
Abstract
Celiac artery compression syndrome, also known as median arcuate ligament syndrome and Dunbar syndrome, is a rare cause of chronic mesenteric ischemia. Ischemia results from external compression of the proximal celiac artery during respiration, typically during expiration, by the median arcuate ligament just below the diaphragm. The author reviews the current literature to highlight the most common signs and symptoms, the imaging features, and the treatment options associated with celiac artery compression syndrome.
Keywords
Introduction
The existence of a distinct clinical syndrome associated with celiac artery compression was first questioned nearly 40 years ago.1,2 Today, celiac artery compression syndrome (CACS), also known as median arcuate ligament syndrome and Dunbar syndrome, remains controversial, and its pathomechanism is still not well defined.3,4 Although some authors have considered differential diagnoses such as neoplasms of the pancreatic head, adjacent duodenal carcinoma, vascular aneurysms, aortic dissection, and sarcoidosis, 5 it has been widely accepted that CACS is a rare cause of chronic mesenteric ischemia resulting from external compression of the proximal celiac artery, typically during expiration, by the median arcuate ligament of the diaphragm. 6
Anatomy
The diaphragmatic crura arise from the anterior surface of the L1 to L4 vertebral bodies on the right and the first two or three lumbar vertebral bodies on the left. In addition, the crura arise from the intervertebral disks and anterior longitudinal ligament. The crura pass superior and anterior to surround the aortic opening and to join the central tendon of the diaphragm. The median arcuate ligament is a fibrous arch that unites the diaphragmatic crura on either side of the aortic hiatus. As seen in Figure 1, the ligament usually passes over the aorta at the level of the first lumbar vertebral body, superior to the origin of the celiac axis (Figure 1); however, in 10% to 24% of the population, the ligament may be lower and therefore cross over the proximal portion of the celiac axis, causing a characteristic indentation (Figure 2). 7 Because of topographic relationships of the participating structures, a spectrum exists from slight compression, which is usually asymptomatic, to complete constriction of the celiac artery. 8 In patients with CACS, the celiac artery is compressed by the median arcuate ligament with expiration. With inspiration, the celiac artery descends in the abdominal cavity, resulting in a more vertical orientation of the celiac artery, which often relieves the compression. With the patient in the upright position, the celiac artery descends farther into the abdominal cavity, which increases the vertical orientation of the celiac artery even more and further relieves compression caused by the median arcuate ligament. 9 Because symptomatic patients, most often female with a mean age of 45 years, 10 tend to present with a variety of symptoms, both diagnosis and the development of a treatment plan are challenging 3 ; therefore, the most common signs and symptoms, the sonographic technique, the imaging features, and the treatments options and outcomes associated with CACS are the focus of this literature review.

Schematic drawing from the sagittal perspective showing the typical anatomy of the median arcuate ligament as it crosses anterior to the aorta and superior to the origin of the celiac axis. Reprinted with permission from Horton et al. 7

Schematic drawing from the sagittal perspective showing a normal-variant anatomy in which the median arcuate ligament crosses the proximal portion of the celiac axis, causing an indentation that is most prominent during expiration. Reprinted with permission from Horton et al. 7
Signs and Symptoms
Clinically, an abdominal bruit that is detected during expiration and disappears during inspiration increases the probability of the clinical diagnosis. 10 Additional signs and symptoms linked to CACS include postprandial abdominal pain, epigastric pain related to respiratory variations, nausea and vomiting, diarrhea, and weight loss. Exercise-induced abdominal pain that occurs in otherwise healthy young athletes has also been reported. 11
Certain positions, such as leaning forward, may mitigate or alleviate abdominal pain. Some patients have chronic, continuous epigastric pain that sometimes radiates to the left flank or into the back. Celiac artery compression may also cause poststenotic dilatation or frank distal celiac aneurysm formation. The development of pancreaticoduodenal artery aneurysms has also been attributed to celiac artery compression; increased collateral circulation from the superior mesenteric artery (SMA) has been implicated as an etiology. Rarely, the stenotic process can involve the renal arteries, causing renovascular hypertension. 3
Diagnostic Evaluation
Diagnostic tests should include mesenteric duplex scanning to assess proximal aortic inflow, the celiac artery, the SMA, and the inferior mesenteric artery (IMA). Patients suspected of having renovascular hypertension or ischemic nephropathy should undergo renal artery duplex scanning. Computed tomographic angiography and magnetic resonance angiography are excellent noninvasive imaging studies, although sometimes biplane contrast aortography, performed during inspiration and expiration, will be necessary to give the proper diagnosis.3,12
Sonographic Technique
Because the symptoms associated with CACS mimic the symptoms associated with mesenteric ischemia due to stenosis or occlusion of the SMA and/or IMA, a sonographic evaluation of the entire mesenteric system is recommended. To optimize the examination, the patient should fast for a minimum of 8 hours before the sonographic study. Studies should be optimized for abdominal vascular imaging with lower frequency (3–5 MHz) transducers. Color optimization should include adjustment of the color gain, color wall filter, and color scale (pulse repetition frequency). Harmonic imaging is recommended to minimize artifacts. Small sample volumes (2–5 mm) should be used to obtain Doppler spectral information from the vessels of interest. All velocity measurements should be obtained with angle correction of 60° or less. 8
With the patient in the supine position, the protocol for the mesenteric evaluation should include examination of the abdominal aorta from the celiac axis to the level of the IMA. The abdominal aorta should be visualized in the sagittal and transverse planes. In the sagittal plane, the celiac artery and SMA can be identified arising from the anterior aspect of the aorta, and the IMA can be identified arising from the left anterolateral aspect of the aorta, below the origin of the renal arteries and just proximal to the aortic bifurcation. Grayscale imaging should be used to evaluate for atherosclerotic plaque or aneurysms in the aorta and proximal branch vessels. Color Doppler imaging should be optimized to assess for patency and blood flow abnormalities, including aliasing, bruit artifacts, and poststenotic turbulence. Spectral Doppler sampling should be performed in the aorta at the level of the mesenteric arteries and at the origin and proximal segments of the celiac artery, SMA, and IMA. 8 According to the Intersocietal Accreditation Commission Vascular Testing, spectral Doppler sampling at the origins of the common hepatic and splenic arteries should also be included, as well as middle and distal segments of the SMA. Additional velocities should be documented both proximal and distal to all areas of stenosis.
When CACS is suspected, it is imperative that velocity measurements of the celiac artery be obtained during both inspiration and expiration to determine whether abnormal velocities are the result of a fixed intraluminal stenosis of the vessel or extrinsic compression of the celiac artery by the median arcuate ligament of the diaphragm. In addition, further evaluation of the celiac artery with the patient upright is also recommended. With the patient in the upright position, the celiac artery descends farther into the abdominal cavity, resulting in a more vertical orientation of the celiac artery, relief of compression by the median arcuate ligament, and improved (i.e., nonstenotic) blood flow. Without upright views, erroneous diagnosis of celiac artery stenosis may be concluded instead of CACS. 9
Imaging Features
Figure 3 demonstrates a normal celiac artery during inspiration and expiration in a patient with no sonographic evidence of CACS. Figure 4, on the other hand, clearly demonstrates the compression of the proximal aspect of the celiac artery by the median arcuate ligament, producing a “kink” and a significant stenosis during expiration. The use of color Doppler imaging, shown in Figure 5, further highlights the stenosis observed during expiration in a patient with suspected CACS. 13 In addition to B-mode and color Doppler imaging, spectral Doppler analysis is also helpful in diagnosing CACS, as celiac artery velocities will increase in areas of stenosis caused by expiration and return to normal levels (<200 cm/s) 14 on inspiration (Figure 6). 6 Finally, abdominal computed tomography angiography is frequently used to confirm sonographic findings of severe stenosis during expiration and normal celiac artery anatomy during inspiration (Figure 7). 10
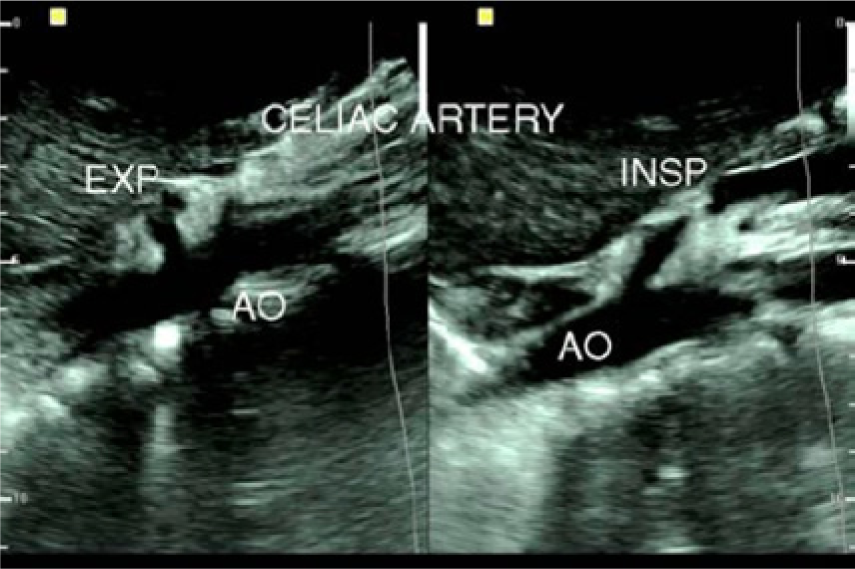
B-mode images of the normal celiac artery during inspiration (INSP) and expiration (EXP), with no stenosis observed. The artery can be seen to ascend with a more vertical orientation off the aorta (AO) during expiration. Reprinted with permission from Youssef. 13
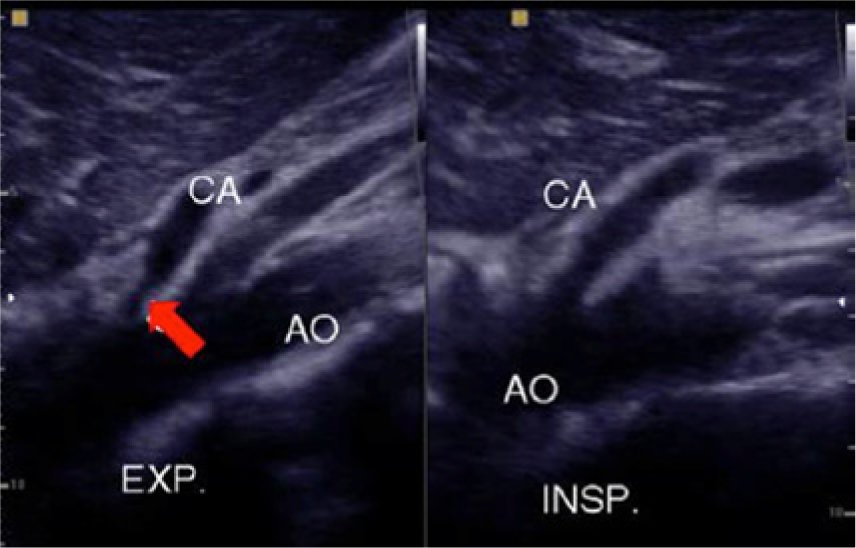
B-mode ultrasound showing expiratory stenosis (red arrow) of the celiac artery (CA). Reprinted with permission from Youssef. 13 AO, aorta; EXP., expiration; INSP., inspiration.
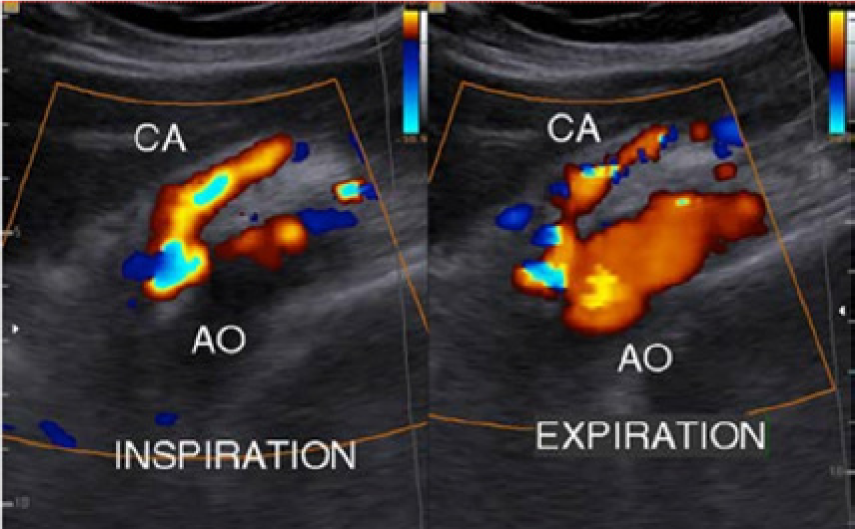
Color Doppler imaging highlights a severe stenosis of the proximal celiac artery (CA) during expiration. Reprinted with permission from Youssef. 13 AO, aorta.
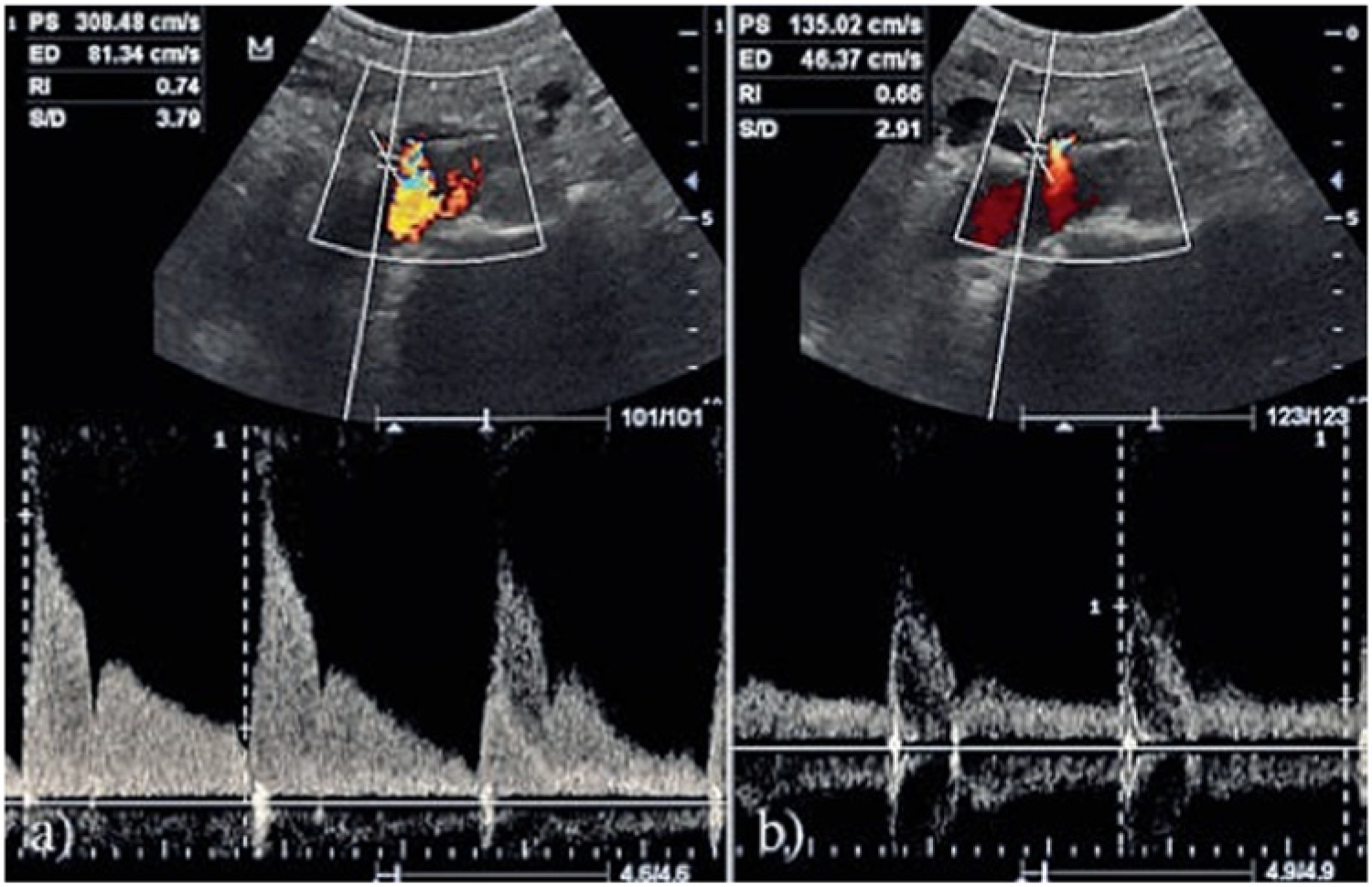
Doppler spectral images of the proximal celiac trunk (A) during expiration, showing elevated peak systolic and end-diastolic velocities (308 and 81 cm/s), and (B) during inspiration, with peak systolic and end-diastolic velocities decreased to normal values (135 and 46 cm/s). Reprinted with permission from Ozel et al. 13
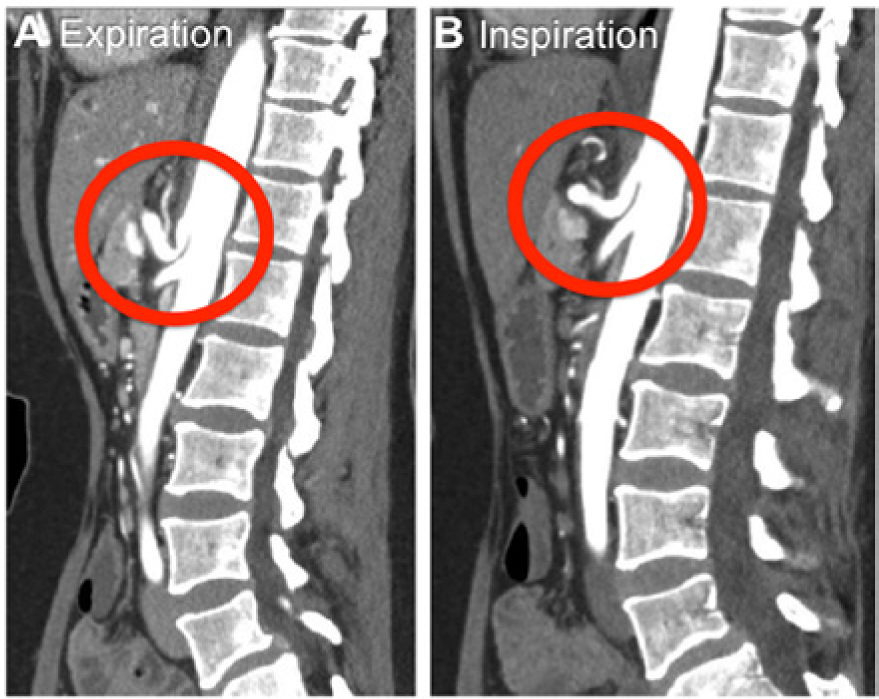
Celiac artery computed tomography angiography (CTA) (A) during expiration and (B) during inspiration. Reprinted with permission from Skeik et al. 10
Treatment Options and Outcomes
There is no consensus on the management of suspected CACS. Percutaneous approaches and stenting of the celiac artery may be difficult because it is tethered to and restricted by fibers of the diaphragm, which is in constant motion. These approaches also lack the ability to fix any residual stenosis; however, they are less invasive.10,15
Both open surgical treatments and laparoscopic options have been safely performed, with minimal morbidity and mortality.3,16,17 Delayed recurrence of celiac artery compression with symptoms much less severe than those noted at initial presentation has been seen frequently using both approaches. Open surgical treatment of the extrinsic compression of the celiac artery is accomplished by transection of the median arcuate ligament and the crus of the diaphragm proximal to the celiac artery. The operation is performed through a short upper midline laparotomy and accessing the celiac artery through the lesser sac, transecting the hepatogastric ligament, and retracting the stomach and esophagus to the left. Frequently, there is a well-defined ligament that is firmly attached to the aorta and the celiac artery, and only with difficulty can it be separated from the underlying aorta. In one recent study, if mesenteric ischemia was confirmed in symptomatic patients who had CACS, then open surgical decompression with revascularization, if it was needed, resulted in 100% long-term relief of the symptoms. 3
Laparoscopic techniques to decompress the celiac artery have been reported, including the use of intraoperative laparoscopic ultrasound to confirm normalization of peak systolic velocities distal to the median arcuate ligament. 11 The laparoscopic approach avoids the potential complications of a midline incision associated with laparotomy, and it has been associated with shorter inpatient hospitalizations and decreased need for prolonged parenteral nutrition.10,17
Conclusions
CACS is a rare cause of chronic mesenteric ischemia. The most widely accepted etiology is compression of the proximal celiac trunk by the median arcuate ligament of the diaphragm during expiration. Although definitive diagnosis of CACS is achieved with some form of contrast-based angiography, duplex sonography with spectral Doppler is a useful modality in the diagnostic workup of patients with CACS, as velocity measurements of the celiac artery during both phases of respiration are easily obtained. When celiac artery velocities exceed 200 cm/s, it is crucial that sonographers measure and compare expiration and inspiration velocities, and examine the patient in the upright position, in an effort to determine whether a probable stenosis is actually within the artery or likely the result of extrinsic compression by the median arcuate ligament.
Unlike angiographic techniques, duplex sonography is noninvasive, is less expensive, and does not expose patients to ionizing radiation or iodinated contrast. In addition, through the use of intraoperative laparoscopic sonography, normalization of peak systolic velocities distal to the median arcuate ligament can be confirmed during surgical repair of CACS.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.