint was assessed using CT scans. Specifically, the condition was defined by the presence of a lateral clavicular displacement ≥3 mm relative to the acromion, in addition to an increased AC joint space width ≥2 mm.
Similarly, the sagittal plane congruity was evaluated through CT imaging, and was characterized by a lateral clavicular displacement ≥3 mm in relation to the acromion and an AC joint space width measuring ≥2 mm when viewed in the sagittal plane. 27
During the rehabilitation period, patients who engaged in functional exercises for less than 30 min daily were classified as having a lack of functional exercise. 28
Statistical analyses
Statistical analyses were conducted using IBM SPSS software, version 27.0 (IBM Corp., Armonk, NY, USA). Patient demographics and injury characteristics are presented using descriptive statistics, with patients dichotomized according dysfunctional or normal shoulder joint function at 1 year following AC joint dislocation surgery for univariate analysis, performed to identify factors associated with poor shoulder joint function. Categorical variables were compared using χ2-test or Fisher's exact test. A P-value <0.05 was considered statistically significant. Variables with a P-value <0.2 in the univariate analysis were included in a multivariate logistic regression model to identify independent risk factors for postoperative shoulder joint dysfunction. The odds ratios (ORs) and their 95% confidence intervals (CIs) were calculated, and a P-value <0.05 was considered statistically significant for the multivariate analysis. A power analysis was conducted prior to the study to determine the necessary sample size for detecting significant differences in postoperative outcomes. The analysis indicated that a sample size of at least 100 patients would provide adequate power (80%) to detect clinically relevant differences with a significance level of 0.05.
Results
The study included a total of 208 patients (mean age, 61.54 ± 6.81 years) who underwent surgical intervention for AC joint dislocation and met the study inclusion criteria (Figure 1). The duration of postoperative follow-up for the study population ranged from 12 to 18 months (mean duration, 17.05 ± 1.72 months), and at the final follow-up, 56 patients (27%) exhibited shoulder joint dysfunction based on VAS scores and CMSs (≥5 and ≤70, respectively). Univariate analysis was performed to identify factors associated with poor shoulder joint function at 1 year following surgery (summarized in Table 1).

Flow chart showing the enrolment, inclusion and exclusion of patients who underwent surgical intervention for acromioclavicular joint dislocation.
Univariate analysis of characteristics between patients with dysfunctional or normal shoulder joint function at 1 year following acromioclavicular joint dislocation surgery.

Data presented as n (%) prevalence.
Statistically significant difference at P < 0.05 (χ2-test or Fisher's exact test).
Sex and injury mechanism
Biological sex was not found to be a significant predictor of postoperative shoulder joint dysfunction. However, the injury mechanism was a significant factor, with high-energy injuries demonstrating a statistically significantly higher risk of dysfunction compared with low-energy injuries (P < 0.001).
Combined coracoclavicular ligament injury and Rockwood classification
The presence of a combined coracoclavicular ligament injury was not found to be significantly associated with postoperative shoulder joint dysfunction, but with P = 0.118, was included in the multivariate analysis. The Rockwood classification of the dislocation also displayed no statistically significant association, suggesting that the classification system may not be a robust predictor of functional outcomes in this context.
Age and BMI
Age was a statistically significant predictor of postoperative shoulder joint dysfunction, with patients aged ≥60 years having a higher risk of postoperative dysfunction (P < 0.001). BMI, however, did not show a significant association with the risk of dysfunction.
Affected side and combined rotator cuff injury
The side of the shoulder affected (right or left) was not significantly associated with postoperative dysfunction. Interestingly, the presence of a combined rotator cuff injury, although not statistically significant (P = 0.056), was included within the multivariate analyses, and may warrant further investigation.
AC joint congruity
Both the coronal (P < 0.001) and sagittal (P < 0.001) plane congruity of the AC joint were significantly associated with postoperative shoulder joint dysfunction, highlighting the importance of accurate joint reduction during surgery.
Lack of functional exercise
Patients who reported a lack of functional exercise postoperatively, defined as <30 min daily, were significantly more likely to experience poor shoulder joint function (P = 0.005).
Multivariate analysis
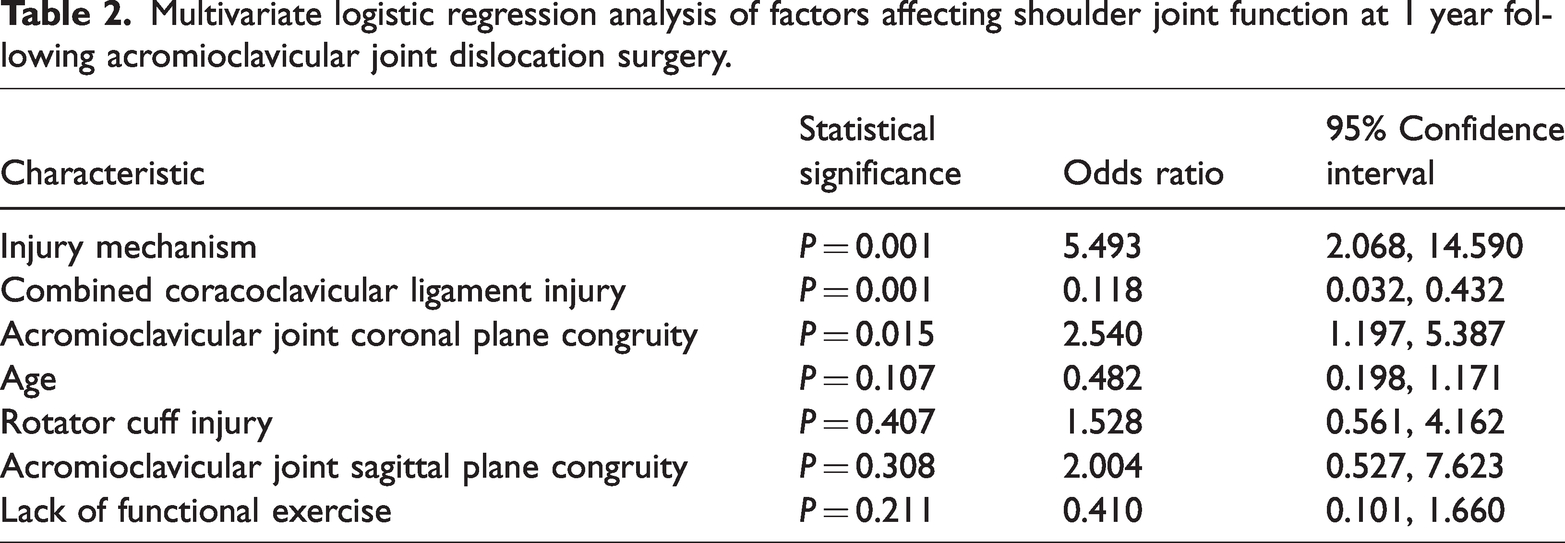
A total of seven factors were included in the multivariate logistic regression analyses: injury mechanism, presence or absence of combined coracoclavicular ligament injury, patient age, presence or absence of combined rotor cuff injury, presence or absence of either coronal plane congruity or sagittal plane congruity, and lack of functional exercise. Multivariate logistic regression identified three independent predictors of postoperative shoulder joint dysfunction (Table 2). High-energy injury mechanisms (OR 5.493 [95% CI 2.068, 14.590]; P = 0.001), combined coracoclavicular ligament injuries (OR 0.118 [95% CI 0.032, 0.432]; P = 0.001), and lack of coronal plane congruity of the AC joint (OR 2.540 [95% CI 1.197, 5.387]; P = 0.015) were significantly associated with an increased risk of dysfunction.
Multivariate logistic regression analysis of factors affecting shoulder joint function at 1 year following acromioclavicular joint dislocation surgery.
Discussion
The most significant finding of the present study was the identification of key risk factors associated with postoperative shoulder joint dysfunction following AC joint dislocation surgery. Specifically, the study found that high-energy injury mechanisms, combined coracoclavicular ligament injuries, and lack of coronal plane congruity are independent predictors of poor functional outcomes. These findings offer critical insights that may inform preoperative counselling, surgical planning, and postoperative management.
The CMS was used in the present analysis as a benchmark for defining shoulder joint dysfunction (≤70), and is an important threshold in evaluating patient outcomes. 29 The observed associations with specific risk factors underscore the complexity of AC joint injuries and the challenges they present in surgical repair and postoperative recovery. 30 The present findings suggest that targeted modifications to surgical techniques and rehabilitation protocols may be necessary to optimize outcomes for patients with high-energy injuries or combined ligament damage. This includes more meticulous surgical techniques to restore ligament integrity and tailored rehabilitation protocols that account for the severity of the injury.
High-energy injury mechanisms
The strong association found between high-energy trauma and poor postoperative shoulder function highlights the severe nature of these injuries, which often involve extensive damage to the stabilizing structures of the shoulder. This complicates surgical repair efforts and increases the risk of suboptimal restoration of joint stability and function. The present findings are consistent with existing literature, 31 reinforcing the need for tailored surgical approaches in managing high-energy AC joint dislocations. The significant association between high-energy injury mechanisms and poor postoperative shoulder function is also consistent with the Rockwood classification, which accounts for the severity of soft tissue damage in determining treatment approaches.
Combined coracoclavicular ligament injuries
The significant correlation observed in the present study between combined coracoclavicular ligament injuries and AC joint stability aligns with biomechanical research highlighting the essential role of the coracoclavicular ligaments in maintaining joint integrity.32–34 The present study suggests that injury to both the conoid and trapezoid ligaments increases the likelihood of postoperative complications, emphasizing the need for precise surgical techniques to restore ligament integrity.
Coronal plane congruity
The present findings highlight the importance of achieving and maintaining coronal plane congruity during AC joint surgery. Inadequate reduction and joint incongruity can lead to increased contact stresses, early osteoarthritis, and impaired shoulder function.35,36 The present study results reinforce the necessity of meticulous surgical realignment and the use of intraoperative imaging to ensure accurate joint reduction.
Interestingly, the present study did not find a significant relationship between the Rockwood classification and postoperative shoulder dysfunction. This observation suggests that while the Rockwood classification is valuable for guiding surgical decisions, it may not be a reliable predictor of functional outcomes.37,38 This finding warrants further research to explore the limitations of the classification system in prognostic stratification.
Clinical implications
The present study emphasizes the critical role of AC joint coronal plane congruity in preventing postoperative shoulder dysfunction. Surgeons must ensure precise alignment of the clavicle and acromion to maintain joint stability. The postoperative rehabilitation process should focus on exercises that promote AC joint stability while preserving coronal plane congruity. A balance between aggressive rehabilitation and the preservation of joint congruity is vital for successful outcomes. 39 Some authors have advocated for over-reduction to ensure stability and prevent recurrent dislocation. 2 However, achieving the correct balance between over-reduction and maintaining joint congruity remains a challenge and requires further investigation.
Limitations
The results of the present study may be limited by several factors, including the potential for selection bias due to the retrospective design, the heterogeneity of the patient population, and small sample sizes in certain subgroups. Further studies with larger cohorts and prospective designs are needed to validate the present findings.
Conclusion
This study underscores the importance of AC joint coronal plane congruity, high-energy injury mechanisms, and coracoclavicular ligament integrity in predicting functional outcomes after AC joint dislocation surgery. Future research should focus on refining assessment methods for AC joint coronal plane congruity and developing standardized protocols to enhance patient care and outcomes.
Footnotes
Author contributions
All authors listed meet the authorship criteria according to the latest guidelines of the International Committee of Medical Journal Editors. Xingfei Zhu and Jan Fan: study conceptualization; Zhiyuan Wang: methodology; Haifeng Li: investigation; Xingfei Zhu: writing the original draft. All authors are in agreement with the manuscript.
Data availability
All data generated or analysed during this study are included in this published article.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.