
Abstract
Median arcuate ligament syndrome (MALS) is a condition characterized by pain in the abdominal region attributed to compression of the celiac artery by the median arcuate ligament of the diaphragm during expiration. MALS is also known as celiac artery compression syndrome, celiac axis syndrome, or Dunbar syndrome. Pain may result from the tight pressing on the celiac nerves in the area. The patient usually presents with symptoms such as postprandial epigastric pain, weight loss, and, occasionally, an abdominal bruit. Furthermore, some individuals may experience nausea and vomiting. It may be an etiology of a rare disorder, chronic mesenteric ischemia.
The median arcuate ligament is a muscular and fibrous arch under the diaphragm where the right and left crus of the diaphragm connect together. This ligament passes superior to the origin of the celiac artery and continues to the posterior diaphragm, encompasses the aorta, and connects the diaphragm to the spine. Median arcuate ligament syndrome (MALS) is a rare disorder characterized by the compression of the celiac artery by the median arcuate ligament of the diaphragm during expiration. The syndrome was first described by Harjola in 1963 1 and Dunbar et al. in 1965, 2 stating that pain is associated with insertion of the ligament at a lower level of the diaphragm, narrowing the lumen of the celiac trunk by compression. This case reports a patient who was diagnosed with MALS primarily by duplex sonography and computed tomography angiography.
Case Report
A 26-year-old man presented to the hospital with chronic right lower quadrant pain. This patient also complained of postprandial epigastric pain, nausea, vomiting, and weight loss. A computed tomography scan of the abdomen and pelvis with contrast was ordered following an abdominal sonographic examination without spectral Doppler of the mesenteric vessels. The results were negative for suspected acute appendiceal inflammation and gallbladder disease based on the initial clinical symptoms. Further testing was done, including upper and lower gastrointestinal endoscopy and blood tests, yet all the findings were within normal limits.
After five months, the patient returned with the same chronic symptoms but included a new clinical finding of an abdominal bruit that was auscultated, for which a computed tomography angiography (CTA) of the abdomen was ordered. Results suggested a focal high-grade stenosis of the celiac axis origin. However, the radiologist noted that it could also be secondary to extrinsic compression by the median arcuate ligament. An incidental note was made of two left-sided main renal arteries. The patient was referred to the radiology department for another abdominal sonogram, this time including mesenteric Doppler. Real-time color (Figure 1) and spectral Doppler examination of the abdominal aorta and its major branches (celiac trunk and superior mesenteric artery) was interrogated in the supine and erect position after eight hours of fasting.
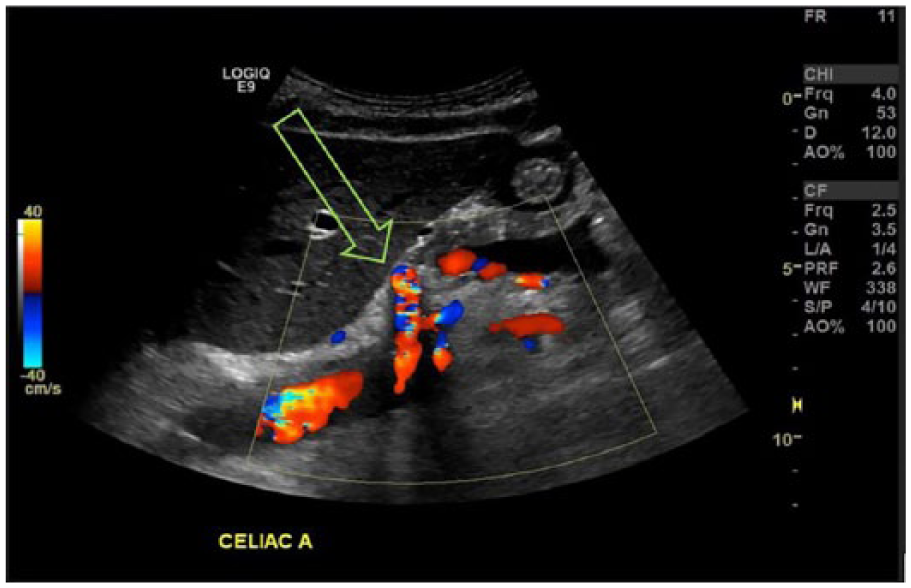
Color Doppler of the celiac artery (arrow) in supine position.
The results indicated stenosis of the celiac artery with turbulent flow. Peak systolic and end-diastolic velocities of the proximal celiac artery (with an angle correction at 49 degrees) were obtained on deep expiration while the patient was in a supine position and measured 331 cm/s and 108 cm/s, respectively (Figure 2). On inspiration, peak systolic and end-diastolic velocities decreased to 200 cm/s and 55 cm/s, respectively (Figure 3).
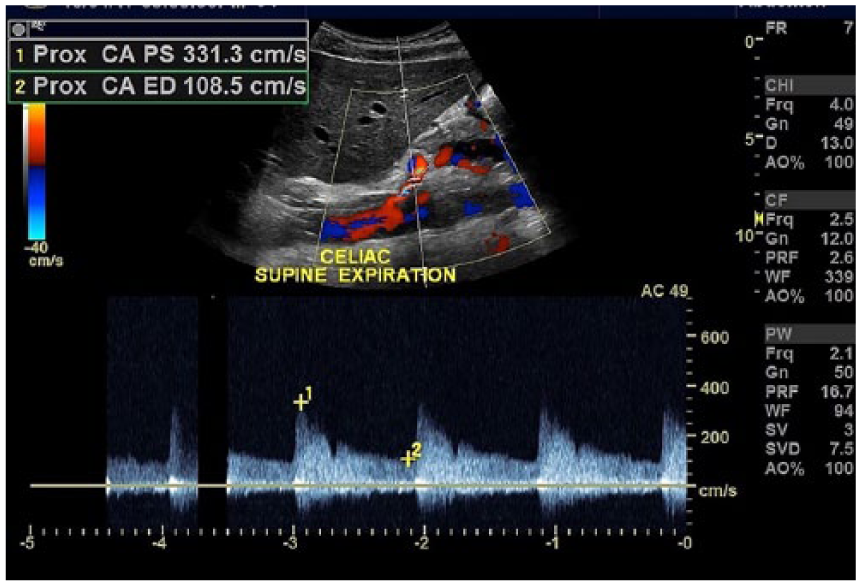
Spectral Doppler image of the proximal celiac trunk during expiration in the supine position. Peak systolic and end-diastolic velocities are elevated (331/109 cm/s).
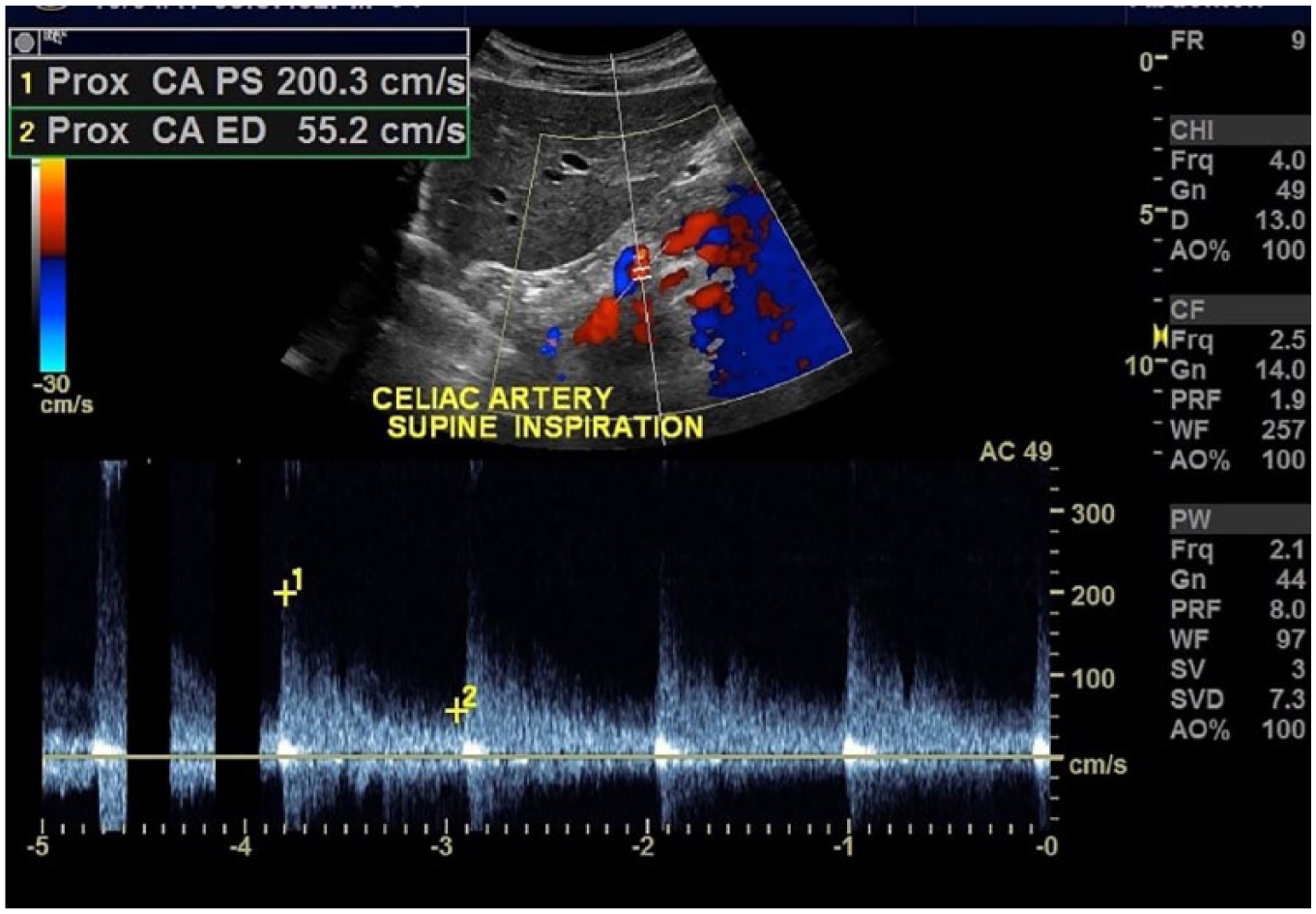
Spectral Doppler image of the celiac artery during inspiration in the supine position. Peak systolic and end-diastolic velocities are decreased (200/55 cm/s).
When the patient was asked to stand up in an erect position, and under normal respiration, the peak systolic and end-diastolic velocities were measured at 143 cm/s and 34 cm/s, respectively (Figure 4). These measurements indicated that the values returned to normal.
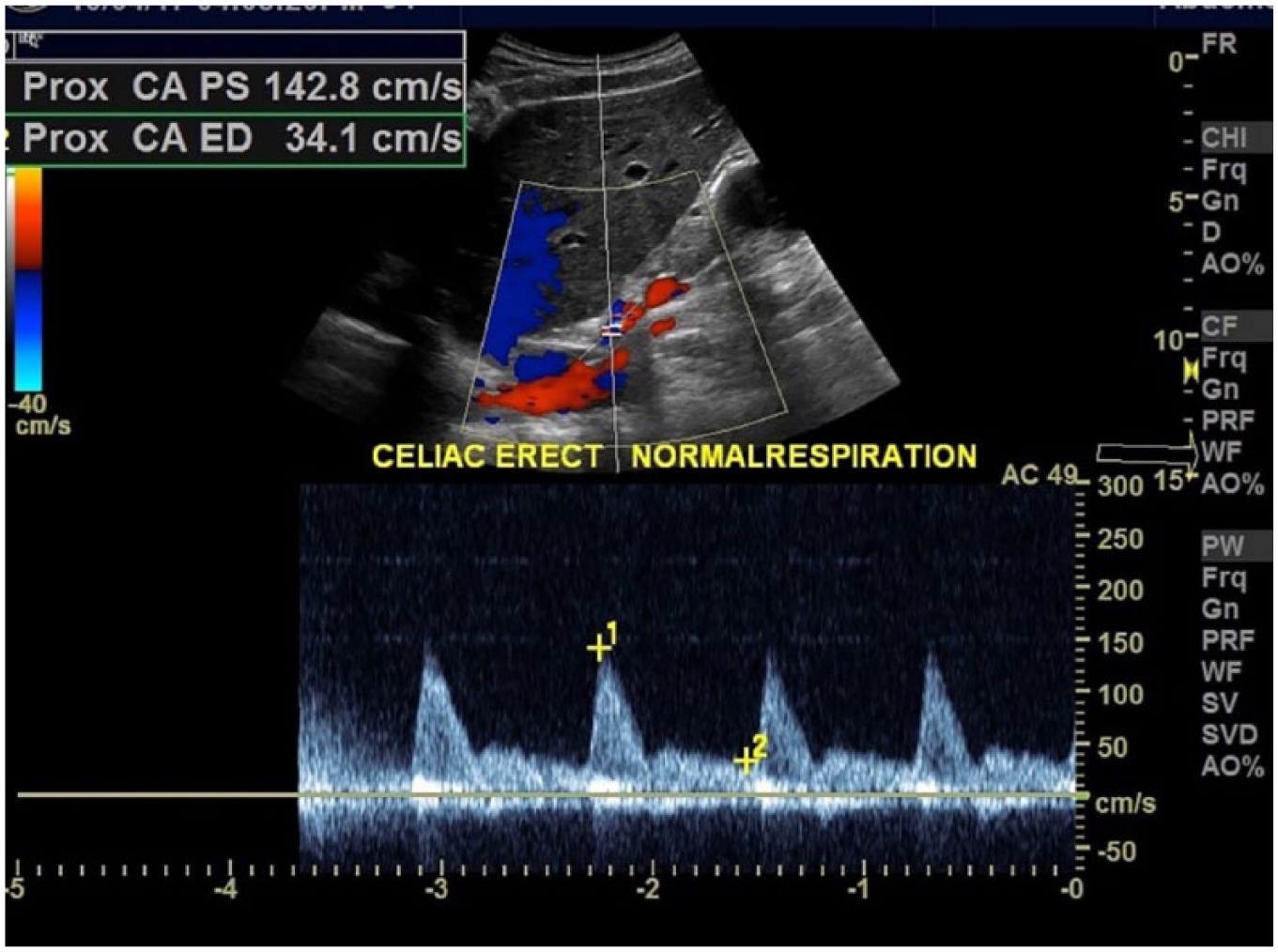
Spectral Doppler image during normal respiration. Peak systolic and end-diastolic velocities within the celiac artery return to normal values with the patient in an erect position (143/34 cm/s).
In this case study, the patient had to undergo extensive evaluation of his gastrointestinal tract (upper and lower), evaluation for gallbladder disease, and even evaluation for gastroesophageal disease before MALS was considered as a diagnosis. Duplex sonography was a useful noninvasive test that helped achieve the diagnosis for MALS in correlation with this patient’s CTA.
Discussion
MALS is a condition that is seldomly considered a differential diagnosis for abdominal pain outside of a cardiovascular physician’s empirical knowledge base. Patients present with postprandial epigastric pain, nausea and vomiting, and subsequently weight loss (typically over 20 pounds). 3 Other symptoms may include diarrhea and delayed gastric emptying, and in some individuals, an abdominal bruit may be heard. It is vital to note the difference between median arcuate ligament syndrome from median arcuate ligament compression. Median arcuate ligament compression occurs in 10% to 25% of the population and does not cause any symptoms. 2 Only about 1% of these individuals who have severe compression experience symptoms. Symptoms typically occur between 20 and 40 years of age and are more prevalent in females than males. The pain from MALS is believed to be caused by the median arcuate ligament compressing on the plexus of nerve fibers surrounding the celiac trunk. In addition, belief is that the compression of the celiac artery can cause ischemia, or decreased blood flow, to abdominal organs, leading to pain. 4 Median arcuate ligament syndrome is distinguished from median arcuate compression by the presence of symptoms. When suspicious for this syndrome, Doppler sonography may be performed to measure the blood flow through the proximal celiac artery during inspiration and expiration. Figure 5 illustrates the anatomical position of the celiac artery with the associated median arcuate ligament in normal anatomy and in MALS.
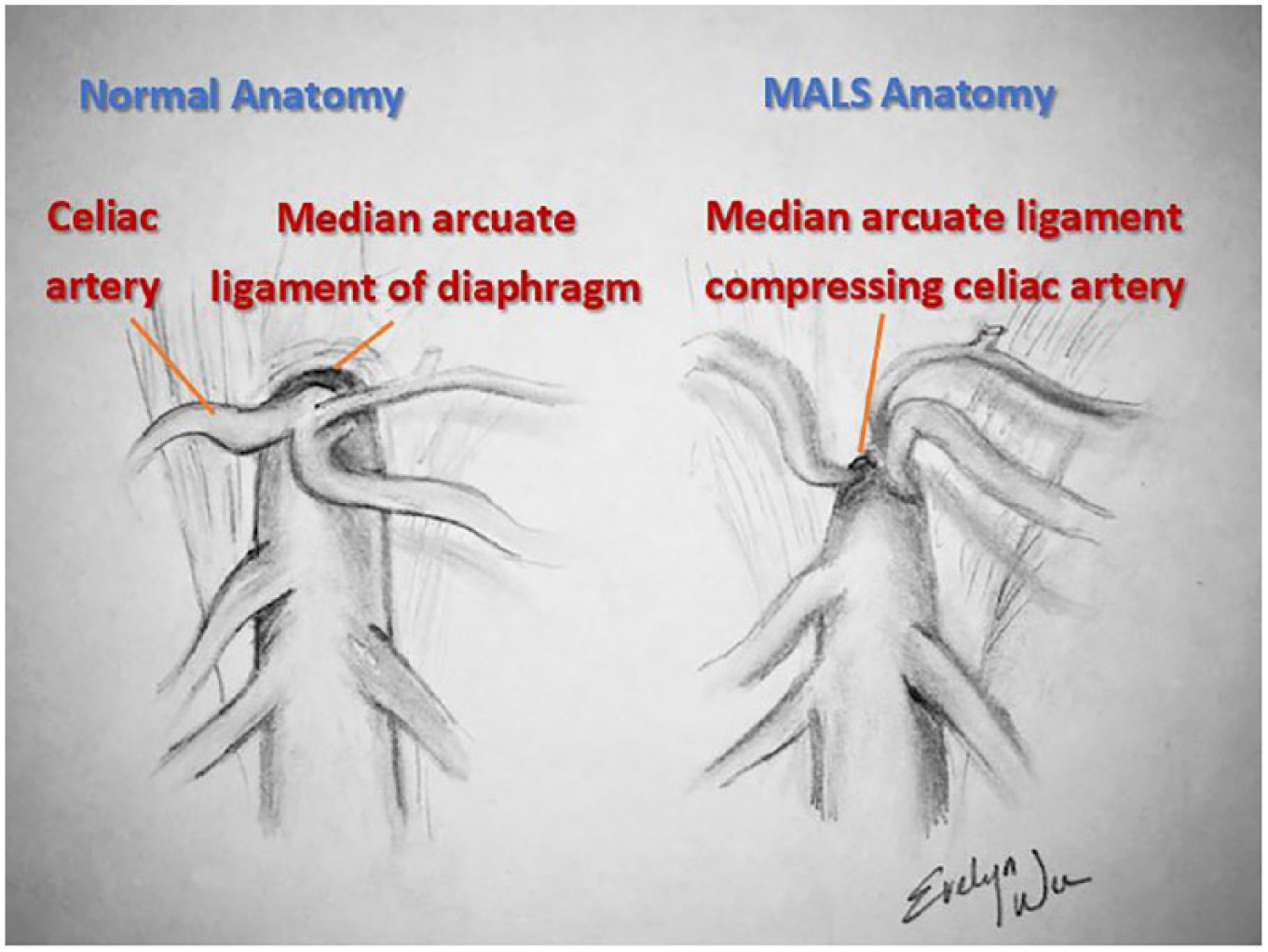
Anatomical illustration of celiac artery and median arcuate ligament. MALS, median arcuate ligament syndrome.
In a normal celiac artery, uniform velocities and waveform configurations (without turbulence) would be present. Peak systolic velocities higher than normal represent stenosis and turbulent flow. The diagnostic criteria for celiac artery stenosis of 70% or greater include a peak systolic velocity (PSV) >200 cm/s and end-diastolic velocity (EDV) >55 cm/s. 5 This was evident in this case study when the patient was placed in the supine position, and in the expiratory phase, the peak systolic velocity measured 331 cm/s. This was greater than the institutional cutoff of 250 cm/s for a 70% stenosis. 5 Upon inspiration, the peak systolic velocity decreased to 200 cm/s. The velocity of the artery decreased because it descended in a vertical orientation away from the median arcuate ligament during the inspiratory phase, thereby relieving some compression. Furthermore, the peak systolic velocity dropped significantly to 143 cm/s (normal reference levels) when the celiac trunk was evaluated while the patient was in an erect position with normal respiration. This was most likely attributed to a more vertical orientation of the celiac axis in this patient position and also because of the less drastic respiration changes.
Traditionally, conventional angiography was used to evaluate the anatomy of the celiac artery. However, it has been replaced by newer, less invasive imaging modalities such as CTA and magnetic resonance (MR) angiography. CTA is the preferred imaging modality over MR angiography because it allows for better visualization of intra-abdominal structures in this setting. 4 The findings of focal narrowing of the proximal celiac artery with poststenotic dilatation, indentation on the superior aspect of the celiac artery, and a hook-shaped contour of the celiac artery support a diagnosis of MALS. 6 The median arcuate ligament is normally several millimeters to centimeters superior to the origin of the celiac artery. In MALS, the ligament lies anterior instead of superior to the celiac artery, causing compression of the vessel and resulting in a hook-shaped contour. During expiration, this condition is exacerbated. The narrowing and hooked appearance is an important characteristic that can help differentiate it from other causes of celiac vessel narrowing, such as atherosclerotic disease. In atherosclerosis, plaque builds up inside the arteries and, over time, hardens and narrows the arteries. Chronic mesenteric ischemia is frequently due to atherosclerosis. 7 Narrowing of the vessel and stenosis may be present, thereby contributing to increased velocity, but no hook-shaped compressed artery will be visualized. Furthermore, if atherosclerosis is involved, the positions used to scan (erect, supine, sitting) and both inspiration and expiration would have a minimal effect on the accelerated velocity. Atherosclerosis disease alters blood velocity without abatement, whereas MALS, as seen in this case study, indicates that maneuvers do demonstrate abatement.
Treatment of MALS is aimed at restoring the normal blood flow of the celiac artery and eliminating the irritation caused by the celiac nerve fibers. Decompression of the celiac artery is the general approach for treatment. The preferred management strategy is by surgically or laparoscopically dividing or separating the median arcuate ligament in combination with destruction or removal of the celiac ganglion. If these interventions are unsuccessful, endovascular methods such as percutaneous transluminal angioplasty may be another alternative for treatment. 8
Conclusion
MALS is a rare disorder and may be an etiology for chronic mesenteric ischemia because of the compression of the proximal celiac trunk by the median arcuate ligament during expiration. Doppler sonography is a useful modality in the diagnostic workup of a patient suspicious for MALS. Doppler measurements of the velocity of the celiac artery during both expiration and inspiration phases, as well as during supine and erect positions, would contribute to the initial diagnosis of MALS. In correlation with CTA and clinical findings, a definitive diagnosis of this syndrome can be achieved.
Unfortunately, the diagnosis of MALS is typically only entertained after more common conditions have been ruled out. In the meantime, the patient may endure months to years of recurrent abdominal pain without knowledge of etiology. For this reason, in patients with upper gastrointestinal disorders, especially postprandial pain that persists after medical therapy, it may be useful to perform vascular investigation sooner with duplex sonography to evaluate the possibility of median arcuate ligament syndrome.
Footnotes
Acknowledgements
Special thanks to Joan Tran (senior sonographer).
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.