
Abstract
Paroxysmal Vocal Cords Dysfunction(PVCD), also known as paradoxical vocal cord motion, is abnormal adduction of the vocal cords during inspiration. Like asthma, PCVD can be triggered by breathing in lung irritants, upper respiratory infection or exercise. However, unlike asthma, PCVD is not an immune system reaction and does not involve the lower airways. Treatment for the two conditions differs. Plasma lactate levels are usually associated with acidosis and an increased risk of poor outcome and are described in a number of disease states of circulatory and/or respiratory failure. In patients with psychogenic hyperventilation, high lactates are associated with hypocapnia and alkalosis and should not necessarily be considered as an adverse sign. We describe a case of a young patient with PCVD mimicking asthma with high plasma lactate and discuss the mechanisms involved.
Background
Paroxysmal Vocal Cords Dysfunction (PVCD), also known as paradoxical vocal cord motion, is abnormal adduction of the vocal cords during inspiration. Like asthma, PCVD can be triggered by breathing in lung irritants, upper respiratory infection or exercise. However, unlike asthma, PCVD is not an immune system reaction and does not involve the lower airways. Treatment for the two conditions differs. Plasma lactate levels are usually associated with acidosis and an increased risk of poor outcome and are described in a number of disease states of circulatory and/or respiratory failure. In patients with psychogenic hyperventilation, high lactates are associated with hypocapnia and alkalosis and should not necessarily be considered as an adverse sign. We describe a case of a young patient with PCVD mimicking asthma with high plasma lactate and discuss the mechanisms involved.
Case presentation
A 34-year-old female patient, known to have non-atopic asthma on regular steroid and salbutamol inhalers, montelukast and cetrizine tablets presented to the Emergency Department in respiratory distress which had worsened over a week. She had a recent history of frequent hospital attendance for management of similar mild to severe attacks labeled as asthma. Her current condition was unresponsive to steroids and nebulised bronchodilators at home. After 2 h in the emergency department managed as a case of status asthmaticus with salbutamol, ipratropium bromide, steroids, aminophylline and magnesium sulphate, she was transferred to the intensive care unit (ICU) for further management.
On arrival to the ICU, it was noted that her respiratory distress was accompanied by inspiratory stridor rather than expiratory wheeze which raised suspicion of upper airway obstruction.
Serial arterial blood gas results.
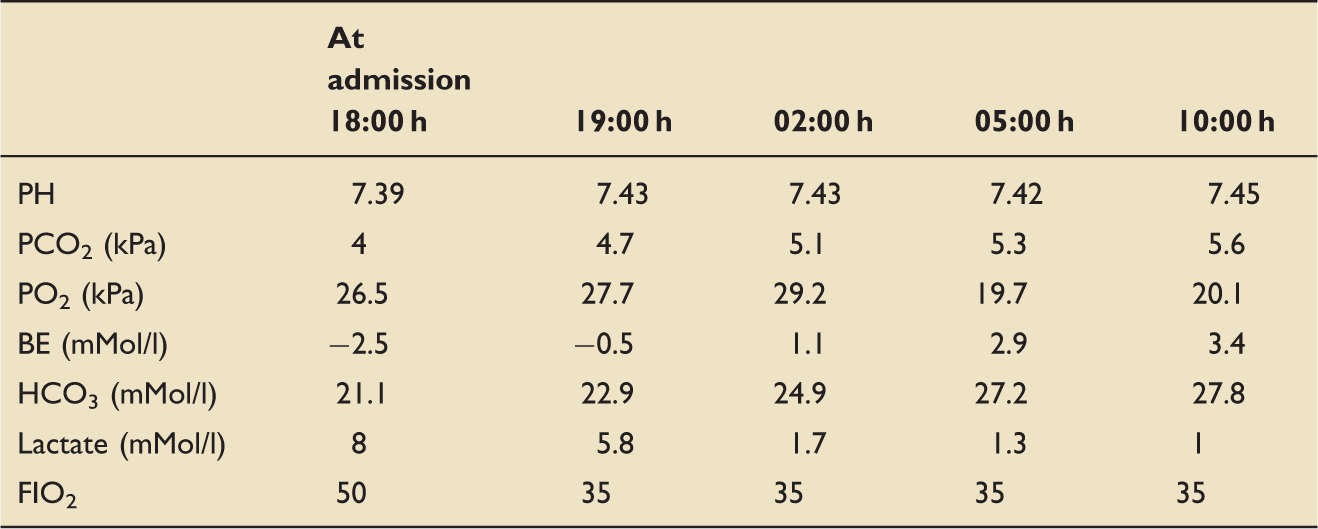
Awake fibre-optic laryngoscopy examination of the vocal cords was performed with full resuscitation and anaesthetic equipment at hand, revealing an in-drawing and adduction of the vocal cords on inspiration with no obvious pathology.
During the procedure, local anaesthetic with lignocaine spray and propofol sedation achieved immediate improvement in the stridor and concurrent normalisation of vocal cord movement, hence lowering of the respiratory rate and much improved chest wall excursion.
Arterial blood gas analysis showed a noticeable rise of serum lactate to 8 mmol/L; empirical antibiotic (co-amoxiclav) and fluid therapies were commenced.
Blood results showed Hb 131 g/L, WCC 14.3 × 109/L, platelets 245 × 109/L, neutrophils 13.2 × 109/L, total protein 65 g/L, albumin 4 g/L, conjugated bilirubin 9 µmol/L, ALT 14 µ/L, AST 60 µ/L and serum amylase 40 U/L.
The septic screen was negative and was associated with a lack of fever and negative sputum and urine cultures. The chest radiograph was reported as normal.
Further management included administration of lignocaine nebulisation, inhaled heliox, oxygen therapy and midazolam sedation during the acute attacks. By the next day, the serum lactate returned back to normal values correlating with the improvement in her condition.
Discussion
PVCD has been frequently described in the literature as inappropriate closure of the vocal cords upon inspiration with subsequent respiratory distress mimicking bronchial asthma.
Munchausen’s Stridor, Emotional Laryngeal Wheezing, Pseudo-asthma, Fictitious Asthma and Episodic Laryngeal Dyskinesia are different names depicting the gross similarity with bronchial asthma in terms of clinical presentation.
PVCD was seen to exist back in the 1800s (mistakenly called hysteria), and was written about in the medical literature in the 1970s. Later, PCVD was studied extensively by National Jewish Medical & Research Centre in Denver from the 1980s to 2014. Much confusion existed and still does, from the many different names given to PCVD and from the multi-factorial (many possible causes) nature of PVCD. 1
While the precise mechanisms have not been definitively established, it may be that the damage to the laryngeal mucosa leads to an accentuation of the glottic closure reflex, but this requires further study. This mechanism is also felt to be important in patients who develop PVCD after irritant exposures. Symptoms of PVCD include dyspnoea, wheezing, throat and chest tightness, and so PVCD is commonly mistaken for asthma. Stridor is frequently present, being loudest above the throat and less audible throughout the chest wall. Dysphonia and aphonia have also been described between attacks of respiratory distress. 2
Diagnosis of PVCD based on symptoms alone is inaccurate. In an asymptomatic period, physical examination will be normal. Chest radiography is typically normal; the features of hyperinflation and peribronchial thickening frequently seen in asthma are usually absent.
During symptomatic periods, spirometry can demonstrate a pattern of variable extrathoracic airway obstruction on the flow–volume curve (flattening of the inspiratory loop, but its sensitivity and specificity are low). 3
Direct visualization of the upper airway is the gold standard for the diagnosis of PVCD. We performed awake fibreoptic laryngoscopy having taken full precautions and preparation for emergency intubation if required. Diagnosis of PVCD was extremely challenging outside of an acute presentation, and we felt that our actions reduced the likelihood of future unnecessary interventions including steroid therapy and mechanical ventilation. 4 Flexible fiberoptic rhinolaryngoscopy allows evaluation of supraglottic and glottic anatomy, appearance of the laryngeal mucosa, and overall movement of the glottis in order to rule out other aetiologies. If performed during a symptomatic period, direct observation will classically show paradoxical inspiratory vocal cord adduction of the anterior two-thirds with a posterior diamond-shaped cleft. Greater than 50% inspiratory closure of vocal cords is sufficient for the diagnosis. Depending on the history obtained, provocation with stimuli known to induce symptoms as exercise or cold air can increase the diagnostic yield. 2
Optimal management of PVCD requires the identification and management of contributing factors. Short-term symptomatic control includes relaxation techniques such as pursing lips, panting, and relaxing the shoulders. If coexistent, appropriate treatment of asthma is crucial. Anxiolytics are helpful if the patient experiences severe anxiety attacks. Continuous positive airway pressure and heliox therapies have been reported to be effective in a small proportion of severely symptomatic patients; topical lidocaine applied to the larynx and superior laryngeal blocks with Clostridium botulinum toxin in selected cases have been attempted with variable success. 5
In our patient, the patient’s initial serum lactate was markedly raised. Lactate is formed in vivo as one of the end products of glycolysis. The metabolic pathway known as glycolysis is the first step of glucose metabolism and occurs in the cytoplasm of virtually all cells. By this pathway, glucose is converted into two pyruvate molecules. The pyruvate formed can be fully oxidised to CO2 under aerobic circumstances by oxidative phosphorylation in the mitochondria. Alternatively, particularly in the absence of oxygen, pyruvate can be converted by the enzyme lactate dehydrogenase to lactate. 6
Hyperlactataemia has been shown to be present in various severe disease states, such as sepsis, cardiac arrest, and hypovolaemic shock. In these conditions, plasma arterial lactate levels are a very important independent outcome predictor, and elevated lactate levels are increasingly used for early detection and treatment for patients with impaired haemodynamics. As a result, many physicians consider lactate as a deleterious metabolite.
Huckabee et al. studied the phenomenon of hyperventilation-associated hyperlactataemia extensively in the 1950s and 1960s and believed it to be a benign process because the lactate-to-pyruvate ratio did not change, which would be indicative of the absence of an oxygen debt. 7
Avest et al. studied 46 patients diagnosed with psychogenic hyperventilation; 14 participants showed a rise in serum lactate above the reference range with no adverse events or requirement for medication. 6
Lactic acid production decreases when intracellular pH is low (acidosis) and increases when intracellular pH is high (alkalosis). This effect of pH on lactic acid production provides a homeostatic mechanism for generating hydrogen ions to rapidly counteract a state of intracellular alkalosis. As CO2 is a source of acid that rapidly crosses cell membranes, the respiratory alkalosis resulting from hyperventilation-induced hypocapnia causes an immediate intracellular alkalosis. Metabolic alkalosis can cause a delayed intracellular alkalosis. 6
In their review of experimentally induced changes in acid–base status, Hood and Tannen found that 12 of 12 studies of respiratory alkalosis and 12 of 15 studies of metabolic alkalosis observed an increase in net lactate production. In contrast, they found that three of three studies of respiratory acidosis and seven of nine studies of metabolic acidosis reported a decrease in net lactate production. The regulatory effect of pH on lactate production is modulated by the concentration of high-energy phosphates and the availability of glucose as a substrate for glycolysis.
Brautbar et al. showed that a combination of hyperventilation-induced respiratory alkalosis and a continuous glucose infusion led to a five-fold increase in serum lactate after 60 min in dogs. This increase in lactate was attributed to the disinhibiting effect of alkalosis on glycolysis, as there was no evidence for intracellular hypoxia or high-energy phosphate depletion. 8
These studies demonstrate that the homeostatic response to alkalosis can lead to substantial increases in lactate levels in the absence of any shortfall in oxidative metabolism. However, it should be noted that in patients with critical illnesses, lactate is a risk marker not a risk mediator: several studies have shown that the administration of exogenous lactate is safe or even beneficial. 9 Lactate can be reused directly as a substrate to generate adenosine triphosphate by many organs, including the heart, the brain and the kidneys. Therefore, it has been suggested that the hyperlactataemia of hyperventilation serves as a favourable metabolic compensatory process during respiratory alkalosis. 10 The exact reason for the hyperlactataemia of hyperventilation will remain a topic of teleological debate.
Our case study is the first to describe the presence of hyperventilation-related hyperlactataemia in a case of paroxysmal vocal cord dysfunction, and although PVCD is not a frequent entity, it should be kept in mind in order to avoid misdiagnoses and unnecessary and possibly harmful medication. One should not forget that although less frequent, PCVD can occur in asthmatic patients. Obtaining a careful history and determining triggers are important in order to establish a correct diagnosis and implement proper treatment. Importantly, a raised lactate in such cases may not represent severe underlying pathology.
Consent
This report is published with the written consent of the patient.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.