
Abstract
Objective:
The purpose of this study was to determine the current scope of practice of sonographers in the United States and ascertain if sonographers’ daily responsibilities align with the Society of Diagnostic Medical Sonography’s (SDMS) Sonographer’s Scope of Practice and Clinical Standards.
Materials and Methods:
A survey was disseminated to SDMS members and clinical sonographers with at least 5 years experience. The survey addressed demographics, education, certification, specialties practiced, job title, work environment, and scope of practice.
Results:
Of the 613 sonographers who responded, 90% were female and 10% male; the most common age group was 55–64 (36.7%). Most sonographers had a Bachelor’s or Associate’s degree. Eighty-three percent of respondents were White, 5.4% Hispanic, Latino, or Spanish origin, 3% Black or African American, and 3% Asian. While 63% of sonographers have read the SDMS Scope of Practice, 52% reported they perform tasks not included or addressed, in their job description. Many teach sonography in the workplace and provide oral and/or written preliminary impressions and diagnoses.
Conclusion:
There are regional differences in scope of practice and gender differences in place of employment and job title. Sonographers reported to practice within the SDMS parameters. The guidelines can be expanded to include educating health professionals in sonography and having an increased role in providing diagnoses.
Diagnostic medical sonography is a multi-specialty field, focused on the use of ultrasound application, for medical diagnosis and treatment. A diagnostic medical sonographer is a health care professional who uses non-invasive, high resolution, ultrasound to image organs, tissues, and vascular structures within the body. Sonographers assist physicians in detecting and diagnosing pathology and also provide ultrasound guidance for invasive procedures. There is great variability in the level of training and education of sonographers across the United States. 1 Although there are national organizations, including the American Registry of Diagnostic Medical Sonography (ARDMS), and the American Registry of Radiologic Technologists (ARRT) that administer examinations and award credentials, 2 there is no federally mandated credentialing requirement or established minimal educational requirements necessary for sonographers to perform examinations in the United States. 3 Many outside the field of sonography do not realize that there are no federal laws requiring licensure for sonographers. 4
The ARDMS has provided information on how licensure differs from certification, noting that licensure is generally required by the government in order to practice a specific profession, but certification is a voluntary way to show objectively measured competence. 5 Certification is usually awarded by professional organizations and demonstrates a person has achieved entry level competency in specific knowledge and skills. According to the American Society of Echocardiography (ASE), licensure regulations define the professional scope of practice, the minimum training requirements to practice, and is considered to be the legal permission to practice. 6 Wilson & Wilson compared and contrasted certification, occupational licensing, and professional certification, and explained that a state requiring licensure usually has a licensing board with political appointees to oversee the guidelines required, and ethical standards. 4 It also identifies any restrictions that would exclude certain people from working in occupations that require public trust. 4 Wilson explains that creation of licensure regulations includes minimal educational standards, qualifications, and guidelines establishing professional standards of practice, to ensure that members of the public obtain safe health care. 4 Licensure is handled at the state government level, as opposed to the federal government level. To date, only four states require licensure of sonographers (New Hampshire, New Mexico, North Dakota, and Oregon). 7
Many sonographers use the term registered or certified synonymously. Registry certification is generally awarded to sonographers after successful completion of examinations on specific subjects, usually by the ARDMS, ARRT, and/or the Cardiovascular Credentialing International (CCI). Hospitals and medical facilities generally look to hire sonographers with credentials, as this indicates a minimum level of competency.3,8 If the imaging department or facility is accredited by an independent agency, many of these organizations require sonographers on site to have ARDMS, CCI, and/or ARRT credentials. 3
History of Sonography as a Profession
The American Medical Association’s Manpower division created the occupation of the diagnostic medical sonographer; diagnostic medical sonography was first recognized as an occupation by the United States Office of Education in 1973.9,10 Although the sonographer was originally called an ultrasound technical specialist in the 1960’s during the infancy of sonography as a profession, the term “ultrasound technologist” was then more commonly used, 11 and the term “sonographer” was introduced in the 1970’s for those with an ARDMS credential. 12 The title “vascular technologist” is frequently used for those practicing in the vascular lab. The Bureau Labor of Statistics first recognized diagnostic medical sonography as a profession independent from radiologic technology in 2002. 12
Scope of Practice
The occupation and career of the diagnostic medical sonographer has evolved and grown over time. While the first generation of sonographers were trained on the job, today formal educational programs are the norm. 10 The use and application of sonography as a diagnostic tool has expanded into nearly every specialty of medicine, and along with that, professional opportunities, education, and responsibilities of the sonographer have grown.
When the profession first emerged, the sonographers’ responsibility was to apply physics and instrumentation to produce static images, but the physician was responsible for ascertaining the relevant information. 1 Diagnostic sonography of the brain and gallbladder was performed as early as the 1940’s, however the first commercial ultrasound equipment systems became available in 1963, 11 marking the beginning of its availability in the hospital setting. The technology and applications of sonography continue to advance and expand. Today, all sonographers must have a strong working knowledge of anatomy, physiology, pathology, and sonographic physics in order to obtain, analyze, and interpret real time images, select appropriate diagnostic and relevant ones, and provide preliminary impressions. Sonographers must use independent judgment and interact with other health care providers in a consultative capacity, using cognitive, affective, and psychomotor skills while providing care for patients.1,13 Baker noted that unlike other medical imaging applications, sonography is operator dependent, and sonographers must be able to interpret each image, in order to obtain the remaining images, as part of a clinical study. 10
As the technology advanced and more specialties of medicine incorporated sonography as a diagnostic imaging application, the scope of practice for sonographers grew. The Society of Diagnostic Medical Sonography (SDMS) was established in 1970. Their goal was and continues to be “to promote, advance, and educate its members and the medical community in the science of diagnostic medical sonography.” 14 The SDMS developed and published the Scope of Practice for the Diagnostic Medical Sonographer in 1993. 15 It was updated in 2000 with the title “Scope of Practice for the Ultrasound Professional” endorsed by the ARDMS, ASE, CCI, SDMS, Society for Vascular Surgeons, and Society for Vascular Ultrasound.¹⁰ Considered a “living document,” it was updated between 2013 and 2015, with the consensus of sixteen medical ultrasound related organizations, and entitled, “Scope of Practice and Clinical Standards for the Diagnostic Medical Sonographer.” 16 It is subject to change as needed. The 2015 document lists the participating and supporting/endorsing organizations, defines the purpose of the document, provides a definition of the profession, and addresses their position on competency and certification. It describes clinical standards, dividing them into four sections. Section one of the document is used to address patient care, while section two describes quality care, assurance, and improvement, with section three providing self-assessment, education and collaboration, and finally, section four codifies professional ethics. The document is easily accessible to all sonographers and can be found on the SDMS website as a downloadable pdf. 16 Prior to the internet, access to these guidelines were limited.
Significance
There is a considerable gap in the literature addressing what sonographers actually do on a daily basis, and if it differs by gender, region, title, years of experience, or type of clinical setting.
The purpose of this study was to ascertain if sonographers were aware of the SDMS Scope of Practice and Clinical Guidelines, if they perform responsibilities mentioned within the document, what the demographics of sonographers currently are in the United States, their attitude regarding education and credentialing, and their current scope of practice.
Materials and Methods
This study was a cross-sectional study designed to investigate what sonographers reported as part of their daily practice, in the workplace. It was designed to examine and explore on the reported scope of practice of sonographers, taking into account geographic region, type of facility, gender, experience, and specialty.
A 40-question survey created with Qualtrics software (Qualtrics, Provo, UT) was distributed electronically via the SDMS, to members who were clinical sonographers with at least 5 years of experience, residing in the United States. Sonography students, educators, retired sonographers, and sonographers with less than 5 years experience were excluded from the study. There were no incentives offered for participating in the study. The survey was reviewed by experienced sonographers and researchers prior to its use. This study was reviewed and approved by the State University of New York Downstate Health Sciences University Institutional Review Board. The survey invitation was deployed via email, and remained open for 1 month (March 8 to April 5, 2021). Invited SDMS members were sent a reminder 2 weeks after the initial dissemination of the survey invitation. Approximately 10 362 potentially eligible members were invited to participate in the survey.
The survey addressed demographics, educational background, certification, employment setting, specialties practiced, job title, work environment, job satisfaction, and scope of practice (see Table 1). Descriptive statistics and cross tabulations were used to analyze the data for this study.
A sample of the survey questions regarding Sonographer’s scope of practice.
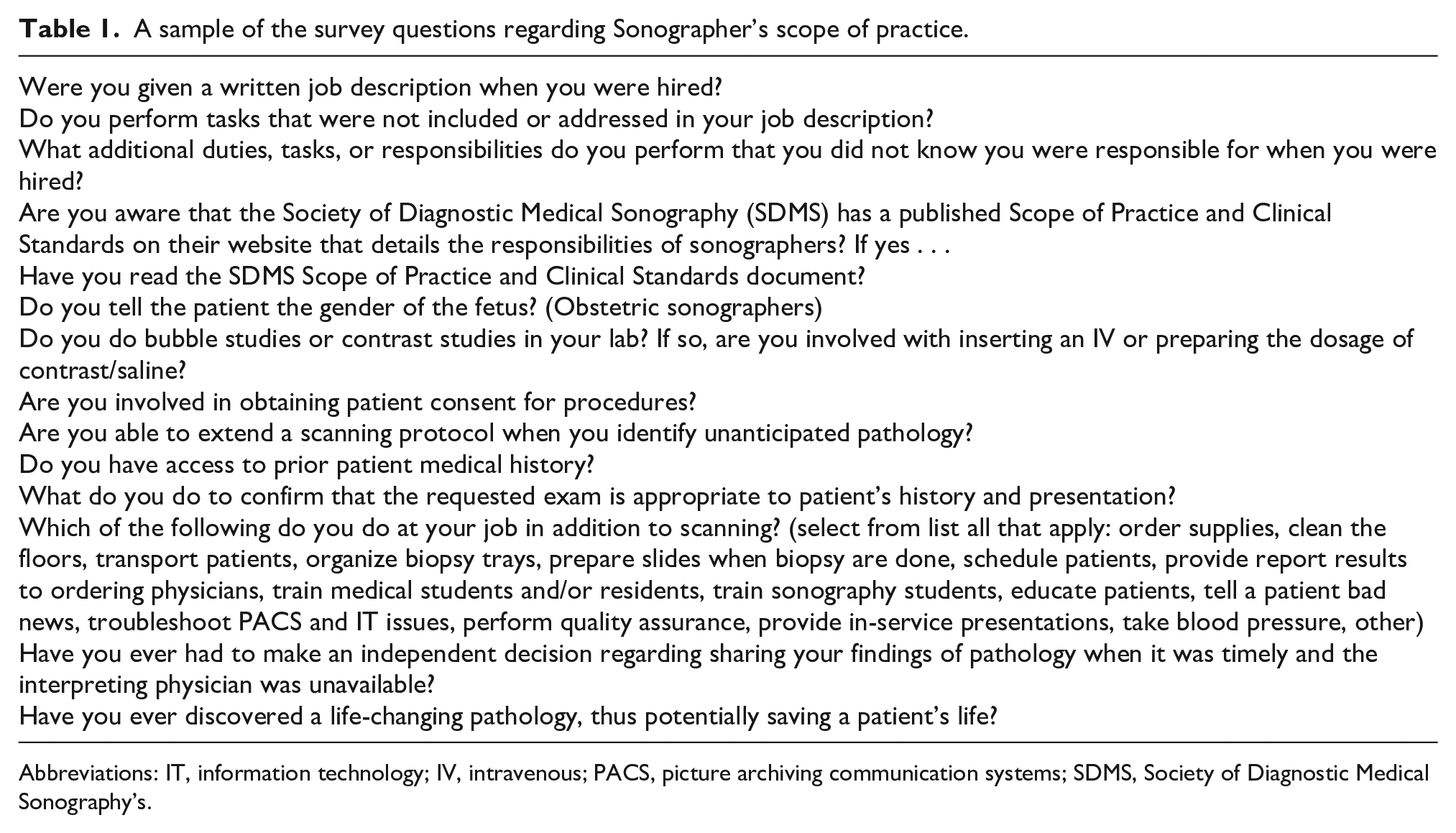
Abbreviations: IT, information technology; IV, intravenous; PACS, picture archiving communication systems; SDMS, Society of Diagnostic Medical Sonography’s.
Results
Six hundred and thirteen sonographers responded to the survey, with participants representing all states except Arkansas, Delaware, Rhode Island, and Washington D.C. (See Figure 1). The response rate was 6% (613/10 362). Twenty-three respondents no longer reside in the United States and their responses were removed from the aggregate data (n = 590). The five states with the highest response rates were California, Florida, Texas, New York, and Illinois.
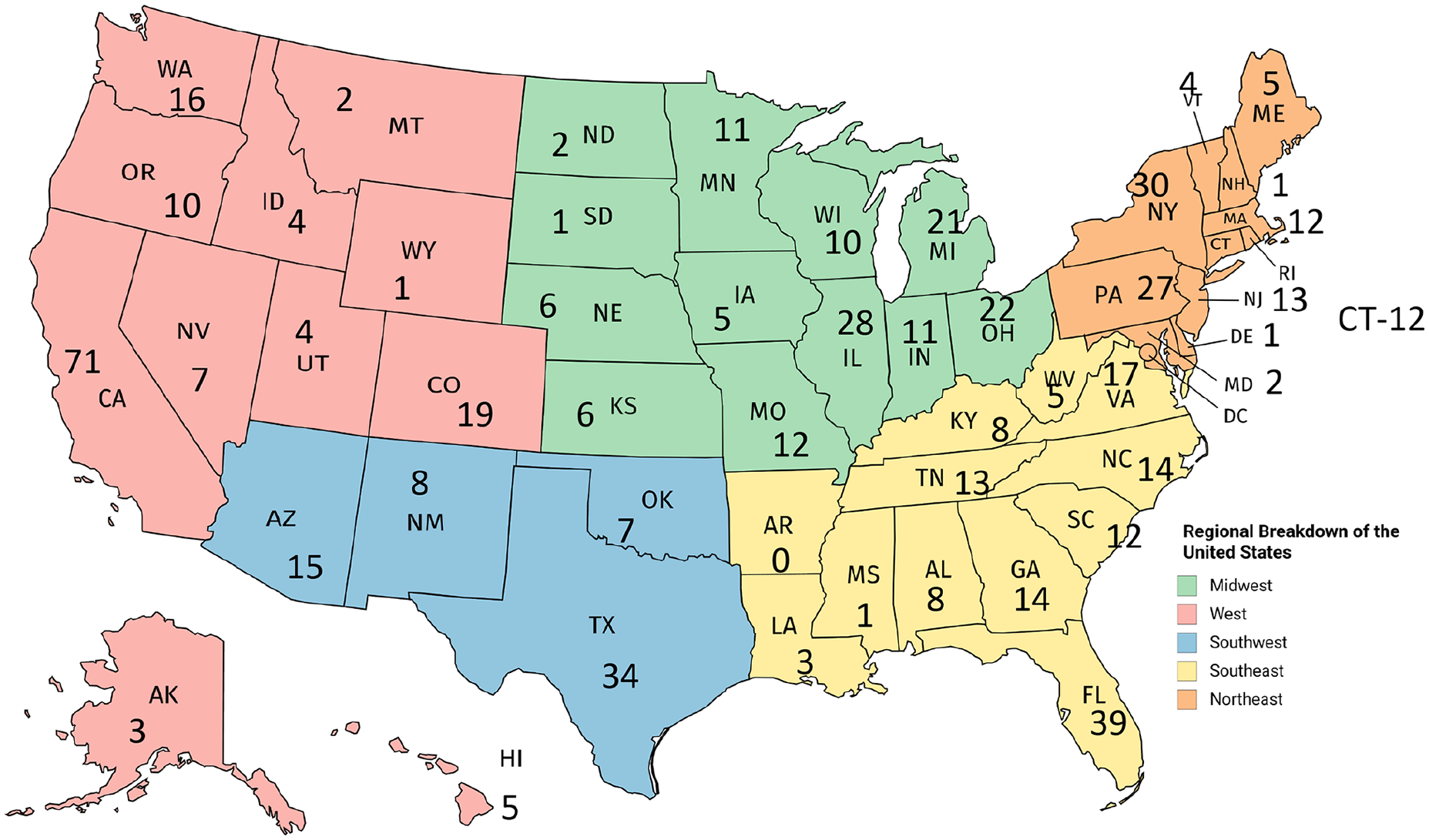
A map which indicates the number of survey respondents, based on the individual state.
Demographics
90% of respondents identified as female, while 9.7% identified as male. One participant chose “prefer not to answer,” with regard to selecting gender. The most reported age group was 55 to 64, followed by 45 to 54 years (See Figure 2). Eighty-three percent of respondents identified as White, 5.4% Hispanic, Latino or Spanish origin, 3% Asian, and 3% African American. Most sonographers responding to the survey are employed full time (71%), working in a variety of health care settings (see Figure 3).
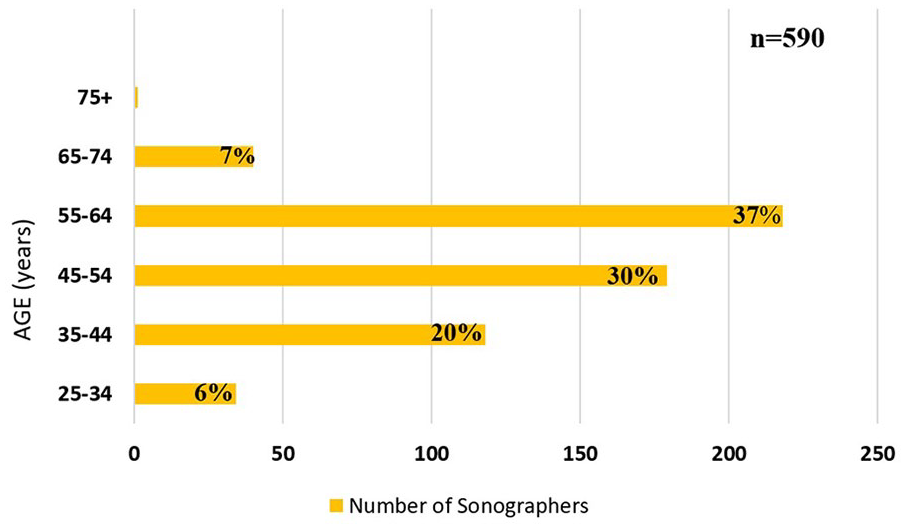
A bar chart that provides the age ranges of sonographers, responding to the survey.
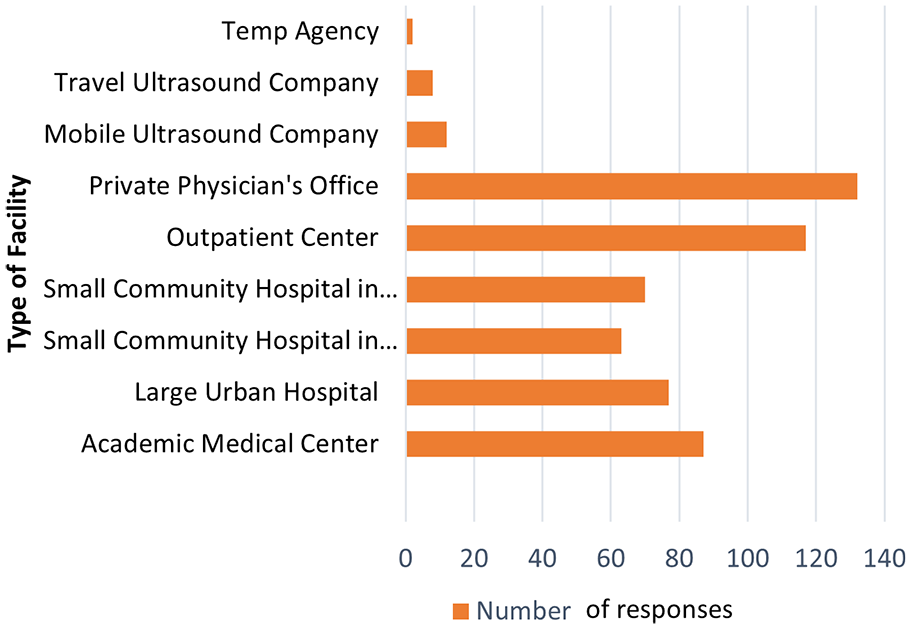
A bar chart that indicates the participating sonographers primary place of employment.
Based on the results of this survey, the most commonly reported workplace for males was an academic medical center (20%) or a large urban hospital (20%); females were most likely to work in an outpatient center or private physician’s office (21% and 23%, respectively). Males were more likely to work for mobile companies than females (10% as compared with 3%).
Work Environment
Most sonographers responding to this survey are employed as staff sonographers (51.8%), working in accredited sonography labs (64%) (see Figure 4). There was a regional difference in accreditation status of sonography labs; the Northeast reported that 91% work in accredited labs, as compared with the other regions of the United States that reported a rate of 55% to 60% (See Table 2).
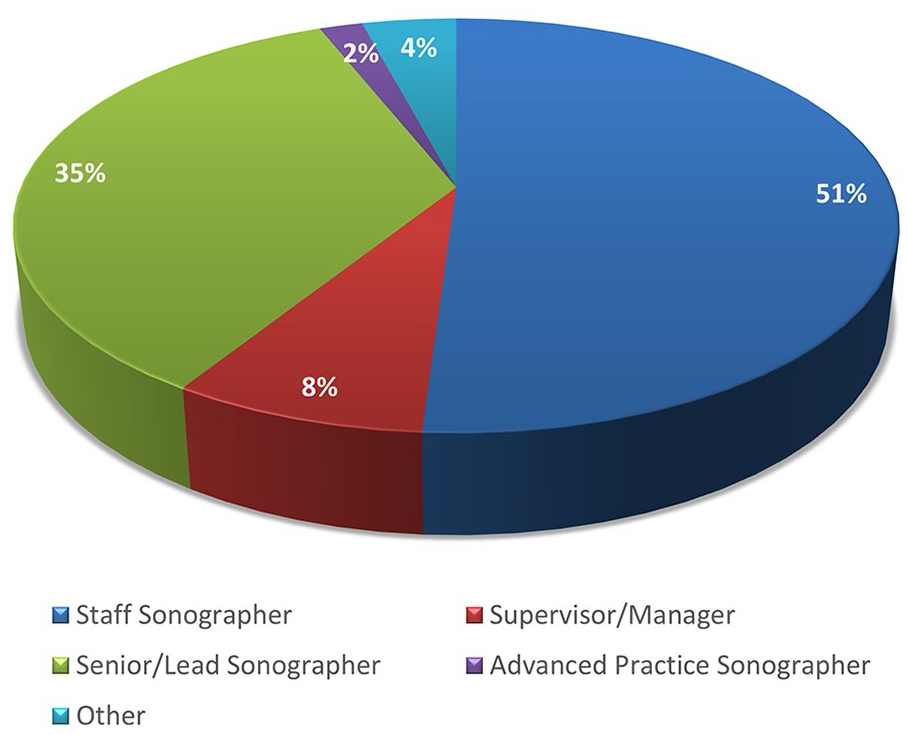
A pie chart that provides the respondents’ selection of job titles.
The Reported Lab Accreditation Status of Sonography Practices Based on Regions of the United States.

Most sonographers who responded to the survey were currently practicing abdomen, obstetrics, gynecology, vascular, and small parts sonography (See Figure 5A). Many sonographers performed sonograms in more than one type of specialty. Generally, sonographers were credentialed in the clinical specialties that they practiced (see Figure 5B). Of responding sonographers, 98% believe ARDMS/CCI/ARRT credentials are important. There were some gender differences noted across the clinical specialties that sonographers reported practicing (see Table 3).
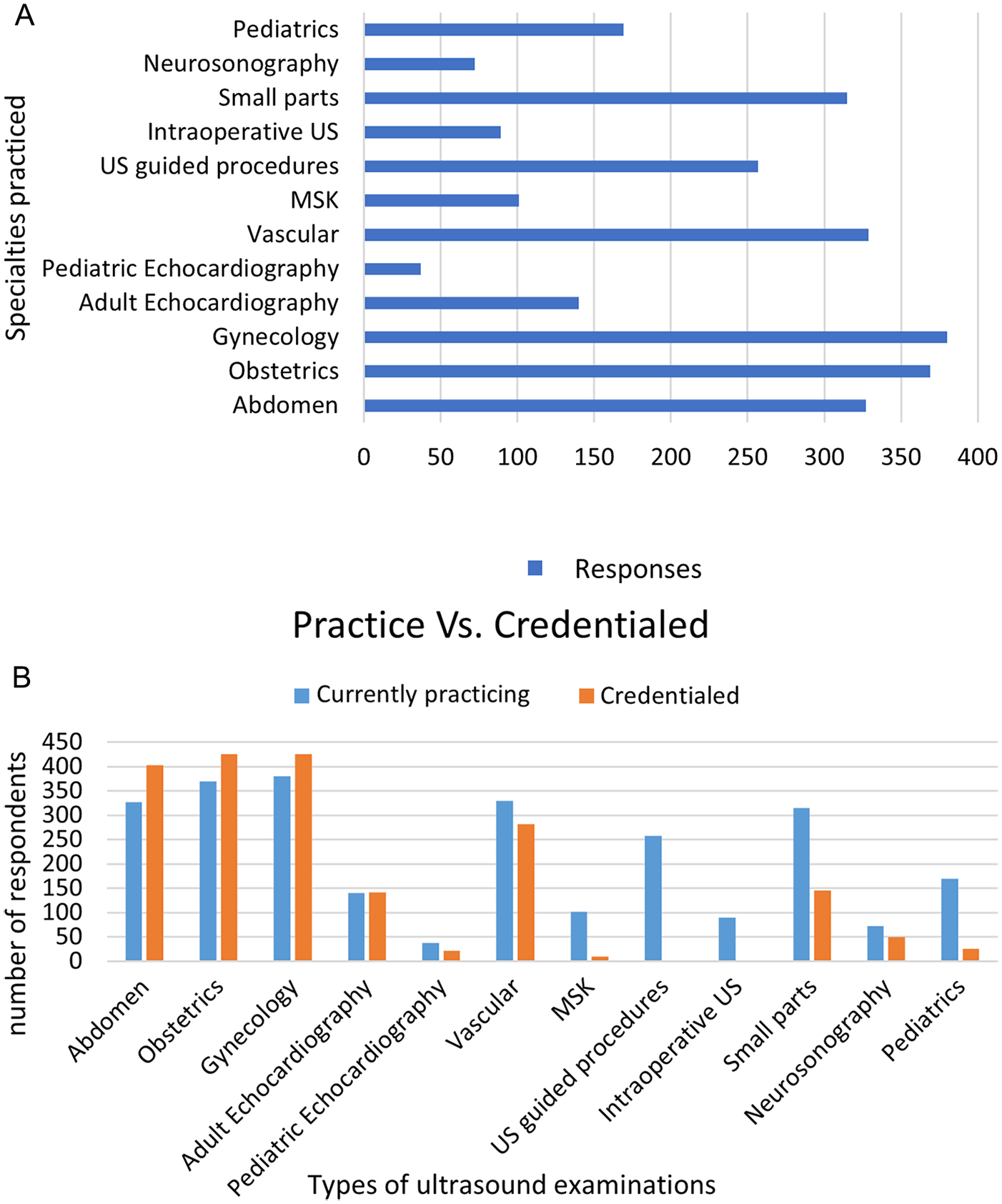
(A) A bar chart that indicates the clinical specialties that participating sonographers chose as their current work practice. Survey participants had the option to select more than one type of clinical specialty. (B) A bar chart that provides a comparison of sonography credentials, obtained by the responding sonographers and the current clinical specialties practiced. MSK, musculoskeletal ultrasound.
The Clinical Specialties That Sonographers Reported Practicing, Based on Their Gender.
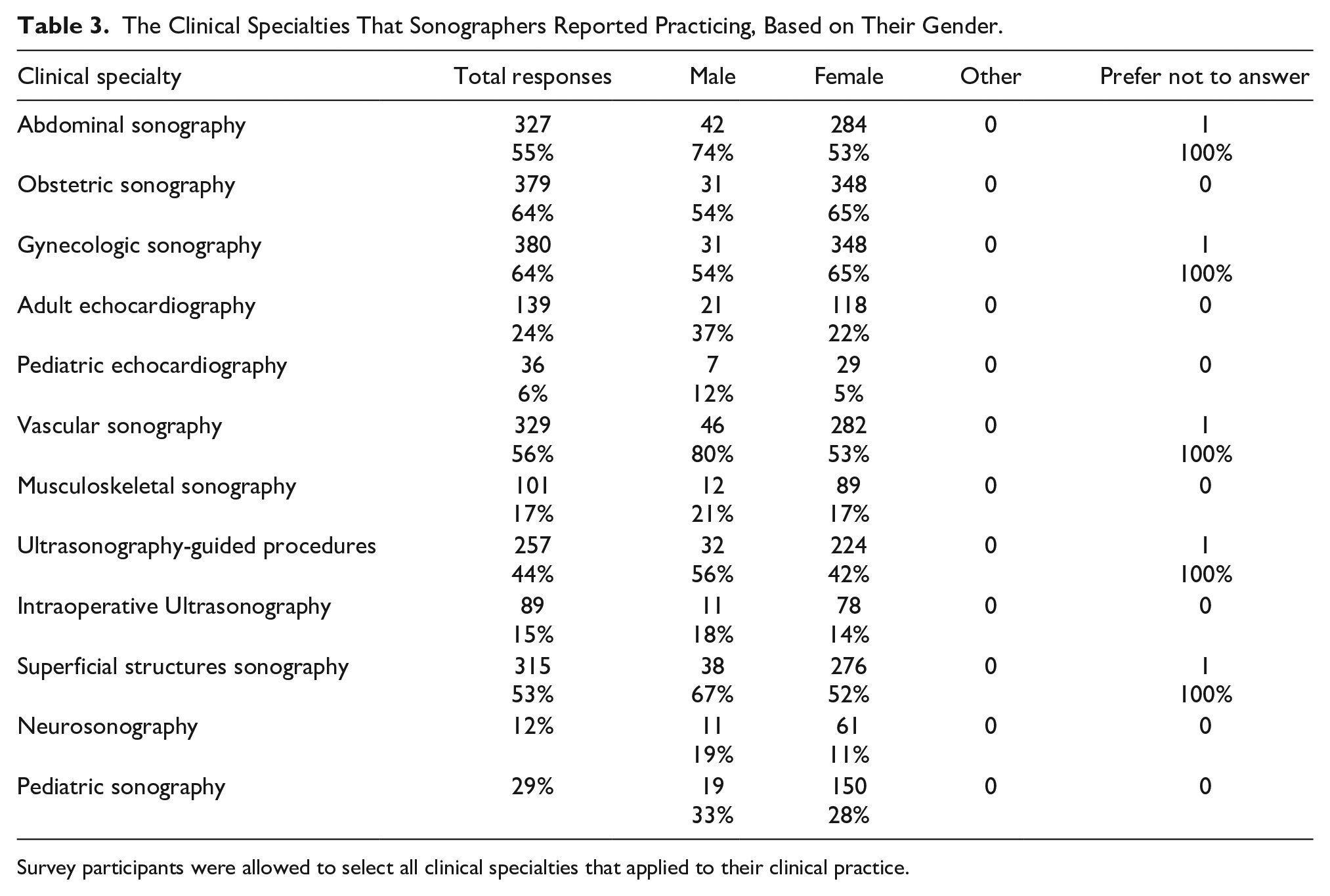
Survey participants were allowed to select all clinical specialties that applied to their clinical practice.
The average survey respondent had been working for 23 years. Of those who responded to this survey, 53% of males held the title of senior sonographer compared with 33% of female respondents. During an average 8-hour workday, 54% of the sonographers responding reported performing six to 10 patient cases a day and that was compared with 30% of respondents reporting that they completed 11 to 15 patient cases. These sonographers reported performing multiple types of sonographic studies, so it is not possible to analyze case numbers per day by clinical specialty. When asked if they felt they had adequate time allotted in a day to examine all patients on the schedule, 72% of sonographers reported often or sometimes, however only 14% reported always. Regarding workload in an average 8-hour workday, 53% of sonographers reported that their managers did not understand how much time was needed to perform each type of sonogram. Sonographers generally had access to a patient’s prior medical history (80%) and did review the patient’s chart, as well as ask the patient their symptoms.
Education
Sonographers reported that they believed the level of responsibility of the job of a sonographer best reflects a bachelor’s degree (56%), and 89% believed sonography programs should grant sonographers a college degree (see Figure 6). Thirty-nine percent of the responding sonographers reported having been awarded a bachelor’s degree, and 38.5% an associate’s degree (See Figure 7).
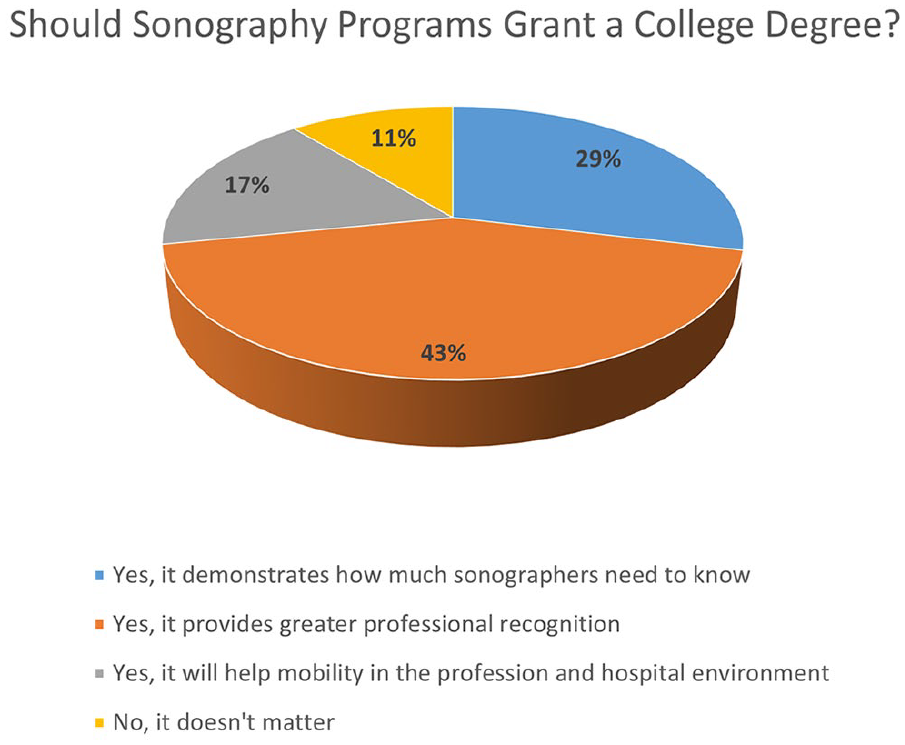
A pie chart that provides the reported attitudes of sonographers with regard to a college degree, in sonography.
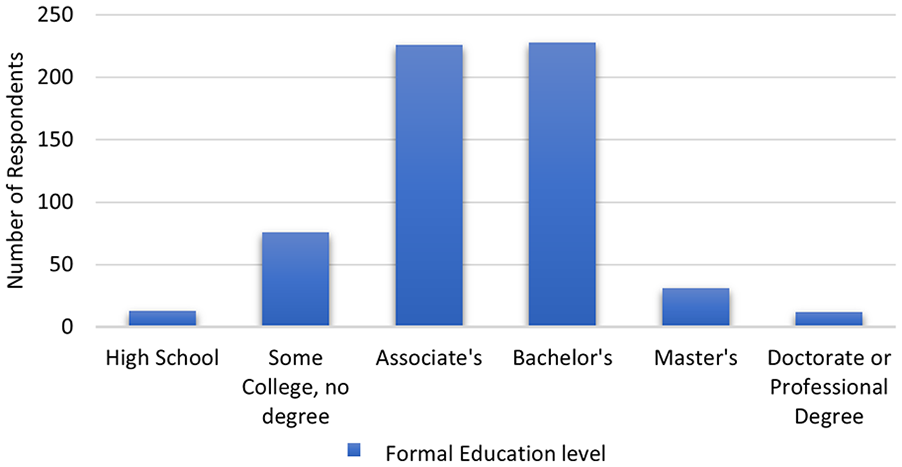
A bar chart that indicates the highest level of education obtained by those sonographers, who responded to the survey.
The most common and highest educational degree granted to those surveyed was an Associate’s degree (40%). Ninety-eight percent of respondents indicated that certification is important and reported holding multiple sonographer credentials.
Scope of Practice
Most of the sonographers surveyed were aware that the SDMS has a published Scope of Practice and Clinical Standards, posted on their website that details the responsibilities of sonographers. There were 63% of participants indicated that they knew about this document, and of that group, 63% had read the document. These responses were also analyzed by geographic region; The Northeast, Midwest and South regions demonstrated that those respondents knew about the scope of practice, within a range of 65% to 67%; sonographers in the Western region of the United States reported 55% knowing the document existed.
Sixty-three percent of sonographers participating in this study were provided with a job description upon hire, and 12% did not recall if they had received one. Of those who did receive a job description, 52% reported they perform tasks not included or addressed in the job description. The most common additional responsibilities not included in job descriptions were as follows: Educating patients, troubleshooting Picture Archiving Communication Systems (PACS) and/or information technology issues, performing quality assurance, organizing biopsy trays and slides, scheduling and office tasks, accreditation, teaching students, obtaining EKG’s, taking blood pressure, collecting specimens, IV insertion, insurance details, and ordering supplies.
The obstetric sonographers, who completed the survey, indicated that 82% revealed the gender of the fetus, during their examination. Sixty percent of the responding sonographers, from various specialties, were involved in obtaining informed consent from patients for procedures. Ninety-seven percent of all participating sonographers reported discovering life-changing findings on their sonographic examinations. Nearly all responding sonographers (99%) provided preliminary impressions to the interpreting physician, with varied methods. Thirty-seven percent of sonographers reported sharing the preliminary impression by digitizing a form into a PACS system with no communication with physician. There were 16% who reported verbally to the physician and 19% that provided a written preliminary impression. Finally, there were 27% who reported combinations of verbal, written, PACS, integrated reports, within the ultrasound equipment system and electronic health record reporting systems. Sonographers reported being able to extend an examination protocol when identifying unanticipated pathology (94%). While only 67% of respondents reported positive clinical findings when the interpreting physician was not available. It is interesting to note that by workplace, 76% of respondents working in a small community hospital, in a rural area, reported making independent clinical decisions and reporting timely positive clinically diagnostic findings.
Only 24% of sonographers participating in the survey reported working in a clinical laboratory that used contrast for sonography examinations. However, for sonographers working in clinical labs that do use contrast or perform bubble studies (agitated saline), 44% reported being involved in inserting an intravenous (IV) or preparing the dosage of contrast/saline, but 45% reported that the nurse is responsible for this procedure. There were regional differences in responses regarding sonographers’ involvement with IV insertion and preparing doses of contrast (see Table 4).
The Responses Based on Geographic Regions With Regard to Differences in Intravenous (IV) Contrast Procedures.
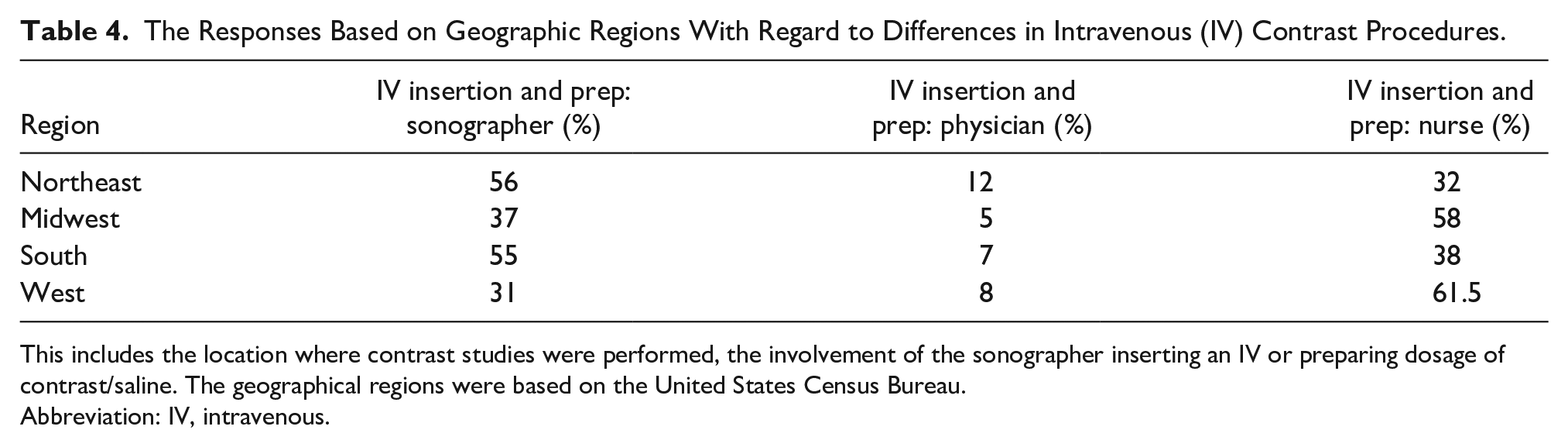
This includes the location where contrast studies were performed, the involvement of the sonographer inserting an IV or preparing dosage of contrast/saline. The geographical regions were based on the United States Census Bureau.
Abbreviation: IV, intravenous.
Sonographers were asked to rank the most common challenges on the job, from least likely to be a challenge to most likely to be a challenge. The sonographers responding, indicated that they experienced overbooked schedules and not enough pay, as their main work concerns (See Figure 8).
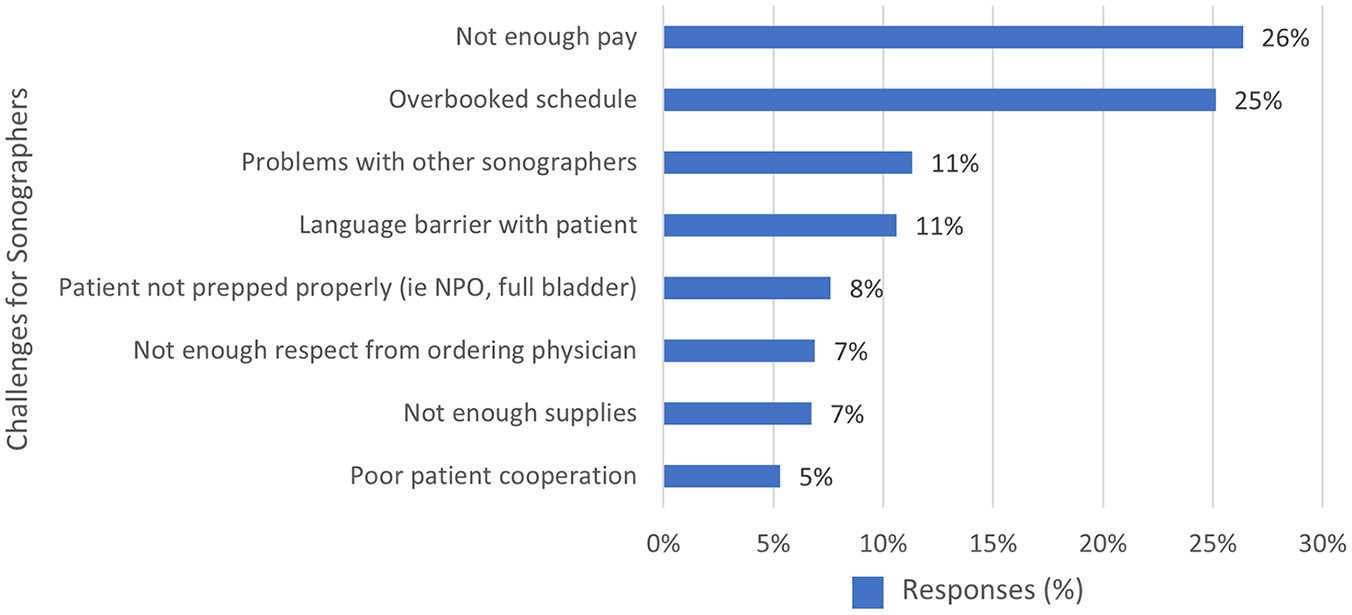
A bar chart including the responding sonographers most common challenges that they encounter in their workplace.
Impression of the Profession
Almost all participants in the survey reported being satisfied that they had chosen to become a sonographer (95%). Ninety-three percent reported that the job as a sonographer meets, exceeds or far exceeds their expectations, and gave many reasons for choosing the field of sonography (See Figure 9).
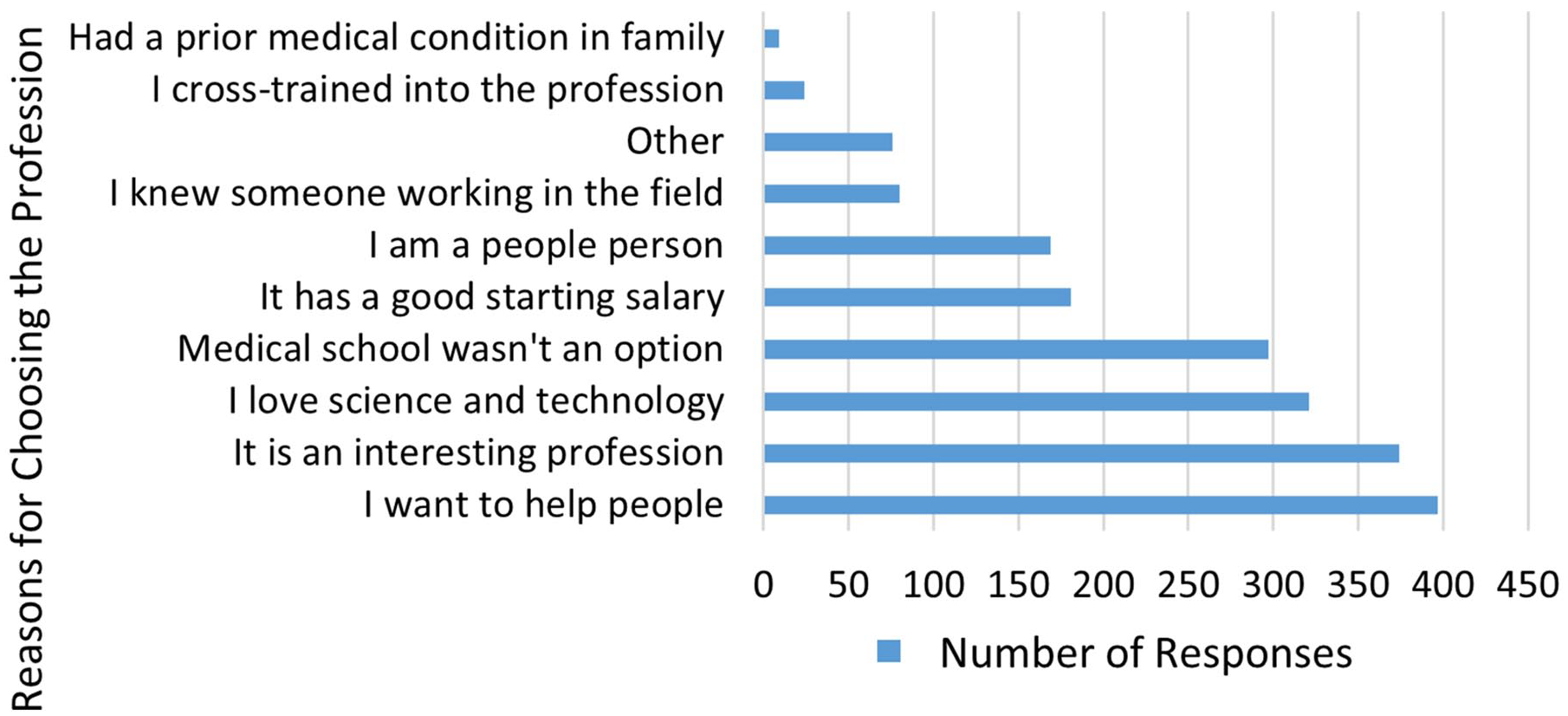
A bar chart that provides the responding sonographers’ reasons for choosing a sonography career. The respondents were able to select multiple responses to this question.
Discussion
Sonography has its roots in the radiology department, and many of the first generation of sonographers experienced “on the job” training. 17 Many sonographers originally cross-trained from other positions in radiology and cardiology, during the infancy of the profession. A multi-year study by Persutte revealed that in 1996, 59% of sonographers were trained on the job. 1 There is not much information publicly available regarding the demographics of sonographers, in the United States. There appears to be greater diversity in the data obtained from the present study compared with Persutte’s data. 1 Sonographers responding to this survey were more likely to be female, 90% compared with 75% of respondents, in Persutte’s study. There were also 93% of respondents that reported to be White compared with 83% in the current study, which represents an increase in diverse respondents, in the current study. The average age and years of experience of sonographers responding to this survey was higher than the Persutte study, which reported an average age in 1991 as 37 years, and 43 years in 1996. 1 In the current study the majority of responses came from the 55 to 64 age group, and they had 23 years of sonography experience, on average. This is in comparison to the Persutte’s participants that had on average 10.6 years of experience in 1991 and 15 years of experience in the 1996 study. 1 Another difference in the respondent cohort, in the Persutte’s study, was that they were recruited from the membership of the American Institute of Ultrasound in Medicine. The current study cohort was drawn from of the membership of the SDMS.
Education
Effort has been expended repeatedly, over the years, to establish a minimum standard of education for sonographers, and establish requirements for a sonographer’s minimum entry level educational and clinical standards. The ARDMS was established in 1975 and was originally known as the Examination Committee, which began looking at clinical competency. 17 The Joint Review Committee on Education in Diagnostic Medical Sonography (JRC-DMS) was established in 1983. This organization worked in tandem with the Commission on Accreditation of Allied Health Education Programs (CAAHEP). JRC-DMS reviews programs curricula and makes recommendations to CAAHEP; it accredits many sonography programs in the United States. This organization has provided standards and guidelines for a proper sonography curriculum. 18 Due to these organizational efforts, the profession now has an accepted pathway for sonography education, and the need for “on the job” training is no longer recognized as sufficient. 10
A bachelor’s degree is still the most common terminal educational degree for a sonographer to earn, and nearly all sonographers recognized the value of obtaining sonography credentials. Most of the current survey respondents (89%) felt that sonography programs should grant a college degree. This provides greater credence and recognition of the amount of education and expanse of knowledge required to become a sonographer. In order to recruit and retain trained sonographers, clinical departments should communicate with administration and human resources departments about the skills, education, and credentialing needed for new clinical hires. Job descriptions should be created and shared with every newly hired employee. The American Medical Association defines a technician as someone with only minimal education and this can be as little as 6 weeks to 6 months of postsecondary education. 19 This is considered to not be a sufficient amount of time required to train and educate a sonography student and achieve clinical competency. The term sonographer should be used instead of ultrasound technician for anyone trained in sonography and becomes credentialed. Those with certification in vascular technology frequently use the title vascular technologist as they may perform sonographic imaging studies as well as non-imaging techniques, to assess for vascular disease. Human resource departments in hospitals, and other facilities that employ sonographers should be provided with these occupational distinctions. Health care unions that represent sonographers should become educated about these occupational details, in order to best advocate for appropriate pay scales, for their members. A sonographer’s salary and responsibilities should be commensurate with their training, credentials, and years of clinical experience.
Accreditation of Clinical Laboratories
Although there is no federal law mandating licensure and only four states currently require licensure, the employment need for credentialed sonographers is significant. Clinical sonography laboratories that are accredited by various professional organizations usually require certified sonographers (see Table 5). There is also need for laboratory accreditation, due to federal reimbursements for the billing of cardiovascular sonography examinations. 20 Clinical laboratory accreditation is one more measure that can demonstrates a standard of quality care, the imaging skills of sonographers, and diagnostic standards. Sonographic examinations that are performed in accredited clinical laboratories are generally of better quality, due to a dedication to superior patient care and the less likelihood of repeat clinical examinations, being ordered. 3
The Sonography Credentialing Requirements That are Required by Varied Professional Accreditation Organizations.
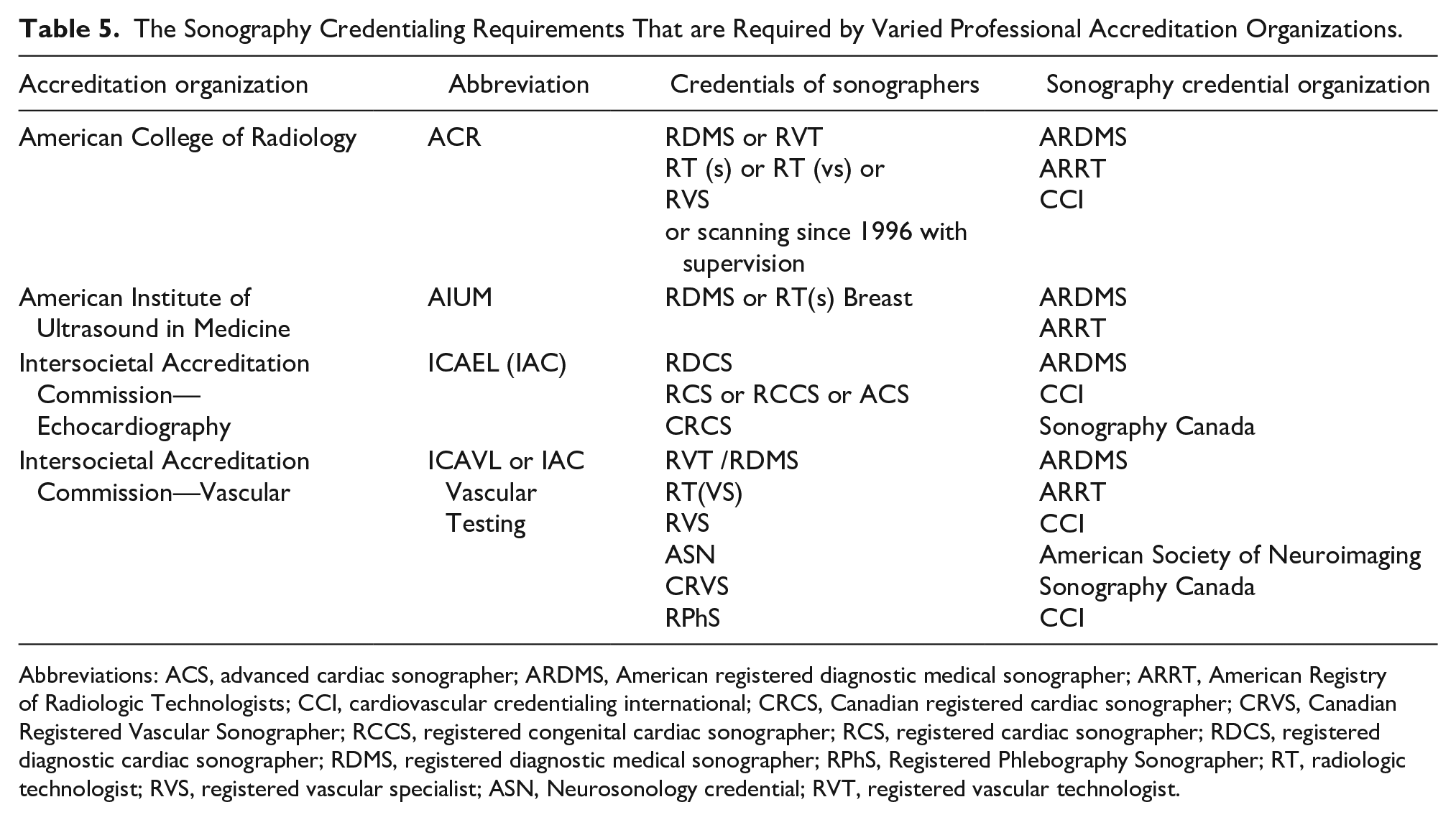
Abbreviations: ACS, advanced cardiac sonographer; ARDMS, American registered diagnostic medical sonographer; ARRT, American Registry of Radiologic Technologists; CCI, cardiovascular credentialing international; CRCS, Canadian registered cardiac sonographer; CRVS, Canadian Registered Vascular Sonographer; RCCS, registered congenital cardiac sonographer; RCS, registered cardiac sonographer; RDCS, registered diagnostic cardiac sonographer; RDMS, registered diagnostic medical sonographer; RPhS, Registered Phlebography Sonographer; RT, radiologic technologist; RVS, registered vascular specialist; ASN, Neurosonology credential; RVT, registered vascular technologist.
Scope of Practice
The field of sonography is constantly evolving with an increased need for educated and well-trained sonographers. In addition to an aging population that requires a higher volume of imaging, many medical specialties are using sonography, as a primary diagnostic imaging technique. It is important for sonographers to educate health care providers and administrators as to the value and level of knowledge that sonographers bring to the care of patients. Being a proficient sonographer requires cognitive, affective, and psychomotor skills, as well as a high level of critical thinking. Those in the workforce should also promote using the term “sonographer” as opposed to ultrasound technician for those who have credentials.
The developing need for the sonographer to handle a patient’s IV insertion, appears to be growing and may be subject to a change in skills. While the new 2020 CAAHEP Standards and Guidelines, for sonography programs, have expanded the sonography educational requirements, which includes knowledge and skill in IV insertion, this has to be balanced with the expectations of sonographers, rules, and regulations regarding IV insertion, which may vary by state.
The autonomy of the sonographer regarding creating preliminary reports and revealing preliminary impressions can and should be reviewed more closely. While interpreting physicians provide a final diagnostic report, the sonographer plays a significant occupational role in the diagnostic process. In the current study, 99% of sonographers reported that they provide a preliminary report, based on their sonographic findings. The professional relationship and level of trust between the sonographer and interpreting physician is an important component in any clinical department that provides sonography services. With some facilities using teleradiology services, or remote supervision in rural areas, this level of reliance on the sonographers’ work has become even more important and relevant. Skilled sonographers are able to provide accurate and reliable technical reports, as they are knowledgeable, proficient in sonographic technique, and appropriately trained to not only acquire diagnostic images, but to interpret them, and provide preliminary recommendation. Based on the current survey results, most sonographers are providing this set of services on a daily basis. This is an area that perhaps should be explored further and recognized, as some of these preliminary findings are being entered in patient charts and PACS systems.
As the diagnostic value of sonography has been promoted as a beneficial diagnostic imaging tool, many others in health care are interested in learning how to complete a sonogram and many sonographers are involved in teaching others (students and health care professionals) these skills. The scope of practice document identifies the concept of sharing knowledge and expertise with others under standard 3.3: Collaboration. It does stop short of describing the opportunity for sonographers to train other professionals. This is another responsibility or activity a sonographer may engage in, especially if they work in an academic medical center.
The SDMS scope of practice document addresses the ability of the sonographer to extend the protocol as needed; however, based on the current study responses, sonographers should have even greater autonomy in terms of preliminary reporting, sharing timely urgent findings, revealing fetal gender, and the level of involvement in contrast studies.
Limitations
The significant limitation to this study was the research design and the convenient sample of participants. No comprehensive master list exists of all sonographers, in the United States. Because there is no required license to practice sonography, there is also no national database of sonographers, in the United States. Therefore, it is difficult to determine the population of sonographers that are currently practicing in the United States. As such, sampling was likely limited, and random sampling was not performed. This survey was distributed to SDMS members that met the study’s inclusion criteria. The SDMS limited the number of reminders that could be sent to its members and the survey was accessible for only 1 month. Considering potential threats to external validity: although there was a low response rate, the sample included sonographers from across the United States with the exception of three states and the District of Columbia. Participants included sonographers with a wide range of clinical specialties, credentials, years of experience, and type of workplace. A greater response rate would have boosted the strength of the findings. There may be a higher number of sonographers than reported in this study that are unaware of the SDMS scope of practice document or may practice additional duties. The sonographers that participated in this study however provided tangible data. A follow-up study could be done that would include sonographers who are not members of SDMS and are currently practicing with at least 5 years of experience.
Conclusion
The majority of the sonographer responding to this survey were women. In this study, the respondents’ data would suggest that there are gender differences in job titles as well as most likely their place of employment. In this study, male sonographers worked primarily in academic medical centers or large urban hospitals. This is in comparison to women reportedly worked primarily in private physician’s offices and outpatient facilities. The data provided suggested that there were some regional differences in sonographer responsibilities, specifically with regard to revealing gender of the fetus, and IV insertion. Most responding sonographers described their job responsibilities as those delineated within the SDMS Scope of Practice document. These respondents indicated that sonographers were providing preliminary diagnostic impressions so this likely needs to be further explored and perhaps recognized.
Program directors of sonography educational programs should acquaint their students with the resources that SDMS provides for sonographers, such as job descriptions and the Scope of Practice and Clinical Guidelines. They should encourage their sonography graduates to request a job description upon hire. The data provided from this study points to a need for the SDMS Scope of Practice document be expanded to include the ability of the sonographer to train other health care professionals in sonography, as most of the respondents reported training other health care providers and students in the sonographic skills. Perhaps if this was to be formally recognized in the scope of practice, it could lead to an official expansion of professional training responsibilities for experienced sonographers.
Footnotes
Acknowledgements
The author acknowledges Milana Yakubova, BS, RDCS, RVT; Alina Menshikov, BS, RDMS, RDCS; Rachel Krischer, BS; and Kayla Warner-Rawlins, BS, RDMS, RDCS for their assistance with data collection, and thank Drs Rena Orman and Mark Stewart for their ongoing support for this endeavor.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
This study was reviewed by the State University of New York Downstate Health Sciences University Institutional Review Board and deemed exempt.
Informed Consent
Informed consent was not sought for this study because all case data were de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study.
Trial Registration
Not applicable.