
Abstract
Objective:
Although there are several methods to assess vocal cord (VC) paralysis, direct flexible laryngoscopy (DFL) is used as a main diagnostic modality. In recent years, transcutaneous laryngeal ultrasonography (TLUS) has emerged as an alternative method to evaluate VCs. The objective of this study was to investigate the efficiency of TLUS in the evaluation of VCs, post-thyroidectomy.
Materials and Methods:
The study included 93 patients who had undergone thyroid surgery. All patients were examined using DFL, 1 to 3 days before surgery, to evaluate their VC functions. Patients were examined using DFL and TLUS on postoperative day 7. Patients’ age, sex, diagnosis, type of surgery, preoperative DFL findings, postoperative DFL, and TLUS findings were recorded.
Results:
Sensitivity, specificity, positive predictive value (PPV), and negative predictive values (NPVs) were 75% (6/8), 98.66% (74/75), 85.71% (6/7), and 97.36% (74/76), respectively. The diagnostic accuracy of TLUS was 97.96%. The area under the receiver operator characteristic (ROC) curve was 0.869, P value <.0001 (95% confidence inteval, 0.75–1.00), which indicated that TLUS was a good tool for identification of VC palsy in this cohort of post-thyroidectomy patients.
Conclusion:
This cohort study demonstrated that TLUS was a reliable diagnostic tool to evaluate VC functions in patients after thyroidectomy. It may be used as a safer alternative during the ongoing COVID-19 pandemic due to the lack of human-originated aerosols.
Thyroidectomy is one of the most common surgical procedures for the treatment of thyroid cancer and other thyroid diseases. Although it is nowadays a safe operation with very low morbidity and a mortality rate of almost 0%, recurrent laryngeal nerve (RLN) palsy is still the most feared postsurgical complication.1,2 Permanent RLN paralysis is observed in 0.3% to 3% of postsurgical patients and transient paralysis in 5% to 8% of patient cases. 3 Although there are several methods to assess vocal cord (VC) paralysis, direct flexible laryngoscopy (DFL) is used as the main diagnostic modality. 4 The major advantage of DFL is its ability to visualize the VCs, in almost all cases. 5 However, this is an invasive procedure that often requires patient referral to an otolaryngologist, which increases health care costs and administrative burden. 6 In recent years, transcutaneous laryngeal ultrasonography (TLUS) has emerged as an alternative method to evaluate VCs, especially in intensive care units and among pediatric patients. This is a noninvasive procedure that can be easily performed on an outpatient basis, as well as being cost-effective, time-efficient, less painful, and well tolerated. 7 In the literature, there are studies that demonstrate the success of TLUS for VC evaluation in a wide range, but the application method and standardization of ultrasonography (US) are varied.8 –10 In this prospective cohort study, the objective was to investigate the effectiveness of TLUS in the evaluation of the VCs, post-thyroidectomy.
Materials and Methods
Study Design
This prospective study included 93 patients who had undergone thyroid surgery for benign or malignant thyroid disease, at a single tertiary referral hospital, between January 2020 and February 2021. The study protocol was approved by the institutional review board (approval number: 2022/514/221). The study was conducted in accordance with the Helsinki Declaration. The patients’ age, gender, diagnosis, type of surgery, preoperative DFL findings, and postoperative DFL and TLUS findings were recorded.
All patients were examined using DFL 1 to 3 days before surgery to evaluate their VC functions. The surgeries were performed under general anesthesia with standard tracheal intubation. Total thyroidectomy and lobectomy without central/lateral neck dissection was the surgical procedure. Patients were examined using DFL and TLUS on postoperative day 7. All laryngoscopic and sonographic examinations were performed by the same otolaryngologist and radiologist, and they were shielded from the results. The cases evaluated for vocal cord paralysis (VCP) were provided weekly US surveillance.
Inclusion and Exclusion Criteria
Patients aged more than 18 years, who underwent thyroid surgery at the Department of General Surgery, consented to the study. Patients with a history of thyroid, parathyroid, or neck surgery, preoperative VC palsy, and patients whose postoperative follow-up could not be performed at the host hospital were excluded from the study.
Ultrasonographic Imaging and Evaluation
Ultrasonography was performed on the VC of all cases on the seventh postoperative day, by a radiologist experienced in sonography. A 3- to 13-MHz linear-array transducer was used with a MyLab Seven ultrasound equipment system (Esaote, Genova, Italy). During the procedure, the patients were placed supine with their neck slightly extended. The ultrasound transducer was placed over the midsection of the thyroid cartilage and scanned cranio-caudally until both true and false cords were visualized. Passive (spontaneous breathing) and active (phonation with “aa”) movements of the VCs were evaluated. Asymmetric VC movements during abduction and adduction were evaluated as paralysis (see Figure 1). All of the US procedures were performed without the physician’s knowledge of the videolaryngoscopy (VDL) results for the VC investigated.
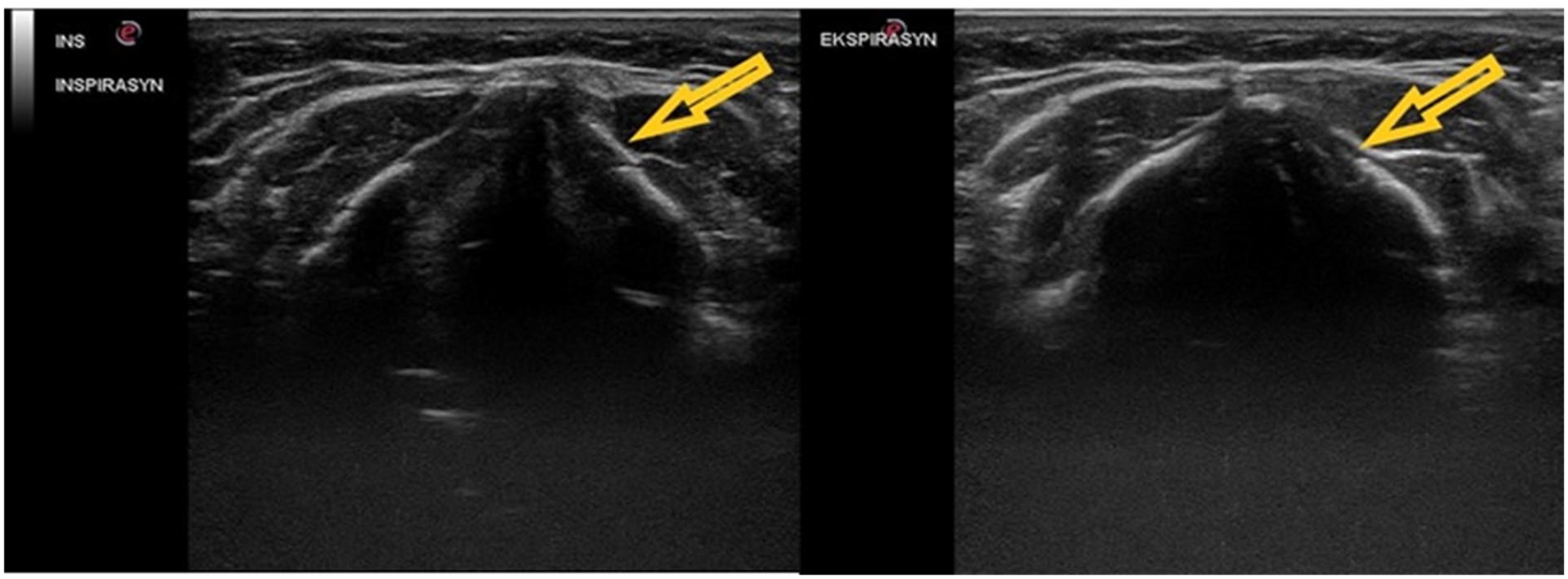
The vocal folds are demonstrated sonographically in the transverse plane, and the left vocal fold movements (indicated by the yellow arrow) are restricted during abduction and adduction.
Statistical Analysis
The statistical analysis of the data was performed using SPSS Version 18.0 software (IBM, Chicago, IL, USA). Descriptive statistical methods (median, mean, frequency, standard deviation, and minimum and maximum) were used to express central tendency. The Kolmogorov-Smirnov test was used to evaluate the normality of quantitative data distribution. The statistical difference between categorical data was evaluated using a Pearson’s χ2 test and Fisher exact test. A receiver operator characteristic (ROC) curve analysis was used to find the sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) for comparison of TLUS and VDL. All analyses were performed at 95% confidence level, and P < .05 was considered statistically significant.
Results
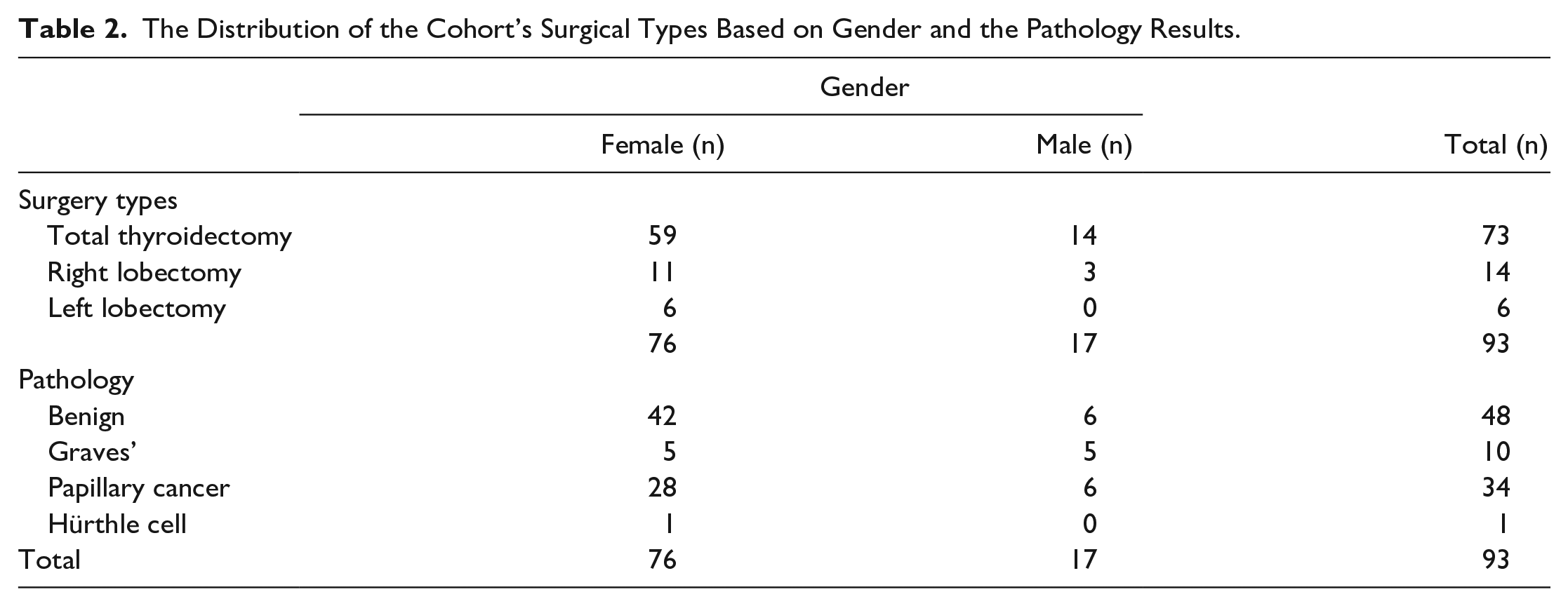
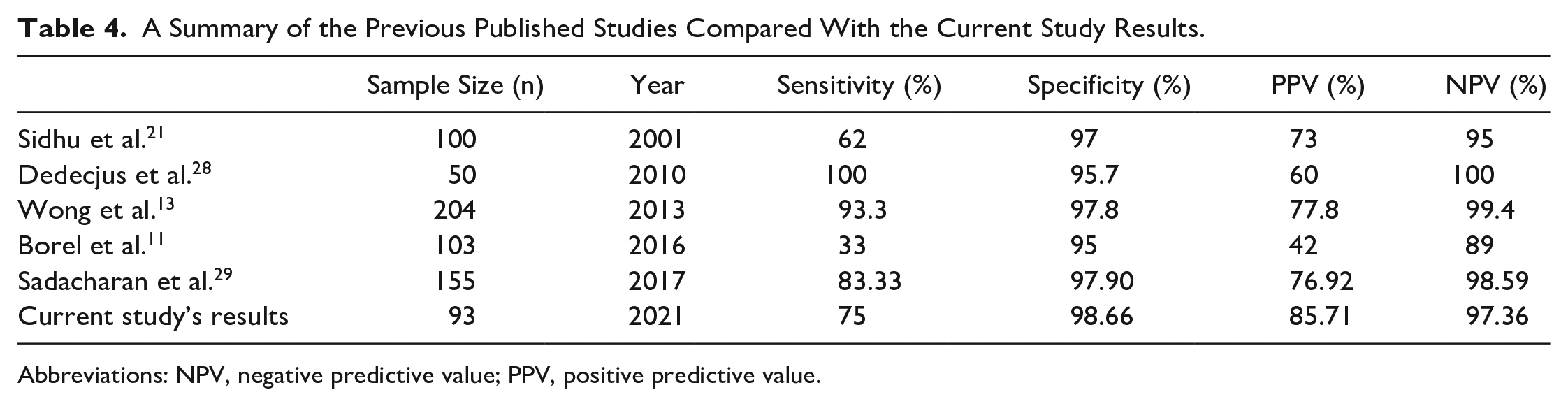
A total of 93 patient cases were included in this study. Descriptively, there were 76 women (18.3%) and 17 men (81.7%). The youngest patient was aged 31 years and the oldest was aged 80 years, both of whom were women. Among the male patients, the youngest case was aged 38 years and the oldest was aged 66 years (see Table 1). A total thyroidectomy was performed on 73 patients, a right lobectomy in 14 patient cases, and left lobectomy in six cases. Among the female patients, a total thyroidectomy was performed on 59 patients, a right lobectomy in 11 patient cases, and left lobectomy in 6 cases. In the male group, a total thyroidectomy was present in 14 cases at most, and there was no left lobectomy (see Table 2). When the pathology results were evaluated, the most common diagnostic findings were benign diseases, in 48 patients, and the second most common finding was papillary carcinoma, in 34 patients. At least one case had Hürthle cell neoplasia, and there were no male cases (see Table 2). According to the χ2 test of independence, there was a significant relationship between pathology results and gender (P = .045). Similar testing demonstrated no significant relationship between surgery types and gender (P = .47). Sensitivity, specificity, PPV, and negative predictive (NPV) value were 75% (6/8), 98.82% (84/85), 85.71% (6/7), and 97.67% (84/86), respectively (see Table 3). The diagnostic accuracy of TLUS was 96.9%. The area under the ROC curve was 0.869, P value <.0001 (95% confidence interval [CI], 0.75–1.00), which indicate that TLUS was a good diagnostic tool for identification of VCP in these post-thyroidectomy patients (see Figure 2). In Table 4, this study’s results and those of previous studies are summarized. When DFL was taken as a reference, the US did not detect VCP in two cases, and in only one male case, a normal VC was misdiagnosed as paralyzed. Transient hoarseness developed in one male and seven female cases and completely resolved at the end of the sixth week, without any medication. No statistical significance was found when the relationship between gender and hoarseness was evaluated using a Fisher exact test (P = 0.55).
The Study Cohort’s Descriptive Results Based on Those Who Consented to Participate.

The Distribution of the Cohort’s Surgical Types Based on Gender and the Pathology Results.
The Results of Detecting VC Paralysis Based on the Use of Ultrasonography.

Abbreviation: VC, vocal cord.
A Summary of the Previous Published Studies Compared With the Current Study Results.
Abbreviations: NPV, negative predictive value; PPV, positive predictive value.
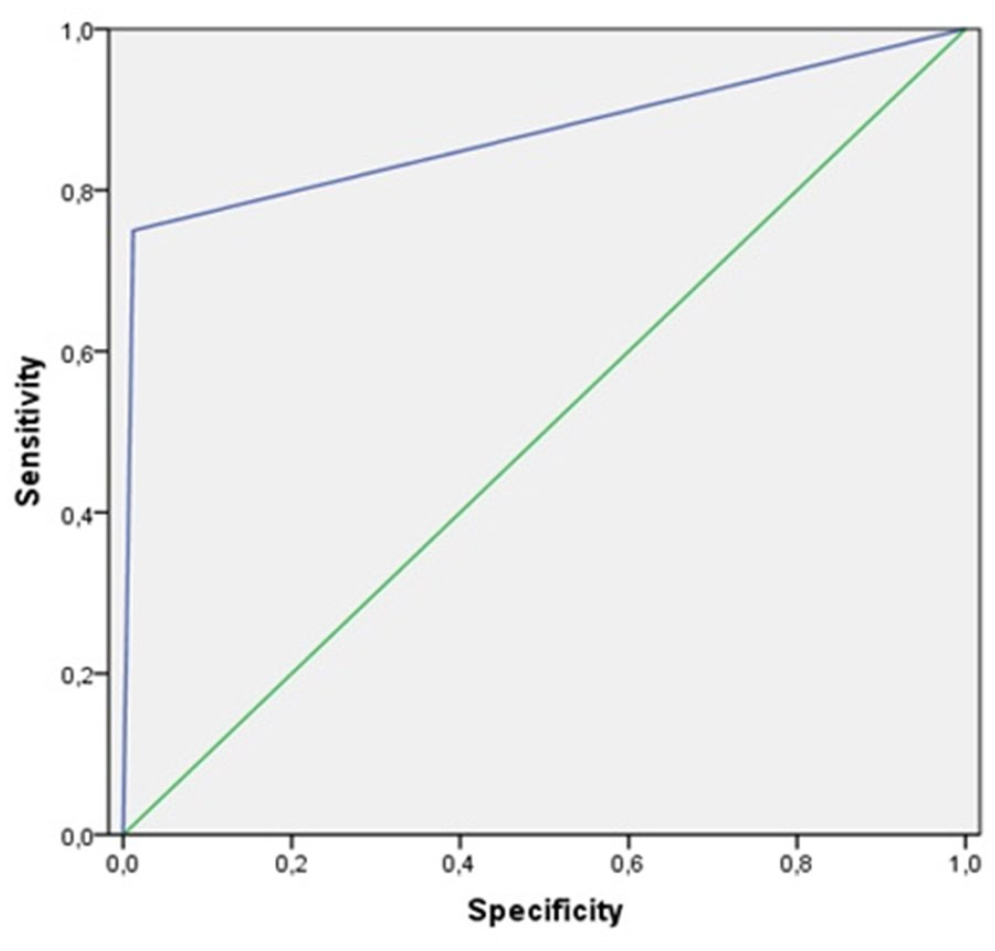
The receiver operator characteristic (ROC) curve analysis is provided based on the results of the ultrasonography examinations of this cohort of patients.
Discussion
Vocal cord paralysis is a feared complication of thyroidectomy. Therefore, intraoperative nerve monitoring (IONM) with surface electrode endotracheal tube is the standard method in thyroidectomy and it can be applied as intermittent (I-IONM) or continuous IONM (C-IONM). 16 Evaluation of VCs in the preoperative and postoperative period is important for the patient management plan. Early detection of recurrent laryngeal nerve paralysis (RLNP) after surgery provides immediate treatment for voice rehabilitation, potentially improving long-term outcomes, while preoperatively it helps identify baseline features and preexisting VCP. 17 There is no consensus on performing a routine VC assessment. Current guidelines recommend preoperative laryngeal evaluation only for patients with an impaired voice (based on patient feedback or rating scales) or high-risk patients (known VCP, previous neck or mediastinal surgery, local progressive malignancy, or major goiter). Postoperative evaluation is recommended only for patients with voice changes.18,19 Various methods have been described for monitoring RLN function and VC function, such as direct visualization of VC movement under fiber bronchoscopy, indirect laryngoscopy (IDL), tracheal palpation during RLN stimulation, or electromyography. However, US is a cheaper and noninvasive diagnostic alternative to these methods. 20 There are studies in the literature showing the success of US in assessing VC function after thyroidectomy, with a varied diagnostic range (33%–100%).9,11,14,21 One of the first studies was reported by Sidhu et al., 21 and although VCs from all the study patients were evaluated, the sensitivity was only 62%. The lack of real-time evaluation in their study may have influenced their results. In a study by Borel et al., 11 only 103 patients’ VC, in the early postoperative period, could be evaluated, which was 62.8% of their cohort; however, TLUS was found to have a sensitivity of 33% and an NPV of 95% for the postoperative diagnosis of VCP. Kandil et al. 9 reported that, of 250 patients, the rate of VC visualization was 50.6%. This study also found that VCs were more difficult to evaluate postoperatively in severely overweight and obese patients. Apart from these reports, the literature would suggest that TLUS is very successful in evaluating VCs and detecting VCP.10,13,22,23 In this study, a high success rate of approximately 97% was achieved in the visualization of VCs. Vocal cord paralysis could not be detected in only two patients, while a patient was misdiagnosed as having paralysis although the VC was normal. Male gender, ossification of the thyroid cartilage due to increased age-related calcification, and hematoma at the thyroidectomy site were described as difficult factors for the evaluation of VC. 17 While the mean age of this study’s cohort was 49 years, three of the patients with VC who could not be evaluated were older than 70 years. Most studies in the literature have described the use of postoperative TLUS, 1 to 10 days after surgery. In some studies, the evaluation took place on the first postoperative day or in the very early postsurgical phase.24 –26 Because problems such as edema, swelling, and pain may develop at this early phase, in this study TLUS was performed as a diagnostic monitor on the seventh postoperative day. In addition, it is predicted that adequate skills in TLUS can be acquired after having performed 40 US examinations. 23 In this study, an examination by an experienced radiologist on the seventh postoperative day may have influenced the diagnostic success rate. The main purpose of this study was to investigate the success of TLUS in detecting VCP. In this patient cohort, transient VCP was observed in eight (8.6%) patients, which is consistent with the literature.12,15,27 –29 Vocal cord paralysis was diagnosed by TLUS in six of these patients (sensitivity 75%), and a very strong correlation was found between TLUS and DFL in the assessment of VC motion (ρ: 0.78 and P < .001).
Limitations
This prospective cohort study had several limitations. First, the results are hampered due to the pre-experimental research design. In addition, the convenient patient sample was not sufficient to detect factors associated with VCs that could not be assessed using TLUS. There was also no application of quantitative measurements with Doppler is this study. Dedecjus et al. 28 found that the use of Doppler, in VC assessment, increased the success rate (sensitivity and specificity 100% and 95.7%, respectively). Finally, the procedures in this study were performed by a single experienced radiologist using 3- to 13-MHz ultrasound transducer. It is recommended to use a low-frequency transducer as other published studies have indicated that it has a higher assessment rate.
Conclusion
In this cohort of patients, TLUS was a reliable diagnostic tool to evaluate VC functions after thyroidectomy. It could be used as a safer diagnostic alternative during the ongoing COVID-19 pandemic because it does not produce human aerosols. Ultrasonography is a noninvasive, rapid, and inexpensive diagnostic choice, at the patient’s bedside, which are all advantages. Especially in nonobese young patients, successful results are obtained in applications performed 1 week postoperatively. This study would suggest that TLUS, with various technical modifications, may become the standard diagnostic procedure in selected patient groups, based on results of further detailed studies.
Footnotes
Informed Consent
Informed consent was not sought for in this study because all case data were de-identified and/or aggregated and followed ethics committee or institutional review board (IRB) guidelines (also referred to as the Honest Broker System)
Ethics Approval
Ethical approval was not sought for this study.
Animal Welfare
Guidelines for humane animal treatment did not apply to this study.
Trial Registration
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.