
Abstract
Essential thrombocythemia is a myeloproliferative neoplasm characterized by platelet aggregation and thrombosis. Clinically, essential thrombocythemia increases the risk of both thrombosis and bleeding. Essential thrombocythemia is more involved in micro- and small-sized arteries than in large arteries. Many essential thrombocythemia patients exhibit various symptoms, including microvascular thrombosis with acute coronary disease, digital ischemia, and transient ischemic attack. This study reports a rare case of recurrent thrombosis in relatively large vessels including splanchnic, lower extremity arteries, and aorta in essential thrombocythemia. A 70-year-old woman was admitted to the emergency room with abdominal pain and fever for a day. The patient underwent three operations due to recurrent arterial thrombosis of superior mesenteric, splenic, aorta, and lower extremities. She had recurrent diarrhea and acute kidney injury because of short bowel syndrome after extensive bowel resection. In conclusion, essential thrombocythemia patients aged >60 years and who have risk factors such as history of major ischemic events or severe leukocytosis must be careful of thrombosis of the medium- and large-sized arteries, including splanchnic and lower extremity arteries.
Introduction
Essential thrombocythemia (ET) is a myeloproliferative neoplasm characterized with platelet aggregation and thrombosis. Clinically, ET increases the risk of both thrombosis and bleeding. 1 The other features of ET include leukocytosis, splenomegaly, microcirculatory disturbance, pruritus, and leukemic transformation. 2 Sometimes ET is detected later on in patients with thrombosis. The annual incidence of ET was 0.38–1.7 per 100,000, 3 and thrombotic complications occurs in 6.6% of ET patients per year. 4
ET is more involved in micro- and small-sized arteries than in large arteries. 5 Thrombosis in ET patients is usually presented in the cerebral, coronary, and peripheral arteries. 6 Many ET patients exhibit various symptoms, including microvascular thrombosis with acute coronary disease, digital ischemia, and transient ischemic attack. 7
Here, we report a rare case of recurrent thrombosis in relatively large vessels, including splanchnic, lower extremity arteries, and aorta in ET.
Case report
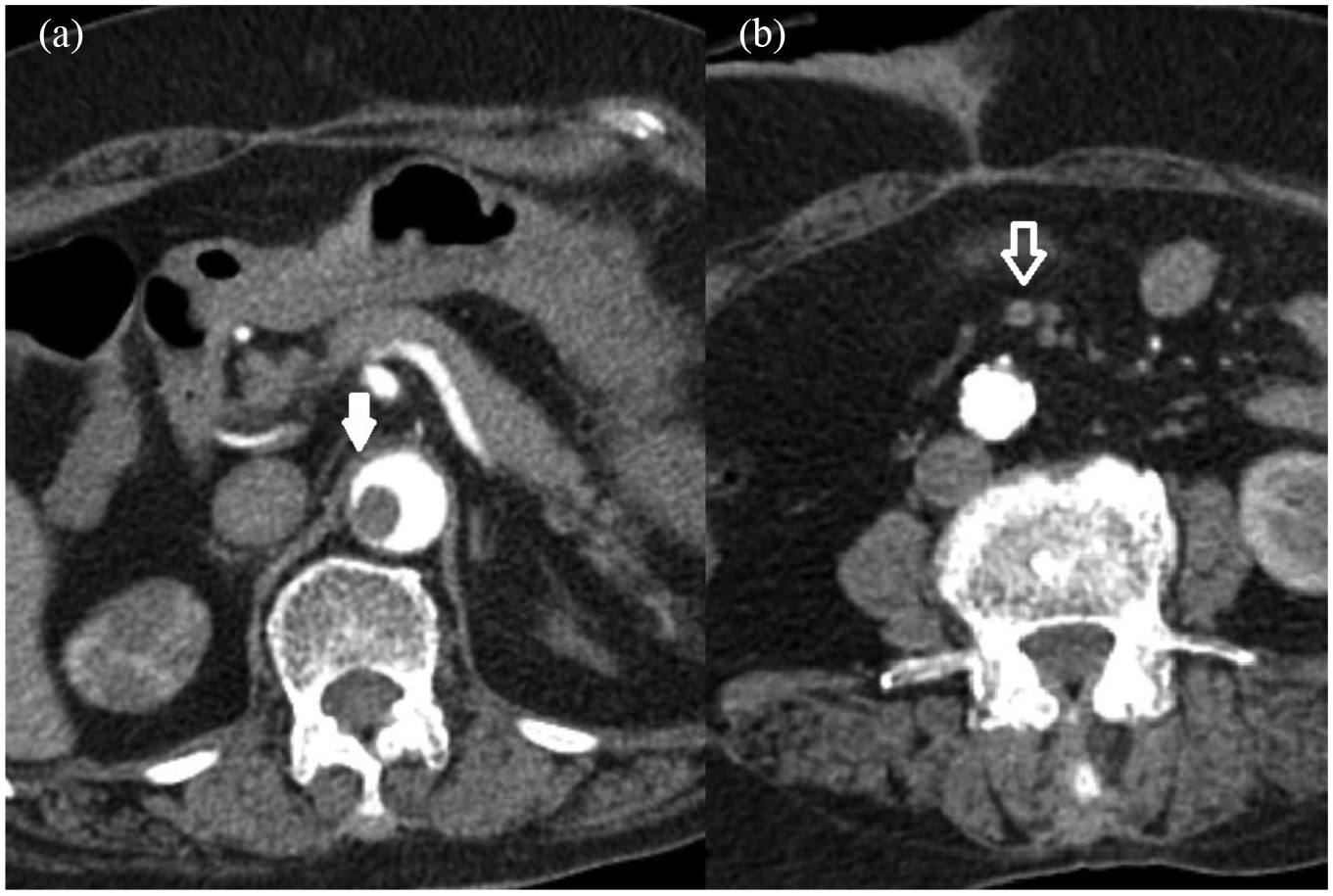
A 70-year-old Korean woman was admitted to the emergency room by ambulance with abdominal pain and fever for a day. She had history of hypertension without any antithrombotic agents. Vital signs were stable. At admission, complete blood count (CBC) revealed a white blood cell count of 49.83 × 103 mm–3, with 75% neutrophils and 3% lymphocytes; platelet volume of 1122 × 103 mm–3, and red cell count of 13.8 mm–3. Other laboratory results showed an elevated creatinine kinase (CK) of 585 U/L, amylase of 117 U/L, and procalcitonin of 6.85 ng/mL. Conversely, laboratory findings, including hepatic, renal function, coagulation, cholesterol, and blood glucose, were within normal limits. The patient had severe abdominal pain with tenderness of the whole abdomen. Abdominopelvic computed tomography (CT) revealed superior mesenteric artery (SMA) thrombosis, jejunal necrosis of long range, and splenic infarction (Figure 1). Emergency operation, consisting of jejunal resection of about 1 m, splenectomy, and double barrel jejunostomy, was performed in the surgical department. Double barrel jejunostomy was performed to check any remnant unhealthy jejunum tissue and to prevent anastomotic leakage.

Enhanced CT scan before the first abdominal surgery: (a) white arrow indicates superior mesenteric artery thrombosis and (b) arrow with white border indicates splenic infarction.
Oral intake was initiated 4 days after surgery, and the patient was stabilized. Bone marrow biopsy showed ET with hypercellular bone marrow and megakaryocytosis. Chromosomal study revealed JAK2 gene mutation at V617F. In postoperative echocardiography, ejection fraction maintained normal without cardiac wall motion defect and arrhythmia. Because of uncontrolled platelet count, the patient took anagrelide and hydroxyurea together with a hematology consultation, postoperatively. Aspirin could not be used due to persistent intraperitoneal bleeding. The patient was discharged without any complications after 2 weeks with hydroxyurea and aspirin.
One month after the first operation, the patient complained of pain in left leg for 2 days. In CT angiography, the femoropopliteal artery was occluded with thrombosis (Figure 2). Emergency thrombectomy with cut-down of femoral and popliteal artery was performed; however, recanalization was unsuccessful due to the failure of catheter passage. Bypass from superficial femoral to below-knee popliteal artery was performed using a reversed saphenous vein graft. After 10 days, the patient was discharged without leg pain and prescribed with anagrelide and warfarin.

Lower extremities CT angiography revealing the artery below superficial femoral artery occluded with thrombosis.
One month after surgery to the lower extremities, the patient visited the emergency room with a new complaint of abdominal pain. Abdominopelvic CT revealed thrombosis of SMA branches, jejunal necrosis, and floating thrombus of the abdominal aorta (Figure 3). Jejunal resection of 1 m and double barrel jejunostomy were performed again. She had recurrent diarrhea and acute kidney injury because of short bowel syndrome after extensive small bowel resection and died 1 year after last operation.
Enhanced CT scan before the second abdominal surgery: (a) white arrow indicates the floating emboli of abdominal aorta and (b) arrow with white border indicates superior mesenteric artery thrombosis.
Discussion
ET is more common in micro- and small-sized arteries than in large arteries. 5 Previous research showed altered regulation of peripheral circulation, including increased resistance and decreased flow. These circulatory disorders were usually confined to the distal arterial bed and the division of the digital arteries. 8 There are some reports of large-vessel thrombosis that required surgery, but such cases are very rare. 5 More cases of ET patients accompanied by aortic thrombosis or splenic infarction are also unusual. 9 However, recent meta-analysis on ET failed to uncover any notable association between JAK2 mutation and microcirculatory disorders. 10 More research is needed in clinical pathophysiology of ET-related vasculopathy.
ET patients show various clinical manifestations, depending on the patients’ risk factors as well as the involved vessels. Carrobio et al. 11 reported that predictors of arterial thrombosis included age >60 years, thrombosis history, cardiovascular risk factors including tobacco use, hypertension, or diabetes mellitus, leukocytosis, and presence of JAK2 V617F. Moreover, Besses et al. 12 also reported that age >60 years and history of major ischemic events may be risk factors of atherothrombotic complications in ET patients. In addition, white blood cell count >104 mm–3 is a risk factor for thrombosis. 13 In this study, recurrent ischemic events and severe leukocytosis were presented in patients aged >60 years. Recurrent occlusions of superior mesenteric, splenic, and femoropopliteal arteries support thrombotic etiologies of ET without cardiac arrhythmia in this study.
Conclusion
Here, we reported a rare case of recurrent thrombosis in relatively large vessels, including splanchnic, lower extremity arteries, and aorta with ET. ET patients aged >60 years and who have risk factors such as history of major ischemic events or severe leukocytosis must be careful of thrombosis of the medium- and large-sized arteries, including splanchnic and lower extremity arteries.
Supplemental Material
Author_Form_IJS_jun – Supplemental material for Recurrent thrombosis of splanchnic and lower extremity arteries with essential thrombocythemia
Supplemental material, Author_Form_IJS_jun for Recurrent thrombosis of splanchnic and lower extremity arteries with essential thrombocythemia by Sung Min Jung and Heungman Jun in SAGE Open Medical Case Reports
Footnotes
Author contributions
S.M.J. contributed in data collection, review of patient history and surgical records, and writing papers. H.J. contributed in the review and control of study concept and design, review of discussion, and writing papers.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The Institutional Review Board (IRB) of the Inje University Ilsan Paik Hospital approved the review of patient records and this study. The number from IRB is 2019-01-027.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
Heungman Jun, MD, PhD (
Informed consent
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article. The patient was already dead and we received written consent from guardian.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.