
Abstract
Acute appendicitis is a condition that can affect any member of the population. Without timely treatment there is a high likelihood of rupture leading to peritonitis, and early diagnosis is imperative to obtaining treatment. Sonography can be used without fear of radiation exposure to the patient and with relatively little discomfort, ideal for pediatric patients. It can also be used with little patient preparation, with the possibility of a more rapid diagnosis than other imaging modalities. For patients presenting with atypical symptoms, sonography may be used to increase diagnostic accuracy, which will lead to a drop in the surgical removal rate of a healthy appendix. When diagnostic criteria are met, sonography results can be correlated with the patient’s blood test and clinical symptoms to make a positive diagnosis. The addition of the transvaginal approach for female patients has further increased the rate of success of diagnosing acute appendicitis, so that appropriate emergent surgery can be done.
Acute appendicitis is an emergent condition that requires immediate care because of the high likelihood of perforation resulting in peritonitis; 1 perforation also carries a doubled risk of patient mortality. 2 Acute appendicitis is the most common emergent condition for adults and children seen for abdominal surgical care.3,4 In a study by the World Gastroenterology Organization, almost a third of cases presenting with acute abdominal pain were diagnosed as appendicitis. 5
Discussion
Abdominal pain in any patient in the clinical setting requires assessment for appendicitis. While patients with typical clinical symptoms do not need further testing for diagnosis and surgical intervention, many patients simply do not present with the symptom complex necessary for reliable diagnosis. 3 Typical presentation of symptoms occurs only about 50% of the time, leaving ample room for nonclassic presentation. 6 Because of its urgent nature, appropriate testing for appendicitis should be fast, easy, and as painless as possible. Negative side effects of testing, such as radiation and contrast injection, are also a concern. Children, just like adults, are frequently seen in the emergency department with abdominal pain, and they require special sensitivity on the part of medical professionals to gather a complete history, elicit all of the symptoms, and determine appropriate testing. Sonography fulfills all these needs without any potentially harmful side effects, and even though they are different populations, diagnosis by sonography is feasible for both adults and children because the sonographic findings are the same.
Another treatment concern is operation on a healthy appendix. Diagnosis may often be uncertain and appendectomy called for, but a reduction of any unnecessary medical interventions should always be the goal. Use of imaging studies to complement the conclusion obtained during clinical examination of the patient has been shown to reduce the rate of unnecessary appendectomy 3-fold. 7 With the economic cost of sonography being relatively low compared to surgical intervention, and considering the social costs to the patient in terms of health and lifestyle following surgery, imaging studies should be pursued when the question of surgery arises.
Diagnostic imaging options all have their strengths and weaknesses. Computed tomography (CT) is reported in the literature to be the most accurate imaging modality, with up to 94-98% overall accuracy. 8 Because of this, CT is often used as the standard course of diagnosis where imaging studies are concerned.4,9 When clinical symptoms are insufficient for diagnosis, CT diagnostic imaging criteria for appendicitis include thickened appendix, presence of an appendicolith, and fluid or fat infiltration around the appendix (Figures 1 and 2). A study by van Randen et al found that if 2 or more of these features are found, CT had a sensitivity of 96%. 10 CT imaging has been shown also to have high specificity for appendicitis. 11 However, in some patients CT might not be the best choice, or can even be contraindicated. 7 Contrast utilization and radiation exposure are the greatest concerns with CT. There is an associated time delay between the administration of oral contrast and acquisition of images, potentially delaying the diagnosis. Though rare, allergic reactions and contrast induced nephropathy are additional risks,12,13 Patients with very little abdominal fat do not create the ideal image for CT diagnosis.1,10,14 As with any test, CT also does not detect 100% of cases of appendicitis. In such circumstances, sonographic reevaluation has been shown to decrease the rate of negative appendectomies and to increase the accuracy of diagnostic results. 15 Reports in the literature have shown that an effective sequence for diagnosis of appendicitis uses sonography as the first choice of imaging modality, using CT when there are negative or equivocal results.8,16,17 This approach takes advantage of the benefits of sonography while maintaining the “safety net” of CT.
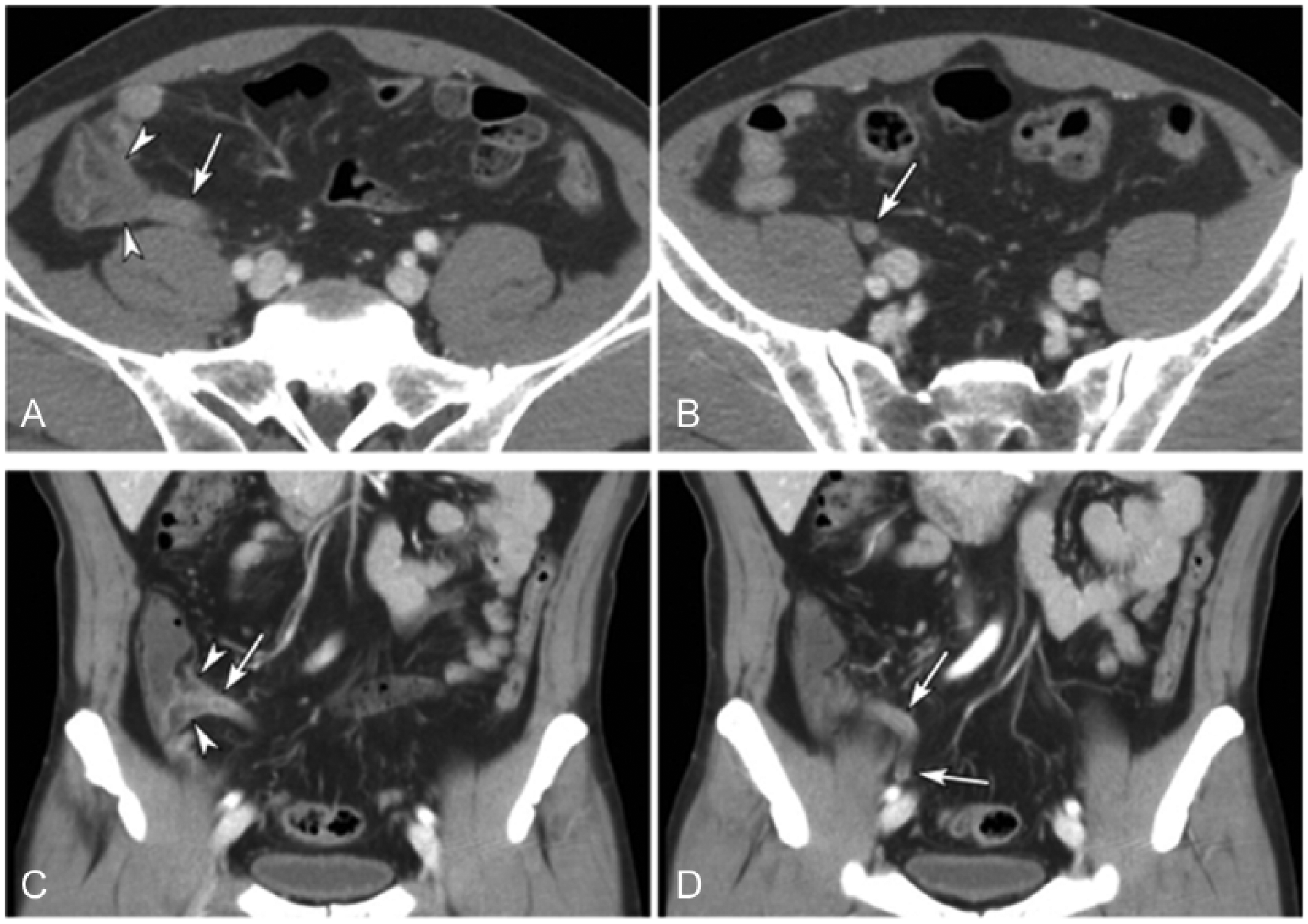
Cross-sectional computed tomographic (CT) abdominal/pelvic scans (A, B) and coronal reformation (C, D) acquired with intravenous contrast material show the thickened appendix (arrows) and edema in the cecum (arrowheads) at the orifice of the appendix. Reprinted with permission from the Open Access article Lee K, Kim Y, Hahn S, et al: Added value of coronal reformations for duty radiologists and for referring physicians or surgeons in the CT diagnosis of acute appendicitis. Korean J Radiol. 2006;7(2):87.
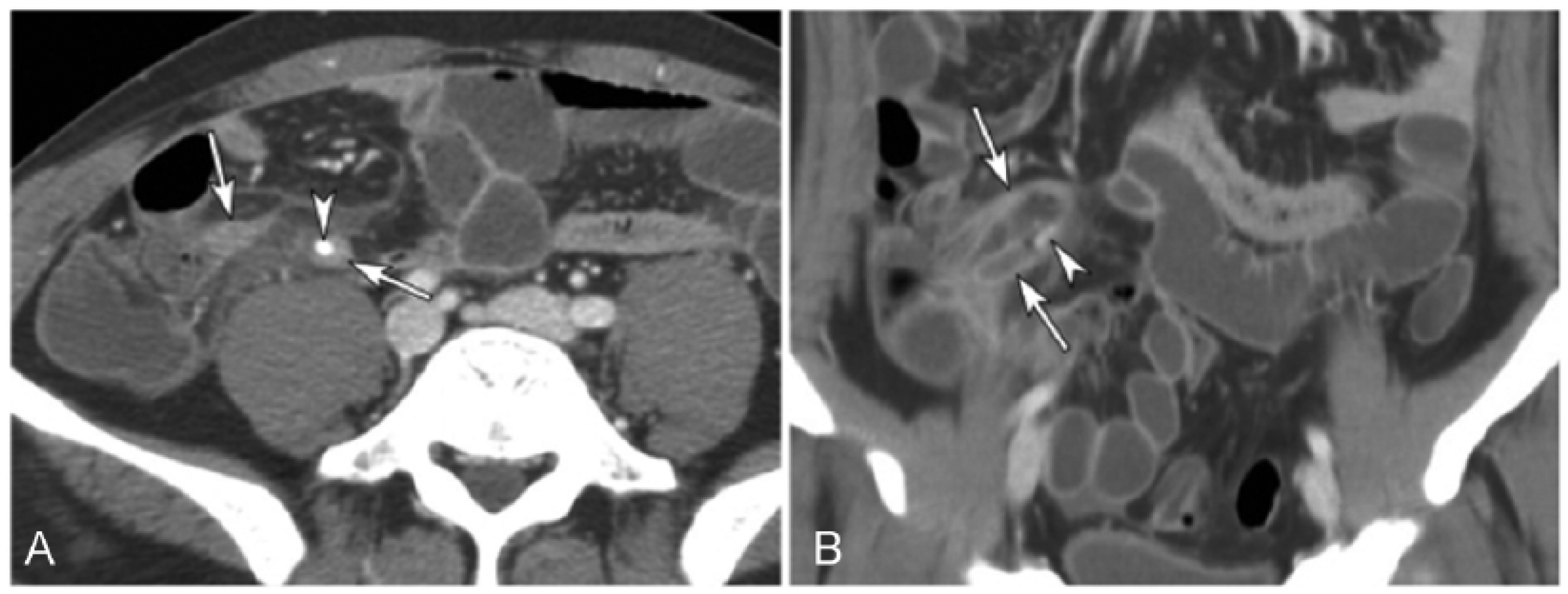
Cross-sectional computed tomographic (CT) scan (A) and coronal reformation (B) acquired with intravenous contrast material show distended appendix (arrows), an appendicolith (arrowheads), and peri-appendiceal fat stranding. Reprinted with permission from the Open Access article Lee K, Kim Y, Hahn S, et al: Added value of coronal reformations for duty radiologists and for referring physicians or surgeons in the CT diagnosis of acute appendicitis. Korean J Radiol. 2006;7(2):87.
Sonographic findings for the appendix include a blind-ended, noncompressible tubular structure arising from the cecum of the large bowel (Figure 3). 18 The anterior-posterior measurement of the tube should be greater than 6 mm to diagnose appendicitis (Figure 4).19,20 Additional characteristic findings are similar to the criteria for CT, including thickened appendix, presence of an appendicolith, and fluid or fat infiltration around the appendix. 21 Using color Doppler, a ring of hyperemic vascular flow will usually be seen in the tissue of this structure (Figure 5). 21 A transvaginal approach may be combined with the transabdominal approach to increase the success rate of diagnosis in female patients (Figures 6 and 7). There have been cases in which a negative transabdominal ultrasound was ruled positive using the transvaginal approach. 19 In particular, patient body habitus can keep the transducer further from the anatomy transabdominally. The transvaginal approach puts the transducer in closer proximity to the structure being visualized, increasing the visibility and clarity of the structure and therefore increasing the diagnostic yield of the study. In obese patients, transvaginal scanning can be instrumental in putting the anatomy closer to the transducer, allowing a higher transmit frequency and increasing the resolution of the image. Keeping the patient in the same examination room and being able to use the same ultrasound machine for transabdominal and transvaginal sonography yields a faster diagnosis, enabling the patient to undergo any needed surgery in a more timely fashion.
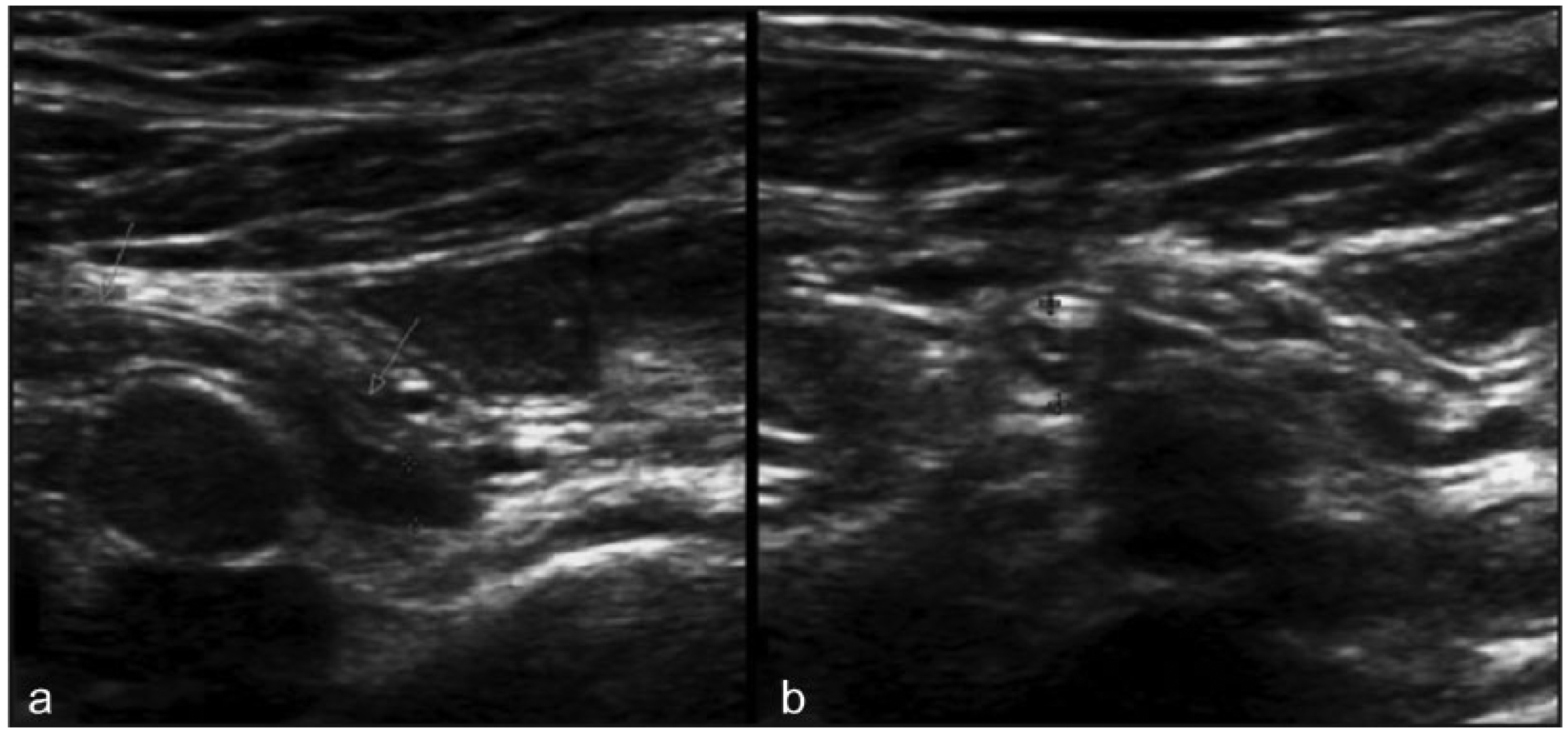
Gray-scale sonographic images of a normal appendix. (a) Long-axis view. (b) Short axis view. A blind-ended, gut-pattern tubular structure (arrows), with 2 mm wall thickness and 4.5 mm lumen width (cursors), is seen anterior to the right common iliac vessels on gray-scale sonographic graded compression. Normal appendix seen in this ultrasonographic examination ruled out appendicitis. Reprinted with permission from the Open Access article Gaitini D: Imaging acute appendicitis: state of the art. J Clin Imag Sci. 2011;1(3):49-57.
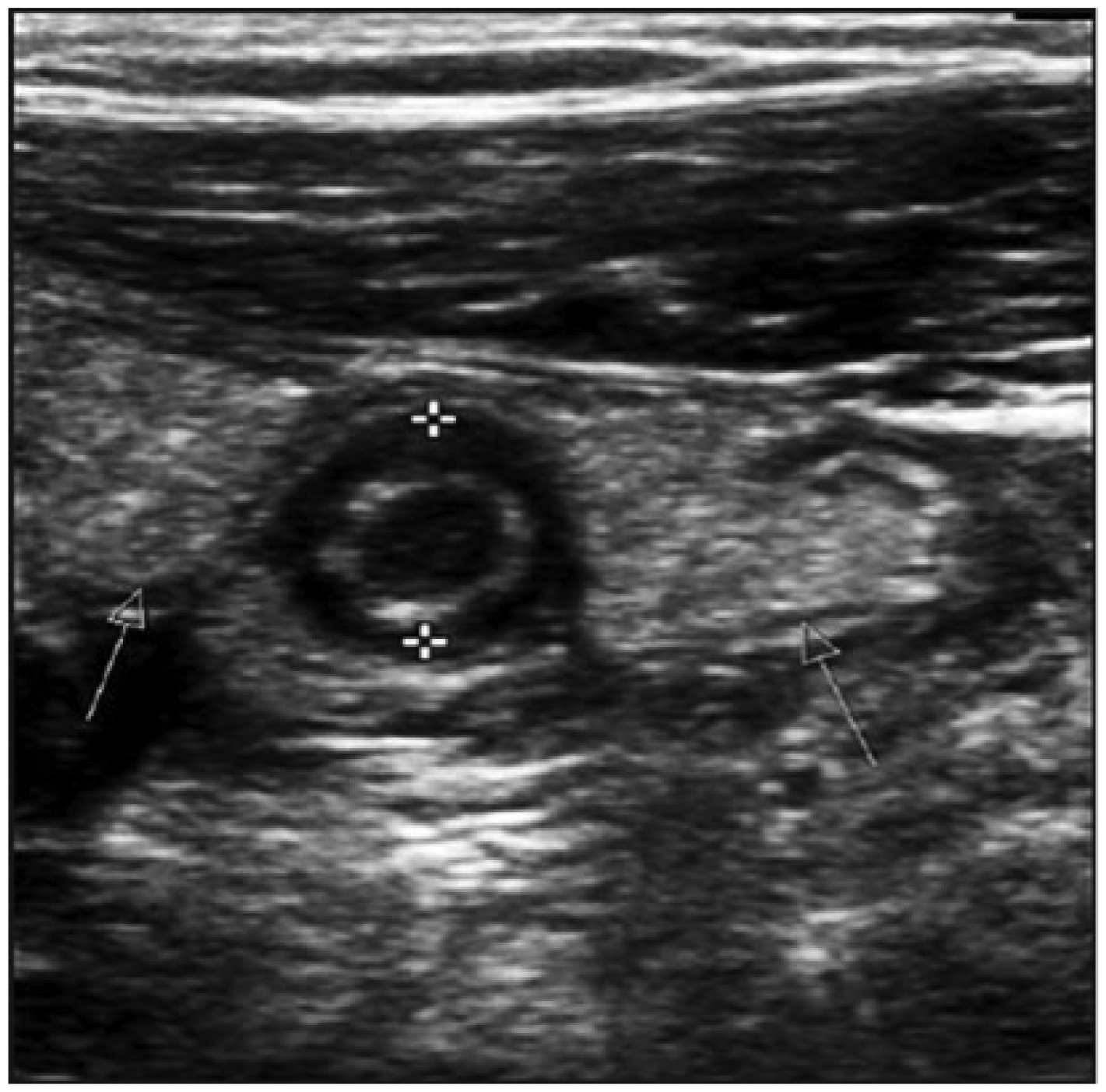
Gray-scale image showing mesenteric fat thickening surrounding acute appendicitis. Hyperechoic thickened mesenteric fat (arrows) surrounding 9.5 mm inflamed appendix (cursors) is seen on compression sonography. Reprinted with permission from the Open Access article Gaitini D: Imaging acute appendicitis: state of the art. J Clin Imag Sci. 2011;1(3):49-57.
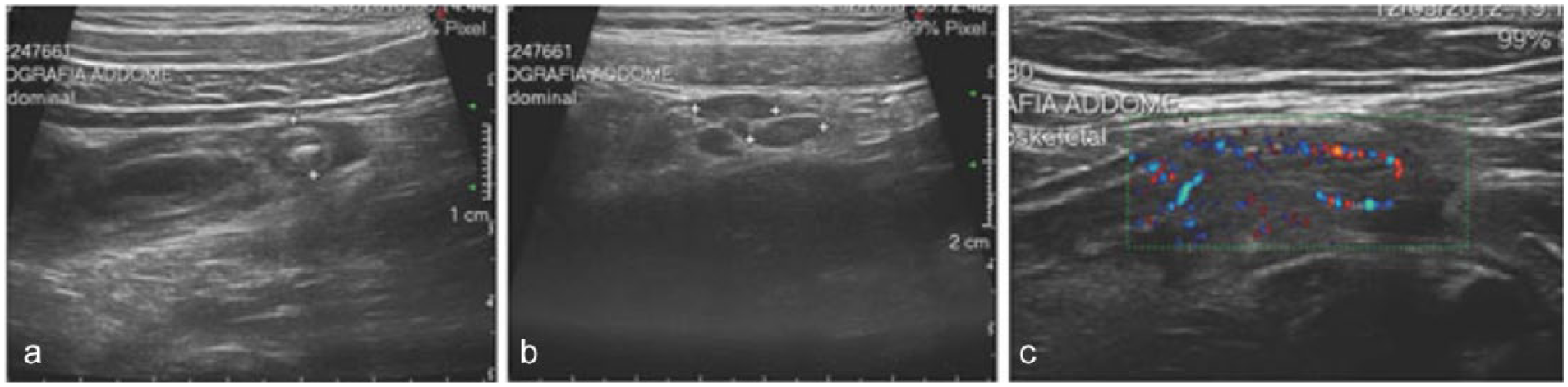
Gray-scale sonograms showing (a) enlarged (>6 mm, cursors) and thickened appendix with appendicolitis and a rim of peri-appendiceal fluid; (b) enlarged lymph nodes along the ileo-colic vessels (cursors); and (c) hyperemia in the appendix wall shown by color imaging. Reprinted with permission from the Open Access article Mazzei M, Guerrini S, Cioffi Squitieri N, et al: The role of US examination in the management of acute abdomen. Crit Ultrasound J. 2013;5(suppl 1, S6):1-9.
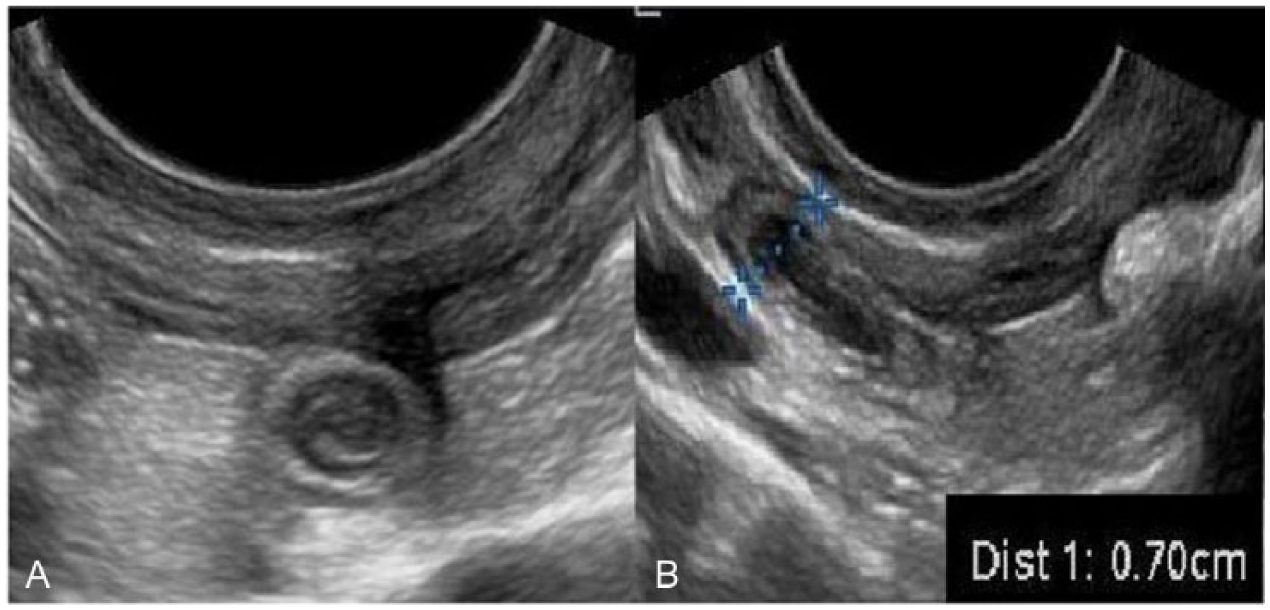
Transvaginal gray-scale sonographic imaging of the right adnexa. (A) Transverse view of the appendix. (B) Long view of the appendix measuring 0.7 cm (cursors). Reprinted with permission from the Open Access article Bramante R, Radomski M, Nelson M, Raio C: Appendicitis diagnosed by emergency physician performed point-of-care transvaginal ultrasound: case series. West J Emerg Med. 2015;14(5):415-418.
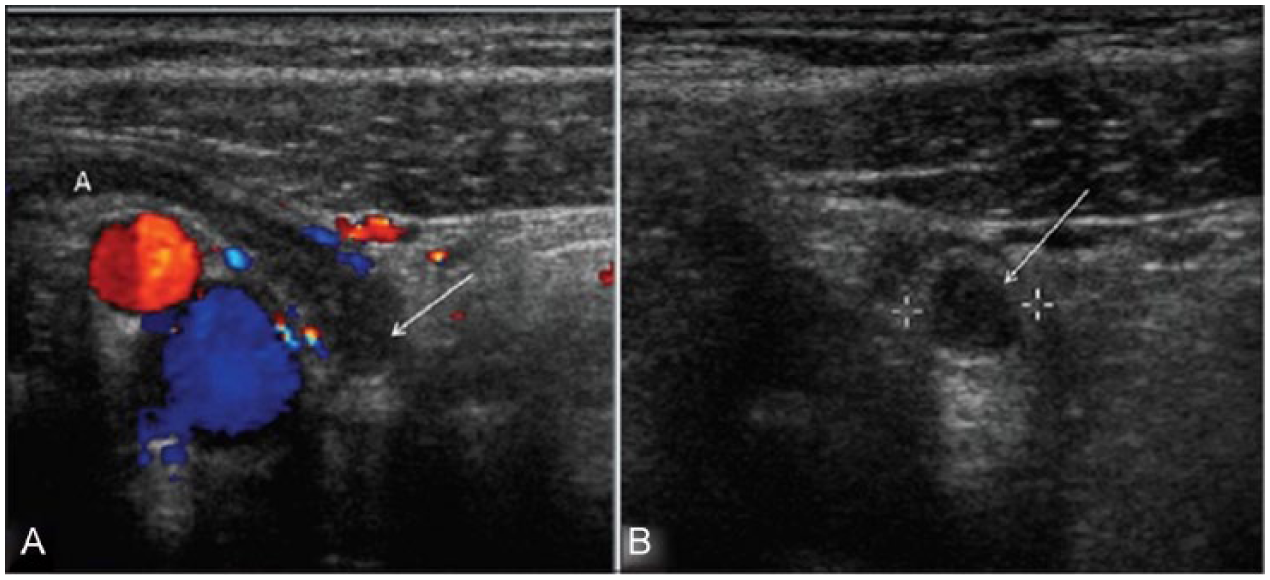
Sonographic imaging of focal appendicitis. (A) Longitudinal color Doppler image of the right lower quadrant shows an enlarged and hyperemic appendiceal tip (arrow) with a normal appearing proximal appendix. (B) Gray-scale transverse image of the right lower quadrant shows enlarged appendiceal tip (arrow; cursors). Reprinted with permission from the Open Access article Siegel M, Sargar K: Sonography of acute appendicitis and its mimics in children. Indian J Radiol Imag. 2014;24(2):163.
An additional benefit of sonography is the ability to simultaneously diagnose other possible causes for the patient’s symptoms. Right lower quadrant or acute abdominal pain in females, classic symptoms of appendicitis, can often coincide with female reproductive system pathology or gastro-intestinal disorders, which may include appendicitis. 22 Ovarian cysts and ectopic pregnancies, for example, are other common causes of acute right lower quadrant pain. 23 When the clinical history is not enough to make a definitive diagnosis, differentiating between these conditions with appropriate imaging is the key to making the diagnosis and pursuing the correct course of treatment. Requiring little waiting time or preparation, ultrasonography, especially transvaginal ultrasonography, is useful in diagnosing these conditions while at the same time evaluating the appendix if necessary, easing the strain on resources other tests may cause.22,24
Other symptoms that can lead to a clinical diagnosis of appendicitis include nausea, anorexia, and rebound tenderness. Frequently, cases do arise where the clinical symptoms do not coincide with such classic presentations of appendicitis or coincide with other pathology, and further diagnostic testing must occur.7,25 Children and seniors in particular can be difficult to evaluate effectively depending on their communication abilities. At the same time, risk of perforation increases with the extremes of age, leaving these populations more vulnerable to the dangerous sequelae of appendicitis. 26 Acute appendicitis is the most common surgical emergency in children, but children can be unwilling to cooperate with the examination or unable to describe their symptoms and their symptoms are also more likely to be atypical.27,28 In addition, risk of perforation increases in younger patients, with around a third of cases resulting in rupture before surgical removal can take place. 29 Diagnosis of appendicitis in children takes some finesse, with indiscriminate use of CT and the resulting radiation exposure not recommended. Seniors are another at-risk segment of the population who may be unable to share or describe their symptoms completely or accurately for various reasons. Risk of perforation in this group is also significantly higher than the general population, as much as 50%. 30 Difficulty in obtaining clinical symptoms, as well as equivocal laboratory results, can lead to an inability of the emergency physician to diagnose appendicitis in children or seniors accurately. This may increase the risk of perforation in those not surgically treated in time, as well as risk removal of a healthy appendix in those who are misdiagnosed with appendicitis. 31
A special case to be considered is appendicitis occurring during pregnancy. This requires immediate surgical attention, and is further complicated by the added risks to the pregnancy. Clinical signs of appendicitis during pregnancy are often not the classic ones, making the diagnosis more challenging to obtain. Clinical symptoms also may mimic other gynecologic or obstetric conditions, and laboratory values may not provide conclusive answers because of physiologic changes during pregnancy.32,33 As well as the usual complexities associated with appendicitis in the nongravid population, delay in diagnosis imposes an even greater risk of complications such as perforation, infection, preterm labor, and risks of fetal or maternal loss. 32 Greater reluctance to operate on a pregnant patient creates the need for careful diagnostic testing, starting with the least harmful type of test, making sonographic testing the first choice on the list of options. 34 CT testing on a pregnant woman involves radiation exposure to the mother and to the fetus, with the likelihood of development of childhood cancer doubling with 1 CT scan during the first trimester of pregnancy.30,35 Magnetic resonance imaging (MRI) is an alternative that does not pose the same complications of radiation exposure; however, the time to obtain an MRI and the cost can be prohibitive. 30 The safety of the mother and the fetus is a top priority, and sonography plays a prominent role in maintaining safe and critical care for these patients.36-39
Conclusion
Appendicitis is one of the most common causes for emergency department visitation, and diagnostic options should be thoroughly researched to provide the best patient care possible. Safe, rapid, and effective treatment should be of the utmost priority. Ability to use ultrasonography as a diagnostic technique at low cost to the hospital and low risk to the patient provides significant benefit to the population as a whole. Reliable results for any age group and any gender leaves little question as to the efficacy of this modality on a large percentage of the population. The safety and comfort of diagnostic sonographic testing gives the patient peace of mind that they will not have an adverse reaction to the testing or that they will have any lasting side effects. Sonography has been shown to reduce the rate of negative appendectomy, avoiding unnecessary surgical intervention. Sonography also has proven useful in finding other causes of right lower quadrant or abdominal pain, especially in the female population while using the transvaginal approach to evaluate pelvic structures.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.