
Abstract
Celiac artery stenosis may occur in patients with a known history of atherosclerosis and should also be considered in those who present with abdominal pain. Sonography is specific and necessary when the information is correlated with a computed tomogram (CT), as it helps to determine patency and velocity within mesenteric vessels. When stenosis is severe, chronic mesenteric ischemia results, as vascular perfusion is diminished to the intestinal organs. In the case presented with severe atherosclerosis, both CT and sonography were helpful in confirming the diagnosis. Sonography can help in evaluating celiac artery stenosis, caused by atherosclerosis versus median arcuate ligament syndrome, by considering the normal velocities of the vessel.
Celiac artery (CA) stenosis has a low prevalence of 5% to 10% and presents with a range of etiology including congenital anomalies, atherosclerosis, pancreatitis, and trauma. 1 Although it is a condition of low prevalence, a patient may present as asymptomatic and incidentally be found to have CA stenosis. If a patient is asymptomatic, treatment is not advised as surgery should be dedicated to symptomatic patients. A prospective study of 400 patients demonstrated the exact etiology of their condition as extrinsic, in 55% of this cohort. 2 The remaining intrinsic patient cases, in that cohort, were caused by atherosclerosis. 2 This study was performed in Korea; therefore, it is important to consider the prevalence of atherosclerosis may be higher in the United States. Atherosclerosis is the underlying cause of 50% of deaths in Western society, which underscores the need for sonographers to carefully evaluate for hemodynamically significant vessel stenosis in this population. 3 It is of clinical importance to identify if the cause for CA stenosis is intrinsic or extrinsic, as the management of this disease can change depending on the exact etiology. 4
Case Report
A 70-year-old woman presented with abdominal pain, elevated liver function tests, and known peripheral vascular disease. The patient previously had inferior mesenteric artery (IMA) occlusion and a superior mesenteric artery (SMA) stent placed. A previous abdominal sonogram, 1-week prior, showed tumefactive sludge, within the gallbladder, cholelithiasis, and no evidence of acute cholecystitis. The patient reported continued abdominal pain after eating, which prompted a concern for possible ischemic bowel disease. The history of peripheral vascular disease and abdominal pain indicated the need for a follow-up sonogram that focused exclusively on the mesenteric vasculature.
The sonogram was performed using a General Electric (GE) LOGIQ E9 ultrasound system (GE Healthcare, Chicago, Illinois) and a low-frequency curvilinear (1–6 MHz) transducer. The patient was placed in the supine position for the examination. The CA and its branches, the hepatic and splenic arteries, were evaluated with gray scale, color, and spectral Doppler. All the vessels investigated were shown to be patent. The celiac, splenic, and hepatic arteries had peak systolic velocities (PSVs) of 638 cm/s (see Figure 1), 735 cm/s, and 320 cm/s, respectively.
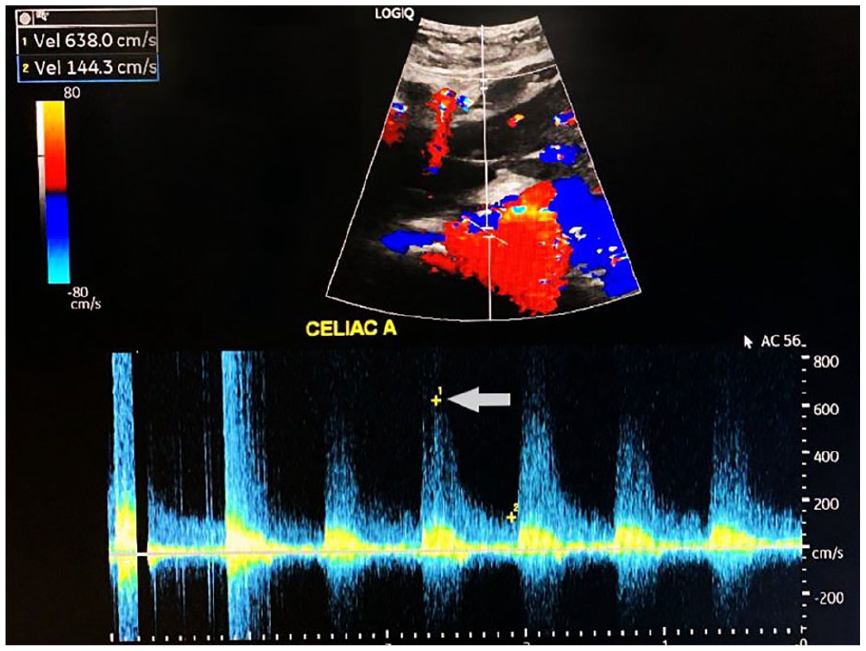
This image demonstrates the velocity of a celiac artery, using spectral Doppler. The velocity is considerably elevated, in this vessel, at 638 cm/s.
These were high peak velocities that were indicative of arterial stenosis. The SMA stent was patent with an elevated PSV of 603 cm/s, at its origin from the aorta (see Figure 2). The CA showed a mosaic flow on color Doppler, indicative of aliasing and a potential stenosis located just proximal to this area (see Figure 3). The IMA was not visualized with this sonographic examination, which may have represented chronic occlusion and was confirmed on computed tomogram (CT). The sonogram for this patient was ordered prior to the CT to evaluate the cause for postprandial pain. The CT confirmed the findings by revealing a patent SMA, an occluded IMA, and severe atherosclerosis, throughout the aorta and vascular branches. The CT for this patient revealed a severely stenosed CA with a hook-like deformity (see Figure 4).
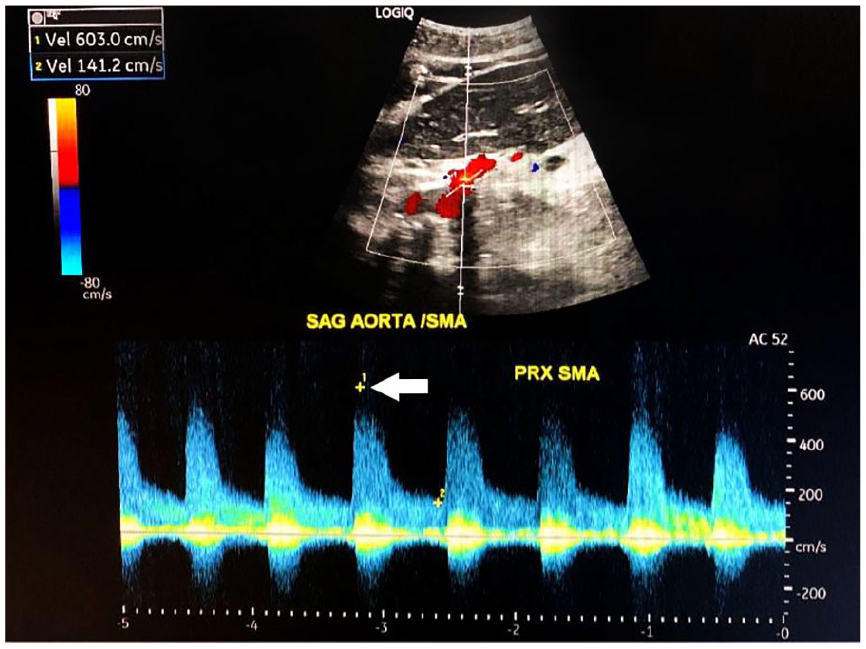
This image demonstrates the velocity of a superior mesenteric artery (SMA), at its origin from the aorta, using spectral Doppler. The peak systolic velocity (PSV) is elevated to 603 cm/s.
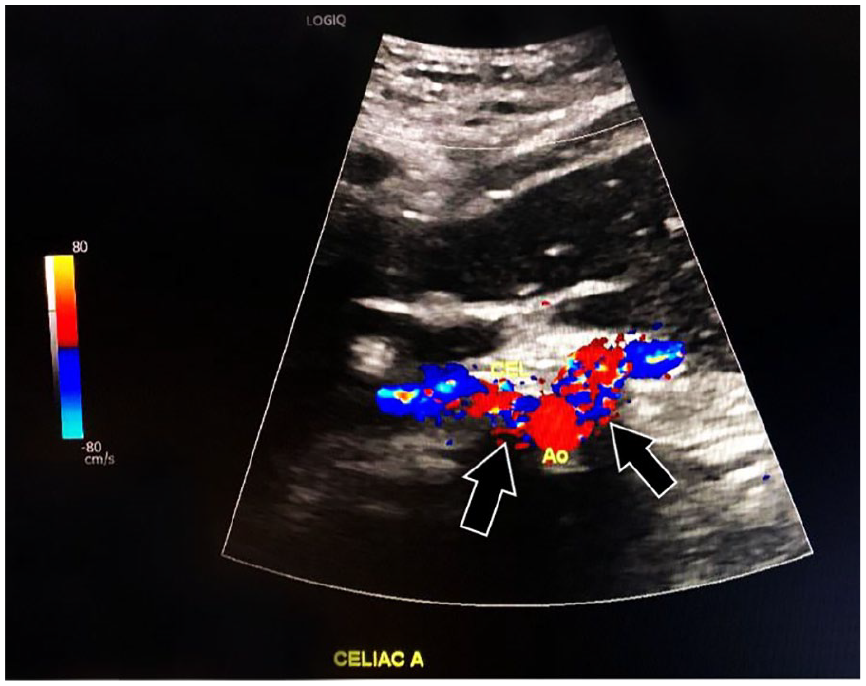
This image demonstrates a mosaic artifact that is seen from the high-velocity flow, within the celiac artery and the associated vessel branches.

This computed tomographic image shows a severely stenosed celiac artery with associated atherosclerotic disease noted, within the abdominal aorta.
The combination of sonography and CT assisted the radiologist in reaching the final diagnosis. The heavy calcifications within the celiac trunk and SMA limited full visualization on CT, particularly with respect to the SMA stent. It was reported that the SMA stent had narrowing within the mid portions of the stent. While this was not fully visualized on the sonogram, due to the calcifications, the elevated velocities indicated narrowing and patency. The narrowing and calcified SMA in this patient likely did not allow for adequate perfusion to the bowel and lead to continued abdominal pain.
Discussion
The celiac trunk is a visceral artery that supplies blood to the abdominal organs, including the liver, gallbladder, pancreas, spleen, duodenum, and jejunum. Poor perfusion of blood flow to the intestinal organs can result in clinical symptoms of postprandial pain and weight loss.5,6 This particular patient did not have treatment due to the surgical risks outweighing the benefits, given the patient’s condition. The prognosis was not considered to be life-threatening, especially given that the SMA was acting as a collateral vessel. However, the symptoms of abdominal pain were likely to continue.6,7
Celiac artery stenosis may arise from an intrinsic factor, such as atherosclerosis, or a congenital anomaly. The most common anomaly concerns the median arcuate ligament (MAL). The MAL is a fibrous arch formed by the crura of the diaphragm. It passes posteriorly to the celiac axis origin, leaving potential for the ligament to extrinsically compress the CA in cases of a high CA origin or an inferior extension of the ligament. 3 In patient cases questioning CA stenosis, the sonographer must attempt to determine whether an extrinsic compression of the CA is due to median arcuate ligament syndrome (MALS). This can be accomplished using spectral Doppler, of the CA, during episodes of both inspiration and expiration.6,8
Celiac artery stenosis is a known cause of ischemic bowel disease; however, it often goes unreported due to the collateral circulation provided by the SMA. 8 The recommended treatment for stenosis is surgery, when clinically indicated, to provide stenting of the artery. 7
Using sonography and CT, as valuable diagnostic tools, to diagnose CA stenosis, it is important to determine the deviation from the normal velocities of the visceral arteries. A PSV of greater than 200 cm/s in the CA and a PSV of greater than 275 cm/s in the SMA are indicative of a greater than 70% arterial stenosis. The normal PSV of the celiac trunk is 98 to 105 cm/s, whereas the normal PSV of the SMA is 97 to 142 cm/s. 5
Patients for this type of examination should not take anything by mouth for 6 to 8 hours prior to the examination. The CA should be examined using color and spectral Doppler during normal respiration, taking note to measure the velocities during inspiration and exhalation to exclude the possibility of MALS.6,9 Sonography is useful as a dynamic imaging tool that can help to differentiate between intrinsic and extrinsic factors. While CT angiography is considered the gold standard for diagnosis, duplex sonography demonstrated a 87% sensitivity, 86% overall accuracy, and 83% specificity when interrogating a PSV of greater than 240 cm/s, in a 50% vascular stenosis. 10
Conclusion
The utilization of sonography, in conjunction with CT, provides the radiologist with critical information when CA stenosis complicated by atherosclerosis results, in imaging limitations. This case study illustrates that when a patient is experiencing significant abdominal pain and has a history of atherosclerosis, a mesenteric Doppler study may be warranted. The sonographer must be familiar with the normal and abnormal velocities of the celiac trunk and SMA, as well as the hemodynamic changes within these vessels. It is prudent for the sonographer to confirm that the cause of this type of stenosis is intrinsic or extrinsic. 4 Sonography is especially useful in determining the patency of a vessel which can be difficult to fully identify on a CT examination.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was granted by the HCA-HealthONE IRB.
Informed Consent
Informed consent was not sought for the present study because all case data were de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).