
Abstract
Laryngeal hemangiomas are rare vascular tumors that mostly present in children. The objective of this publication is to shed the light over this rare diagnosis. We report a case of adult onset of laryngeal hemangioma arising from the junction of the vocal fold and vocal process. The patient presented with a history of hoarseness of voice. An in-office laryngoscopy was performed that revealed a pink lobulated mass arising from the left hemilarynx. Intraoperatively, suspension microlaryngoscopy was performed; the lesion was identified and successfully resected using cold dissection technique. Histopathological analysis was consistent with laryngeal hemangioma. The patient is now a year post resection and remains asymptomatic without signs of recurrence. To conclude, adult onset of laryngeal hemangioma is very rare. When present, resection with either or both cold steel (microscissors) and laser have shown good outcome. Patients should be monitored afterwards for possible recurrence.
Introduction
Hemangiomas are benign vascular tumors with unknown etiology. They represent the most commonly diagnosed congenital benign tumors, and ∼60% arise in the head and neck region.1–3 Laryngeal hemangiomas are slowly developing vascular tumors,1,2 which are either children (infantile hemangioma) or adult hemagiomas.1,2 Infantile hemangiomas are more common in first 2 months of life. 4 Adult hemangiomas are more likely to be seen in men and are not considered progressive tumors but also do not regress spontaneously. 5 Small hemangiomas might simply be observed over time, while large hemangiomas may need treatment. 6 – 7
In adults, laryngeal hemangiomas are rarely encountered, with 27 patients in published reports in the English literature. 3 We report a case of an adult with glottic hemangioma that was successfully treated by surgery.
Case report
This case report received exemption from the institutional review board. An informed written consent was taken from the patient to proceed with reporting and publication of this case.
A 42-year-old male with no history of chronic disease, who was a nonsmoker and nondrinker, presented to the otolaryngology—head and neck surgery clinic complaining of voice hoarseness for 1 month and foreign body sensation that was not improving. His symptoms started after an episode of acute laryngitis that lasted for 5 days. One week later, he started to develop the previously mentioned symptoms. He did not complain of any choking attacks, dysphagia, hemoptysis, pain, neck swelling or cutaneous lesions. On physical examination, he was noted to have breathy and hoarse voice without stridor or work of breathing. A complete head and neck examination was performed, which was normal.
Stroboscopy was attempted but was not feasible due to an extremely sensitive gag reflex that was easily triggered by both nasopharyngoscopy and rigid laryngoscopy. During the limited examination, a lesion was noted in the larynx that looked round, likely pedunculated and likely came off of the left vocal fold process, with bilaterally intact vocal fold mobility.
The patient was taken to the operating room for assessment and surgical resection under general anesthesia. The patient was kept spontaneously ventilated without endotracheal intubation for the majority of the surgery. This was achieved using a combination of inhalant anesthesia and intravenous medications including propofol while avoiding the using of muscle relaxant agents. We utilized the Benjamin laryngoscope to suspend the larynx. After suspension laryngoscopy was performed, larynx examination revealed a pink, round, lobulated mass with a stalk originating from the junction of the left vocal fold and process (Figure 1).
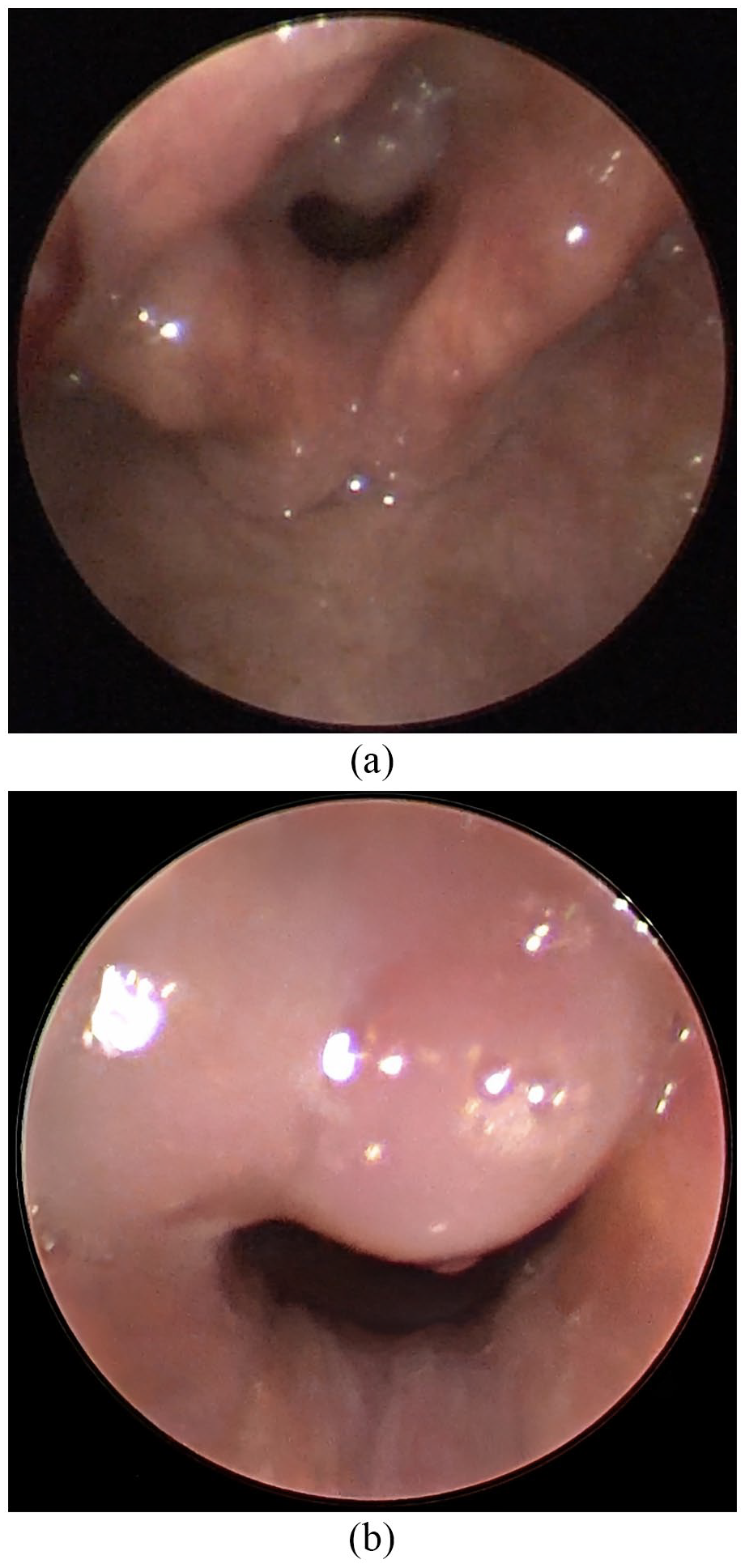
(a) A round, lobulated mass with a stalk originating from the left junction of the vocal fold and process. (b) Shows a close up image of the lobulated mass.
Full excision of the mass was performed using cold dissection instruments (Figure 2). Using left-facing grasping forceps, the mass was manipulated. Microscissors and spatulas were used to complete the dissection of the stalk. Adrenaline pledgets were utilized for hemostasis. At the end of the surgical intervention, the suspension was removed, and the patient was handed back to anesthesia and subsequently transferred to the recovery room.

A view after resection of the bulk of the lesion, revealed the origin of the stalk at junction of the left vocal fold and process. The stalk was resected afterwards.
The patient tolerated the procedure well and was discharged on analgesics, proton pump inhibitors, as well as voice rest. The patient returned to the clinic 1 week later with near-to-normal voice.
Histopathological gross examination of the specimen revealed a round, lobulated mass with a narrow stalk. Microscopic examination revealed surface stratified squamous epithelium with variable sized vascular spaces in the submucosa (inset) lined by benign flattened endothelial lining, which justified the diagnosis of laryngeal capillary hemangioma (Figure 3).

(a) Histopathology revealed surface stratified squamous epithelium. (b) This figure highlights the variable sized vascular spaces seen in the submucousa (inset) lined by benign flattened endothelial lining.
The patient is now 18 months post surgery and is asymptomatic. On a routine follow-up, an in-office laryngoscopy was performed that revealed no signs of recurrence. Although full stroboscopy was not possible to be performed due to the patients severely sensitive gag reflex, the patient reports voice returning back to his baseline voice prior to this condition happening.
Discussion
Adult onset laryngeal hemangioma usually occurs in the supraglottic region and presents with dysphonia, dysphagia, foreign body sensation and rarely hemoptysis. 1 In our case, hoarseness and foreign body sensation were the only two presenting symptoms.
The etiological and predisposing factors are not well understood and have been unconvincingly enumerated; the factors are thought to be smoking, vocal abuse, intubation and laryngeal trauma. 8 The case presented here did not have any of these factors, but rather an episode of acute laryngitis. This is an interesting finding as none of the previously published case reports describe an episode of acute laryngitis immediately prior to the onset of symptoms.
In previous studies, computed tomography (CT) and magnetic resonance imaging (MRI) have been found to be helpful in detecting the size, form, anatomical association and extent of hemangiomas. The results suggest that the use of CT, MRI and laryngoscopy will help in the delineation and diagnosis of laryngeal hemangiomas that have deep extensions. 9 In the present case, laryngoscopy was used to identify a mass that looked round, likely pedunculated and likely coming off of the left false vocal fold.
On a histological level, hemangiomas are formed of large, irregular, blood-filled channels lined with a single layer of endothelial cells between loose fibrous tissue septa of varying thickness. 10 Pathological examination is definitely required for definitive diagnosis. 9 Adult laryngeal hemangiomas can be classified as cavernous, which is most common, capillary or mixed. 11
Since there are only limited data available about adult laryngeal hemangioma, there are no well-established treatment protocols. Treatment options include endoscopic surgery with mixed approaches of microscissors and laser.2,3
In a study by Kazikdas et al., 12 capillary hemangioma was found on the anterior one-third of his right vocal fold and was successfully excised with microscissors without complications postoperatively. In another study by Laohakittikul and Srirompotong, 13 lobular capillary hemangioma was found at anterior half of left true vocal fold; excision with laryngeal carbon dioxide laser was done successfully. Similarly, we excised the lesion by cold steel surgery. The patient reported improvement in his voice quality, and 18 months later, he was still asymptomatic and without signs of recurrence.
Conclusion
In conclusion, adult laryngeal hemangiomas are rare, and their etiology is not well understood. In this case, endoscopic approach whether with microscissors was performed safely and without recurrence.
Footnotes
Acknowledgements
The authors do not have any acknowledgment to report for this manuscript.
Author contributions
R.R. contributed to the data collection, manuscript writing, revision editing, final manuscript review and production, and approved the final version. A.S. contributed to the data collection, manuscript writing, final manuscript review and production, and approved the final version. A.T.G. contributed to the data collection, production of figures, manuscript review and approved the final version. A.F.B. contributed to the data collection, manuscript writing, final manuscript review and production, and approved the final version. F.Z. contributed to the data collection, manuscript writing, revision editing, and final manuscript review and production.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article