
Abstract
Sonography has made substantial technological improvements over the years, removing many of the barriers to its application in evaluation of the musculoskeletal (MSK) system. Sonography offers the advantages of a dynamic, real-time evaluation that routinely incorporates patient movement, evaluation of MSK structures in symptomatic positions with real-time feedback from patients, and a patient-friendly, noninvasive imaging modality. However, educational standards and efficacy of musculoskeletal ultrasonography (MSUS) have demonstrated as much variance as published reports of MSUS accuracy and interobserver agreement. This review focuses on the available literature on MSUS utilization and training and the need for development of international standards and protocols that will serve to improve clinical application and interpretation as well as the quality of research, improving reliability and reproducibility of data.
Introduction
Despite advancements in the technology and utility of musculoskeletal ultrasonography (MSUS), little progress has been made to reconcile the extreme variance in education and training for this modality. A growing number of countries have implemented musculoskeletal (MSK) programs into medical students’ curriculum and/or provided supplementary training. However, the guidelines are sparse and lack consistency in length of time, number of examinations performed, and knowledge required for proficient musculoskeletal sonographic performance. Increasing literature centering on observational and interpretational discord between operators and reading radiologists can perpetuate the skepticism MSUS has struggled against within imaging and rheumatology communities, detracting from its value and utility. Reports on the unreliability of data obtained through quantitative ultrasound measures continues to be published highlighting the limitations inherent to this field, such as operator dependence and experience as it relates to the diagnostic quality of MSUS. These factors, along with the increasing trend of sonographic implementation in musculoskeletal evaluation, indicate a pressing need for standardization of protocols and technique to legitimize this modality and improve the consistency of its application and interpretation.
Musculoskeletal Sonography
Since its introduction in the late 1950s, sonography has made substantial technological improvements, removing many of the barriers to its application in MSK evaluation. Increased transducer frequencies have enhanced resolution of soft tissue, cartilage, and bony surfaces, and software technology enables improved visualization of MSK anatomy and pathology through the use of elastography and contrast agents. The portability of many newer machines has made this modality invaluable to rheumatologists as a method to guide interventional procedures. These measures have improved the overall global utilization and acceptance of MSUS, evidenced by the increasing literature on its application. The limitations and challenges of this modality continue to contribute to the apprehension many radiologists and rheumatologists have regarding its current and future role in MSK evaluation.
Advantages of Sonography
Compared to magnetic resonance imaging (MRI) as a gold standard, MSUS possesses unique attributes that lend value to this imaging method. Sonography allows focal interrogation of pathology and allows dynamic, real-time evaluation that routinely incorporates patient movement. A more thorough evaluation can be conducted of MSK structures in symptomatic positions and enables real-time feedback from patients, enhancing diagnostic value. Sonography also can be considered the more patient-friendly imaging modality as it imposes no restrictions on space or movement, which is an important consideration for patients who suffer from claustrophobia. Sonography has gained significant stature as a complementary tool in rheumatologic applications for guidance assistance, enhancing physicians’ clinical skills. Sonography plays a major role in shoulder assessment, has demonstrated superiority in knee assessment over the clinical examination, improves the accuracy of injection procedures, and has aided in the provision of new insights into pathogenic processes of rheumatic diseases.1–5 In addition to the increased utility of this modality through technological improvements, sonography is a less expensive technique to employ, which is in line with the cost-effective initiatives of America’s Health Care Reform Act. The economics of medical imaging will almost certainly impact the potential influence this advantage may have in the future on third-party payers’ requirements in MSK assessment prior to authorizing MRI evaluations.
Limitations of Sonography
Sonography is the most operator-dependent medical imaging modality in use today, which remains a primary limitation of this technique in MSK evaluation. This limitation poses the greatest risk of observer bias; the risk of incorrect image acquisition and/or interpretation attributable to experience can adversely impact patient diagnosis and plan of care. 6
Technical limitations commonly encountered with sonographic evaluation of musculoskeletal structures include artifactual anisotropy as reliable MSUS assessment relies on the transmission of the sound beam perpendicular to the imaged structure. 4 Deviation from a 90° angle will partially reflect the sound beam away from the transducer, reducing the signal amplitude and corresponding echogenicity of the structure displayed. Although a commonly occurring limitation, anisotropy can be eliminated by maintaining an angle of insonation perpendicular to the tissue of interest. Reduced diagnostic capability of sonography in bone assessment can also be attributed to poor sound beam interaction with certain types of tissues. The physical properties of bone result in absorption of sound waves, inhibiting evaluation of intra-osseous and intra-articular structures in musculoskeletal evaluation. However, these technical limitations can be overcome through training dedicated to appropriate transducer selection, proper probe position and angling techniques, and the assurance of solid, uniform skin contact.
Challenges
The slow acceptance of sonography in musculoskeletal evaluation can be attributed largely to the apprehension of many radiologists and rheumatologists to take on a time-consuming modality with no standardized methods of training. The historical variances in educational standards, prolonged learning curve, and low rates of competency assessment have also contributed to the questionable reliability and reproducibility in published reports.5,7 Historically, and to a certain extent still today, a great deal of MSUS is performed directly by radiologists; therefore, formal educational programs are largely inaccessible or far too anatomically advanced for the majority of Sonographers and rheumatologists. Several programs utilizing guidelines for training recommended by organizations such as the European League Against Rheumatism (EULAR) have been challenged for being excessive, especially by physician groups in the United States. 8 In addition to skepticism about the diagnostic accuracy of MSUS, many rheumatologists lack the necessary technical knowledge to perform the examinations proficiently 9 and point to cost and availability of instrumentation as obstacles to integration of sonography in the clinical setting.
Variability of Results of MSUS
Reports of randomized clinical trials evaluating the diagnostic accuracy of a modality contain the implication that a universal protocol is utilized; however, the failed development and adoption of international standards renders the majority of MSUS research inconsistent with this assumption. Continued apprehension regarding MSUS utility may be attributed to published reports of diagnostic quality and reliability of sonography in musculoskeletal assessment. Interobserver and intraobserver variance and operator experience have been topics of interest in publications focusing on discrepancies in pathology interpretation between operators, MRI examinations, and radiologists. Because the high degree of operator dependence, skill level, and/or experience greatly influence the image acquisition and efficacy of technique employed, the nonstandardized protocols implemented in such reports are critical to the resulting variance between observers, operators, and interpreters. 10
In a study by Juni et al 11 conducted to evaluate the impact of protocol on MSUS test accuracy in detecting carpel tunnel pathology, failure to define clear-cut standards resulted in a substantial degree of variability in test performance characteristics, negatively impacting the perception of diagnostic accuracy. A study by Jousse-Joulin et al 12 investigating the reproducibility of clinical synovitis by sonographic assessment determined the inter- and intraobservational reliability to be highly dependent upon the examiner, indicating technique and protocol were major factors in reported results. Research supporting these data from a study by Gagnon et al 13 on MSUS application for tendon assessment found low interrater reliability and recommended an established protocol to minimize measurement error and improve reliability. A study by Stenboeg et al 14 implemented EULAR recommendations for the assessment of joints with MSUS and found protocol and scanning technique to have the greatest impact on observer variability; specifically, the position of the transducer and joints during image acquisition being critical to reproducibility and, therefore, reliability of data.
The impact of protocol remains an underlying question in contradictory reports. For example, two studies reporting inter- and intraobserver agreement of MSUS involving finger and toe joints utilizing nonstandard protocol found a high rate of reproducibility between operators ranging from 82% to 97% overall.15,16 A separate study on the interobserver reliability of rheumatologists who performed sonographic assessments in accordance with EULAR recommendations found overall agreement in toe joints at 82% and lower agreement for finger joints of 73%, demonstrating a moderate level of reliability despite consistent protocol application. 17 Similarly, reported results on the reliability of MSUS of the shoulder have ranged from 81% between expert MSUS operators using established protocols and following EULAR MSUS guidelines 17 to 98% agreement between two operators, one expert and one with no previous training in MSUS assessment, using nonspecific scanning techniques. 18 Additional studies also demonstrate variable results of accuracy and ill-defined parameters of what constitutes experience in a Sonographer. The study by Lee et al 19 examined the sensitivity and specificity of MSUS in knee assessment and found them to be 32% and 59%, respectively, when performed in general radiologic practices without established expertise in MSUS application; they failed to find added value in the complementary utilization of MSUS with clinical examinations for knee pathology. This can be compared to the study of Schmidt et al, which showed 88% and 91% sensitivity and specificity in sonographic knee evaluations performed by 14 expert MSK radiologists in compliance with EULAR recommendations. 17 While many of the published reports do not define the protocol utilized, it can be reasonably assumed that the variance in observation and interpretation is at least as great as the techniques and skill levels of the Sonographers performing the scans. The result is an increasing number of reports of low levels of agreement that threaten to undermine the value and reliability of MSUS and decrease its overall implementation and utility.
Experience as a Factor
Other studies center on experience as a determining factor in MSUS diagnostic accuracy, though the length of time performing MSUS, method of training, and numbers of cases are not clearly defined by most published trials. For example, a report by Vlychou et al 20 demonstrated an accuracy of 87% for MSUS of the shoulder compared to arthroscopy or open surgical findings; it was noted by the investigators that the Sonographer had been performing MSUS for two years and this experience likely contributed to the resulting high degree of accuracy. A study by Tanimura et al 21 on the interobserver agreement in MSUS detection of rheumatoid synovitis found higher levels of agreement between two experienced MSK Sonographers compared to the third inexperienced Sonographer in pathological detection. In contrast to this, a study exploring the potential impact of specialty background and experience on interobserver agreement in detecting rheumatoid arthritis in the fingers and toes with MSUS reported little impact of background and experience between an experienced MSK radiologist and a rheumatologist with experience consisting of only 50 supervised MSUS exams. 15 Reported studies have also found little difference in the learning curve and the agreement of multiple joint evaluations between less experienced Sonographers and seasoned MSK Sonographers.22–24 A high degree of agreement was achieved between an operator with ten months of experience and a rheumatologist with ten years of MSUS experience, as well as between Sonographers with one versus four years of experience.22,23 To compound the contrary reports further, some research has suggested that greater interobserver agreement, despite experience, is more easily achieved with MSUS of specific anatomical sites. 24
The overall variability illustrated in the published literature likely represents the variability of MSUS technique in practice. The implications surrounding conflicting reports suggest a significant impact of protocol and experience on the diagnostic capabilities of MSUS, which further suggests that the development of guidelines for training and standardization of protocol may be very difficult to devise and implement, but nonetheless important.
Training
While MSUS has made substantial progress in the imaging world it has not succeeded in developing formal training inclusive of criteria and protocols that are critical to the diagnostic capability of the examination and accuracy of the interpretation. Despite the low accessibility of educational programs for many Sonographers and rheumatologists, there are myriad formats of MSUS education currently in place containing a degree of variance rivaling the previously discussed publications. The increasing international attention and acceptance of MSUS has compelled some national and international organizations to develop curriculum and training standards to deliver MSK education to radiologists and rheumatologists. Available methods of MSUS training in place consist of a mixture of formal, informal, and self-guided training with globally divided parameters defining competence. An international survey of the current training experience of practicing MSUS radiologists and rheumatologists showed that 74% of those surveyed were self-taught, 63% took a formal training courses, 50% had been supervised by an expert, 34% had been trained by an MSUS specialist; also, 38% of those surveyed reported a competency assessment, though the majority consisted of peer review processes. 25
In the United States, the American College of Radiology (ACR) recommends a four-month training consisting of a minimum of 500 scans evaluating multiple anatomical sites.5,26–28 The American Institute of Ultrasound in Medicine (AIUM) also recommends 500 scans on multiple MSK sites or 300 scans dedicated to a single anatomical site. In Europe, EULAR recommendations for training are incorporated into rheumatology training in Germany and Italy consisting of 200 jointly performed examinations and 60 independently performed MSUS examinations. 5 The UK has no current guidelines, though the Royal College of Radiology recommends 300 hours of supervised scanning, and the Society of Academic Emergency currently employs educational requirements of 150 sonography examinations.5,26 The Spanish Society of Rheumatology recommends 90 examinations for intermediate certification and a total of 180 scans for advanced certification. 28 In addition to these formal programs, there are several organizations that offer self-directed web-based courses, such as EULAR and Michigan Health Systems, that include illustrations, technical information, and guidelines for MSUS. 5 The utility of available training programs was assessed in 2010 in a survey that consisted of an international analysis reflecting that 22.6% of countries had implemented MSUS training as a mandatory component in rheumatology education, 35.5% of countries offer this as an elective, and only 6% of the programs in place require a competency assessment. 7
The disproportionate number of facilities, nonstandard content, and lack of international training curriculum, competence assessment, certification, or national registry all contribute to the widespread variance of results in the use of MSUS by radiologists and rheumatologists. This continued absence of formal training standards defining the basic level of competence for MSUS operators has important educational implications. It raises questions regarding who should administer training, when it should be implemented, and in what form it should be delivered in order to legitimize MSUS. These issues have generated interest among researchers in defining the efficacy of MSUS program structure currently available to define which parameters influence the skills and experience of operators.
Formal training standards and recommendations have been reviewed and researched for their content, such as the adequacy of the number of examinations recommended. In 2001, a study by Bearcroft and Speed 26 to determine the minimum number of cases required to achieve clinical competence found that performance was not adequate at 200 scans when evaluating the performance of radiology residents. These data undermine the national standards of organizations that recommend 200 examinations (or less), such as the programs in Germany and Italy, 5 as well as the educational requirements of the Society of Academic Emergency Medicine and the Spanish Society of Rheumatology.26,28
The efficacy of informal training has been explored in relation to the length of the program to define how much time is sufficient to develop clinically acceptable scanning skills. A study performed in 2006 on applied informal training evaluated a program consisting of courses in basic ultrasound over a three-month period with 5 hours per week of supervised scanning and found the length and content sufficient for acceptable clinical skills 29 (Figure 1). Other studies found smaller timeframes adequate. A novice scanner who underwent an intensive four-week program developed skills reportedly comparable to the expert rheumatologist, based on moderate to excellent interobserver agreement in pathologic detection of bone erosions 30 (Figures 2, 3, 4). Research on a 16-hour introductory course for physicians found it provided adequate skills to obtain high degrees of accuracy. 26 Web-based courses have reported high rates of success at imparting the skills necessary to achieve clinical acceptance and agreement in MSUS. An evaluation of the efficacy of online learning by Unlu et al 31 included the performance of an operator following review of images on the EULAR website, 2 hours of tutoring from an experienced Sonographer, and 24 nonconsecutive hours of active scanning. The results reported a mean score within clinically acceptable parameters for diagnostic quality and accuracy. A 3-hour self-directed training based upon information and illustrations from a web-based program in MSUS of the hip was deemed sufficient in length and context to acquire the necessary MSK sonographic skills, 27 and a 75-minute mentored training of a Sonographer with one year experience in MSUS yielded 96% accuracy and overall clinical competence in guided injections. 32 In contrast, other studies report training has less influence on the interobserver agreement in many joints, but that sonographic accuracy of tissue pathology is greater with experience and/or training. 28
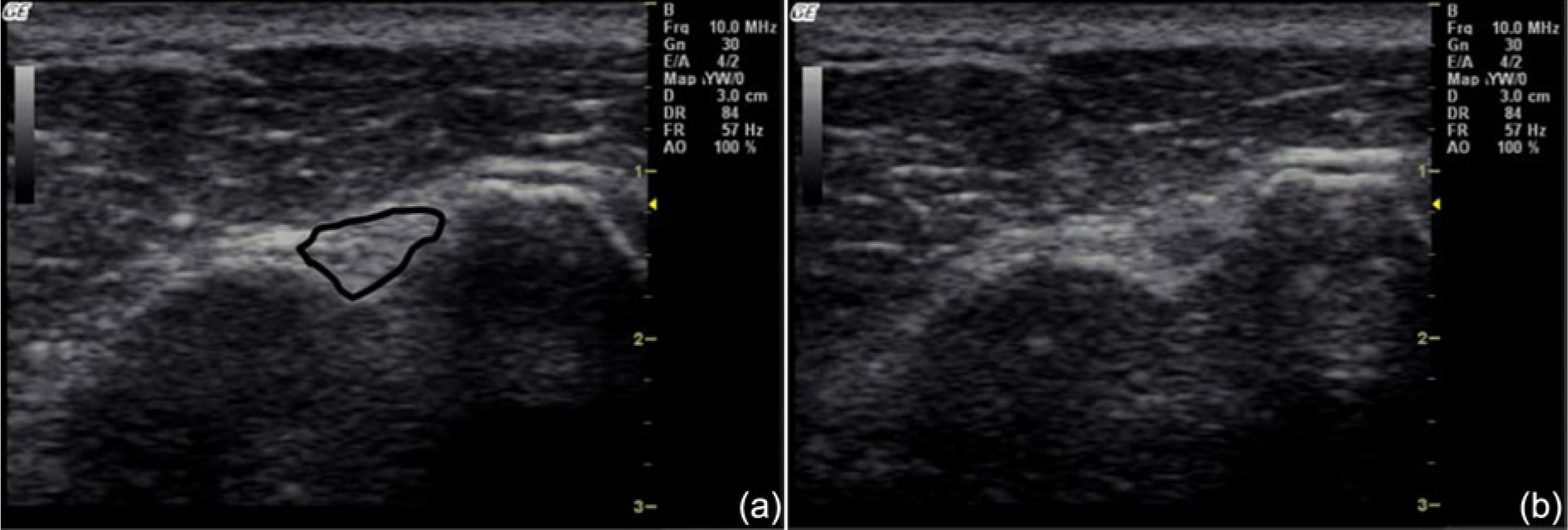
(a) Transverse view of the proximal long head of the biceps tendon (shown outlined) in the bicipital groove with the transducer face held perpendicular to the tendon. (b) Same image as a, but with the transducer held slightly oblique to the tendon (not at 90°), causing the tendon to appear hypoechoic (darker) because of tissue anisotropy; this can mimic a tear of the tendon. Reprinted with permission from Lento PH, Primack S. Advances and utility of diagnostic ultrasound in musculoskeletal medicine. Curr Rev Musculoskelet Med 2008;1(1):24–31.
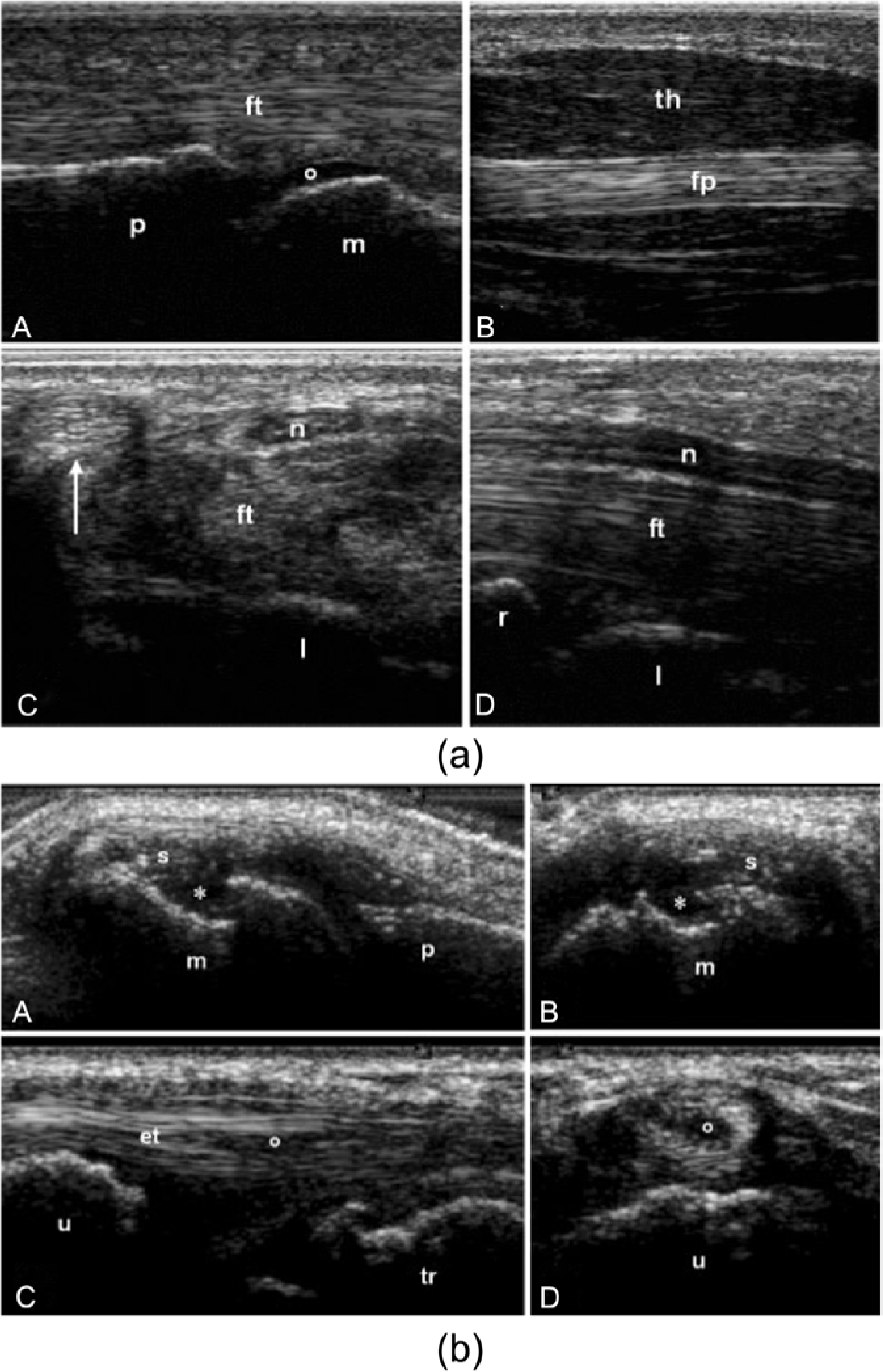
(a) Sonographic images of healthy subjects taken by rheumatologists during a competency assessment after three months of mentored training. (A) Longitudinal volar scan of a metacarpophalangeal joint. (B) Longitudinal scan of the thenar eminence. (C) Transverse and (D) longitudinal volar scans of the carpal tunnel. (b) Sonographic images of patients with rheumatoid arthritis taken by rheumatologists during a competency assessment after three months of mentored training. (A) Longitudinal and (B) transverse dorsal scans of the metacarpophalangeal joint showing synovial hypertrophy (s) and a bone erosion (*) of the metacarpal head (m). (C) Longitudinal and (D) transverse lateral scans of compartment six of the wrist showing a partial rupture (o) of the extensor carpi ulnaris tendon (et). Reprinted with permission from Taggart A, Filippucci E, Wright G, et al.: Musculoskeletal ultrasound training in rheumatology: the Belfast experience. Rheumatology (Oxford) 2006;45:102–105. Abbreviations: m, metacarpal head; p, proximal phalanx; o, articular cartilage; ft, finger flexor tendons; fp, flexor pollicis longus tendon; th, muscles of the thenar eminence; l, lunate bone; n, median nerve; arrow, flexor carpi radialis tendon; r, radius; u, ulna; tr, triquetrum.
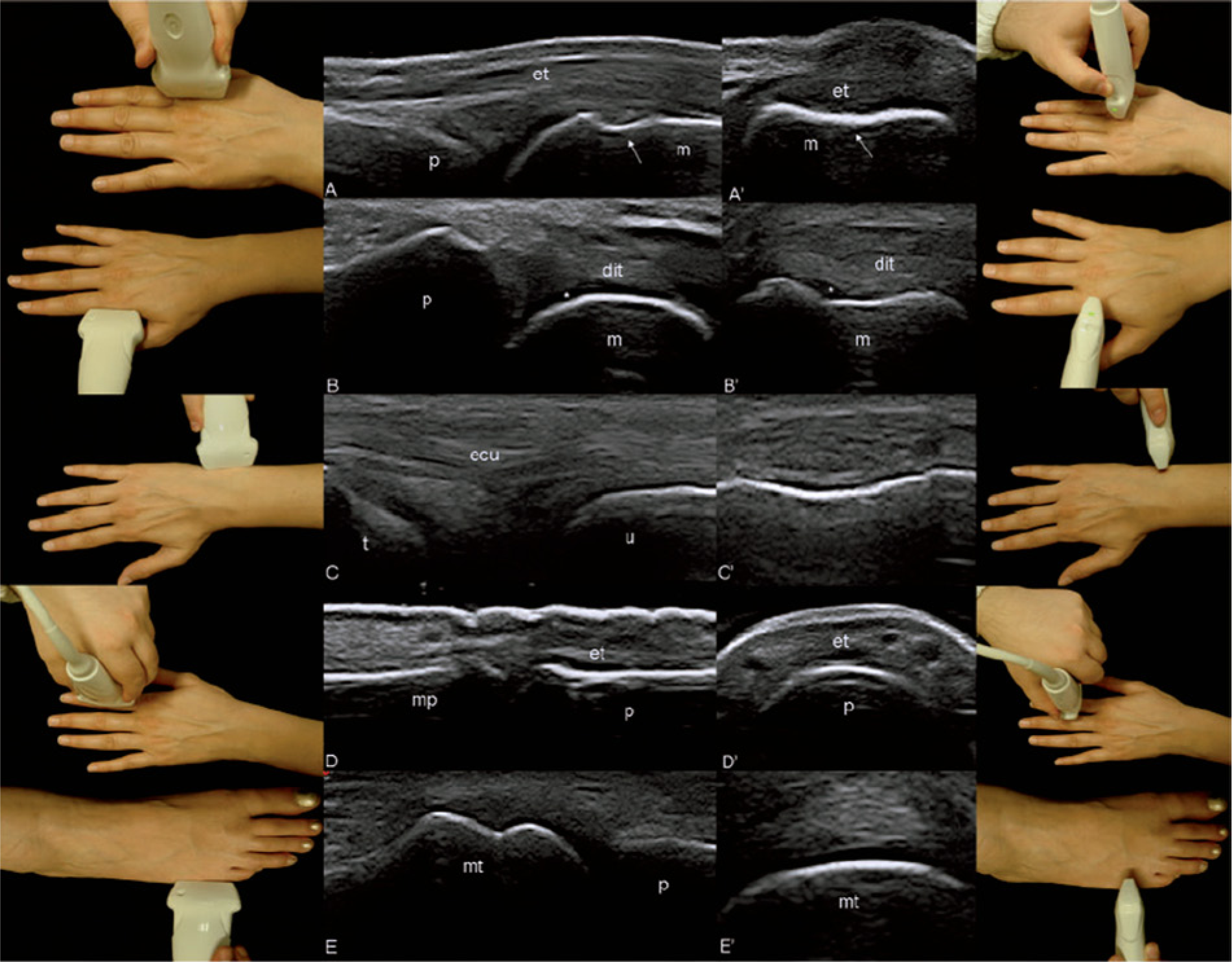
Sonographic images of a healthy subject taken by a rheumatologist without prior sonographic training after an intensive four-week mentored training program with the respective photographs showing where the transducer was placed for the examination. (A) Longitudinal and (A′) transverse dorsal scans of the second metacarpophalangeal joint showing the regularity of the bone profile at the anatomical neck level (arrows). The same joint on (B) longitudinal and (B′) transverse lateral scans showing the clearly defined anechoic band corresponding to hyaline articular cartilage (*). The ulnar head on (C) longitudinal and (C′) transverse scans. The second proximal interphalangeal joint on (D) longitudinal and (D′) transverse dorsal scans. The fifth metatarsal phalangeal joint on (E) longitudinal and (E′) transverse lateral scans. Reprinted with permission from Gutierrez M, Filippucci E, Ruta S, et al.: Inter-observer reliability of high-resolution ultrasonography in the assessment of bone erosions in patients with rheumatoid arthritis: experience of an intensive dedicated training programme. Rheumatology (Oxford) 2011;50:373–380. Abbreviations: p, proximal phalanx bone; m, metacarpal bone; u, ulnar bone; t, triquetrum bone; mp, middle phalanx; mt, metatarsal bone; et, extensor digitorium tendon; dit, first dorsal interosseous tendon; ecu, extensor carpi ulnaris tendon.
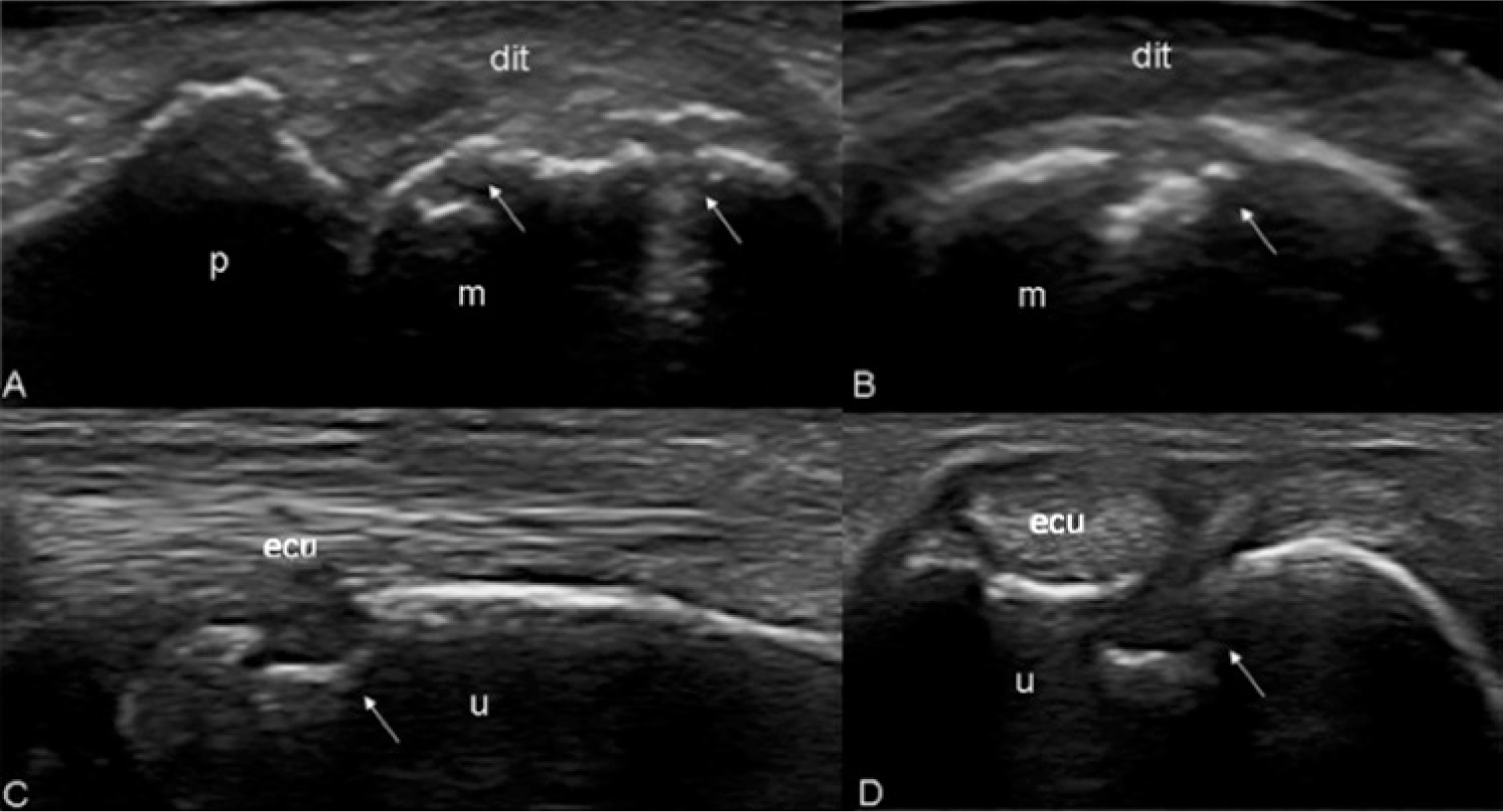
Sonographic images taken by the same rheumatologist as in Figure 3 showing gray scale features of bone erosions (arrows) of the second metacarpal head on (A) longitudinal and (B) transverse lateral scans and of the ulnar head on (C) longitudinal and (D) transverse lateral scans. Reprinted with permission from Gutierrez M, Filippucci E, Ruta S, et al.: Inter-observer reliability of high-resolution ultrasonography in the assessment of bone erosions in patients with rheumatoid arthritis: experience of an intensive dedicated training programme. Rheumatology (Oxford) 2011;50:373–380. Abbreviations: m, metacarpal bone; p, proximal phalanx; u, ulnar bone; dit, first dorsal interosseous tendon; ecu, extensor carpi ulnaris tendon.
The objective of studies undertaken to evaluate the parameters of education primarily seeks to define the minimal training required for the student to acquire the greatest degree of diagnostic accuracy. However, the variability of the reported efficacy of such programs, coupled with the variability of skills, techniques, and educational programs available, continue to stymie integration of MSUS into MSK evaluation leading professional organizations to continue to push toward international standards and uniform protocols to improve the consistency of education and application of MSUS.
Discussion and Recommendations
MSUS utilization is clearly on the rise and available educational opportunities have garnered increasing interest among radiologists, rheumatologists, and Sonographers. A recent study determining the interest in MSUS among rheumatology fellows found up to 50% have attended a lecture or course on MSUS. Forty-one percent of fellowship programs have incorporated MSUS into their training to varying degrees. Up to 81% of those surveyed believe that MSUS has a future as a standard clinical tool for the rheumatologist. 28 Increasing utilization and acceptance of MSUS by radiologists and rheumatologists, combined with recent development of national registries issuing certification in MSUS, has necessitated professional recommendations to improve uniformity.
Experts in MSUS as well as the majority of involved professional organizations such as the American Registry of Diagnostic Medical Sonographers, EULAR, and the British Society of Rheumatology agree on the need for educational criteria to include the provision and establishment of detailed anatomical knowledge of the MSK system, basic knowledge of ultrasound physics, and hands-on experience, though the number of cases and extent of involvement by the operator has not yet been uniformly accepted.5,9,26 A renewed effort should be made in the form of a joint venture of radiologists and rheumatologists to facilitate the development of educational standards and improve the consistency and value of MSUS.
Conclusion
Experience and expertise in the operator-dependent field of musculoskeletal ultrasonography determine the value of diagnostic information, and education has the greatest impact on technique and interpretation. Educational standards and efficacy have demonstrated as much variance as published reports of MSUS accuracy and interobserver agreement. Developing consistency in the components of MSUS training including the form of delivery, criteria, cases, length of training, and methods of competency assessment are critical to improving uniformity. The development of international standards and protocols will serve to improve clinical application and interpretation as well as the quality of research, improving reliability and reproducibility of data.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.