
Abstract
Sonography plays a primary role in the diagnosis of gynecological diseases. A retrospective review of incidental findings report by transvaginal sonography (TVS) was performed to evaluate the ability of TVS to visualize rectosigmoid carcinoma. The authors performed a retrospective review of 450 women who were referred for TVS because of suspected gynecological indications to evaluate those with incidental findings. Of these, 15 with incidental findings were subsequently diagnosed with rectosigmoid carcinoma. The sonographic properties and clinical findings were systematically evaluated. TVS findings included solid nonhomogeneous lesions (mean diameter of 4 cm; range, 1.6–8 cm), distended rectal walls, and gas inside the gastrointestinal lumen in 53% (n = 8) of the cases. Total wall invasion was suspected, and signs of edema were noticed in 60% (n = 9) of the cases. All lesions seen by TVS were pathologically confirmed as carcinoma of gastrointestinal origin. Inspection of the rectosigmoid during a TVS examination has the ability to detect unsuspected rectosigmoid lesions.
Although sonography has become the primary diagnostic tool for most gynecological diseases, in gastroenterology and surgery, it has traditionally had little impact. Gas in the gastrointestinal cavity and the need for a large area of scanning limit the capability of sonography in evaluating the gastrointestinal tract.
The development of modern transvaginal transducers has greatly enhanced the quality of sonographic imaging of pelvic organs. High-frequency transducers of 7.5 MHz or higher, with their close proximity of the vaginal probe to the pelvic tissue, enable accurate visualization of the part of the rectosigmoid that is hidden in the lower pelvis, as well as of gynecological structures. 1
Currently, transvaginal sonography (TVS) is a diagnostic tool used for the diagnosis of gynecological problems of the uterus, ovaries, and adnexal areas. TVS has potential to enable detailed viewing of the layers of the bowel wall, as well as detection of edema, inflammation, and even neoplastic infiltration.2,3 Pathological alterations in bowel wall layering, thickness, and echogenicity, as well as peristalsis, are readily recognized. In addition, TVS differentiates suspected lesions located deep in the pelvis as gastrointestinal or gynecologic.
This retrospective review evaluated the ability of TVS to visualize incidental rectosigmoid carcinoma. MEDLINE search of the English literature from 1980 to 2010, with the terms transvaginal sonography, rectal carcinoma or sigmoidal carcinoma, ultrasound, rectal masses, and gastrointestinal, yielded only few articles; most are not from recent years and not related to the specific topic.
Materials and Methods
Medical records and sonographic data were retrospectively reviewed of patients from August 2006 to August 2008 who had TVS performed with the following gynecological indications: (1) pelvic pressure, (2) abdominal discomfort, (3) abdominal bloating, or (4) abdominal pain. Those cases with retrosigmoid lesions were compared with pathology that demonstrated rectosigmoid carcinomas by pathology.
All TVS was performed by the same operator (R.A.) with the HDI 5000 sonography system (Advanced Technology Laboratory, Bothell, Washington), using vaginal 4- to 8-MHz probes and convex 2- to 5-MHz transabdominal probes, or the IU22 machine (Philips Medical Systems, NA, Bothell, Washington).
A complete examination of the uterus, ovaries, and adnexa was performed, with the transducer aimed posteriorly at the rectoanal junction. The rectum and sigmoid were scanned as the transducer moved along the sigmoid up to 2 cm from the descending colon. Suspicious lesions were sagittally and transversely examined and recorded. Transabdominal sonogram was performed as needed when data from the TVS examination were not adequate or an upper lesion was suspected.
The following features were assessed from the TVS images obtained: (a) structure of the rectum wall and depth of invasion, (b) structure of prerectal fat, (c) echogenicity of the lesion, (d) gas inside the gastrointestinal tract lumen, and (e) boundaries and diameter of the lesion. Color or Doppler sonography was performed according to clinical judgment and therefore was not performed routinely.
Pathology reports describing final staging of tumors were collected for comparison to the sonographic features (i.e., wall invasion, echogenicity, and diameter). Analysis of variance (ANOVA) t test was used for statistical analysis with SPSS for Windows version 16 (SPSS, Inc., an IBM Company, Chicago, Illinois). P < .05 was considered statistically significant for all comparisons.
Results
During the above-mentioned period, 450 women were evaluated, of whom 15 had an incidental finding of a rectosigmoid lesion reported by TVS and were diagnosed by pathology with rectosigmoid carcinoma. None of the patients incidentally diagnosed with rectosigmoid carcinoma presented with vaginal or rectal bleeding. Their relevant demographic and clinical characteristics and final diagnoses are presented in Table 1.
Demographic and Clinical Data of the Study Group (n = 15)
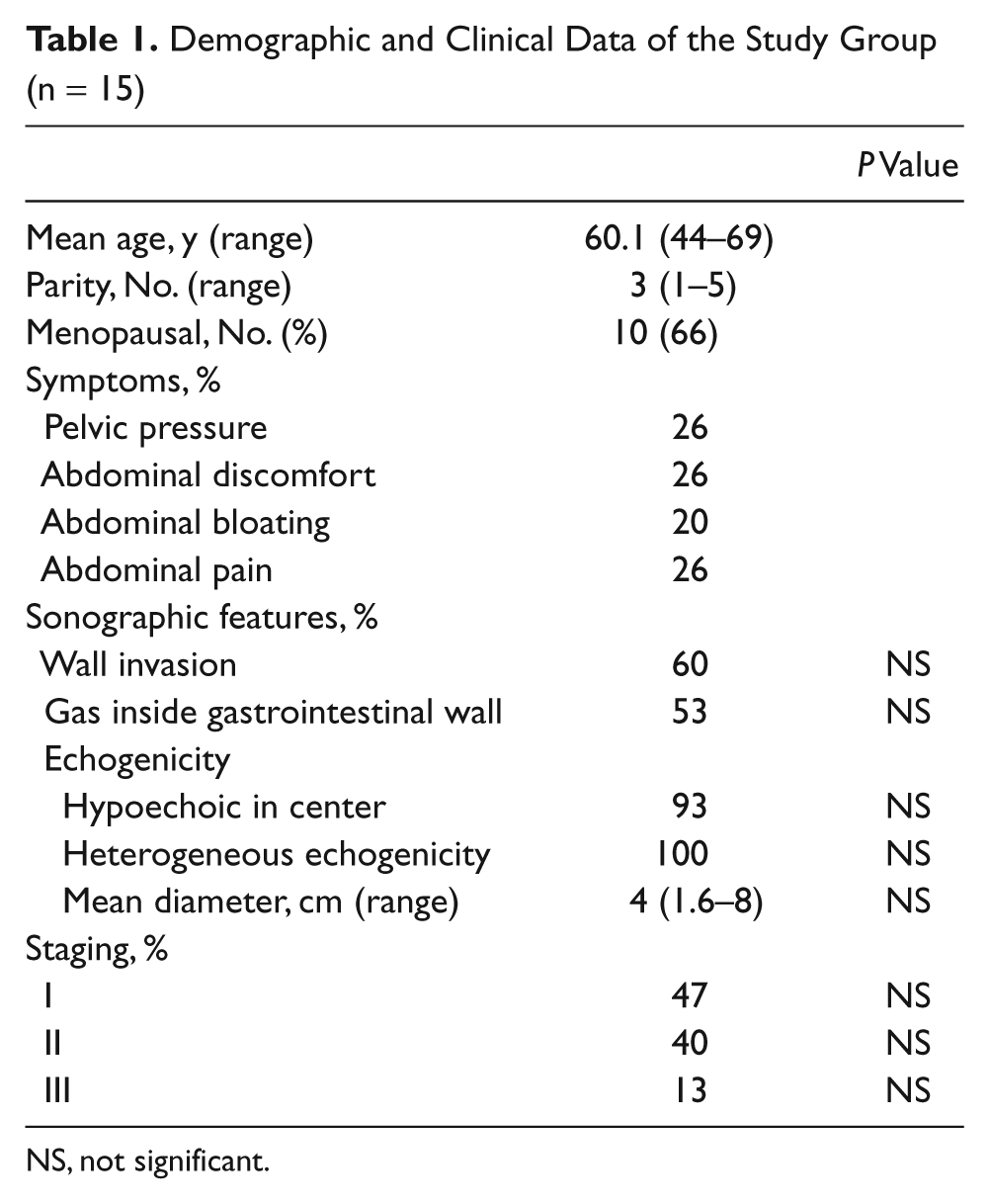
NS, not significant.
All TVS examinations were performed without complications. Some women reported discomfort during the sonographic examination, which lasted 10 to 15 minutes.
In one woman, the lesion was seen to invade the uterine cavity, with gas filling (Figure 1). None of the other lesions involved the uterus or ovaries.
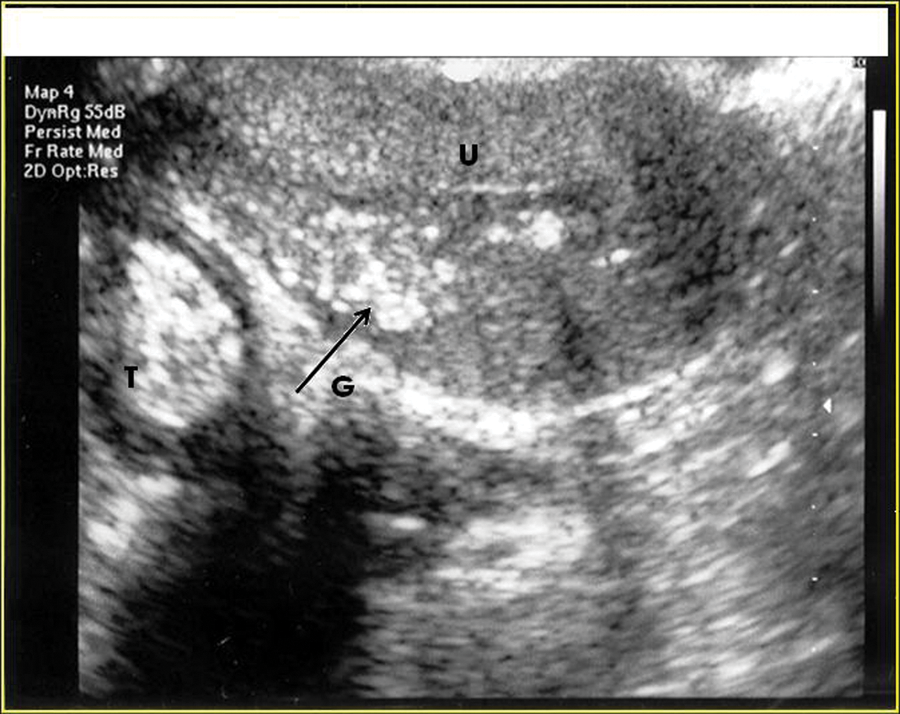
Lesion (T) seen invading the uterine cavity (U), with gas filling (G, arrow).
In those women diagnosed with rectosigmoid carcinoma, no other coexisting abnormalities of the genital tract were discovered during the sonographic examination. Gastrointestinal findings by TVS included distended rectal walls with solid nonhomogeneous lesions (Figure 2) 4 cm in mean diameter (range, 1.6–8 cm; Table 1). Irregular boundaries of the lesions and rectosigmoid walls were identified in all cases. Gas inside the gastrointestinal lumen was detected in 53% (8/15) of the women (Figure 3). All lesions except one were hypoechoic in the center; most were characterized by heterogeneous echogenicity in other parts of the lesion. In 60% (9/15), wall invasion was suspected, and signs of edema were seen (i.e., distended rectal wall) (Table 1). No correlations between sonographic findings and other clinical, demographic, or pathological characteristics were noted. Variables, including depth of invasion, diameter of the lesion, echogenicity, and gas inside the gastrointestinal tract lumen, with regard to staging of the tumor, age, parity, and clinical symptoms were compared.
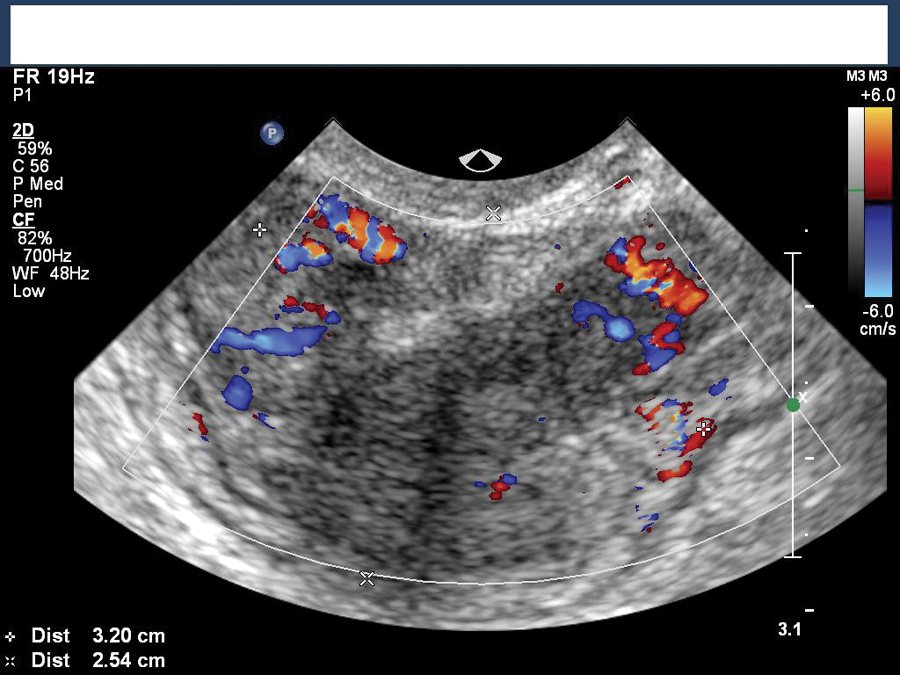
Rectosigmoid lesion showing blood vessels and distended lumen.
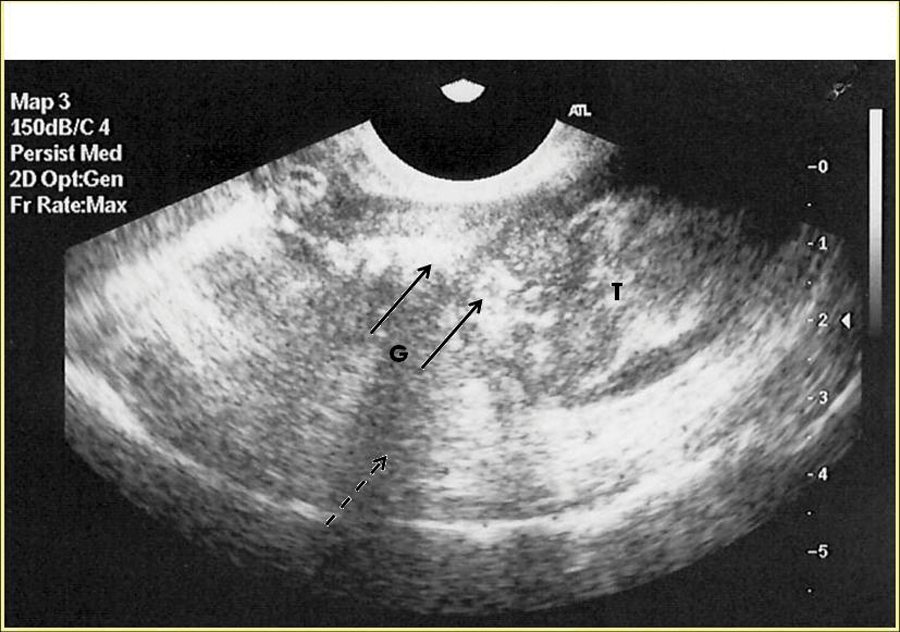
Gas inside the gastrointestinal lumen (G, arrow) was detected in 58% of the cases, appearing as an acoustic shadow beneath (broken arrow). The tumor is marked near the lumen (T).
Rectosigmoid carcinoma was confirmed histologically in all 15 women with a solid lesion in the rectosigmoid, after a biopsy was taken, either by definitive surgery or by other diagnostic procedures, such as sigmoidoscopy or rectoscopy.
A comparison between the staging of tumors and the sonographic features (i.e., wall invasion, echogenicity, and diameter), using the ANOVA t test, was not statistically significant.
Discussion
Although sonography is not widely used to diagnose bowel pathology, a variety of bowel lesions can be identified during routine abdominal and pelvic studies and TVS. TVS performed with a high-frequency probe provides high-resolution images not only of the uterus and ovaries but also of portions of the urinary and gastrointestinal tract in close proximity to the vaginal vault. Nongynecologic pathologic conditions can thus be diagnosed.4,5
Compared with TVS, endorectal sonography is less comfortable and is limited both in its ability to evaluate stenotic lesions and in its poor visualization of high rectosigmoid tumors. 6 TVS was found to be an excellent adjunct to endorectal sonography in the staging of rectal cancer in women and may be particularly helpful when endorectal sonography is unsuccessful due to tumors that are stenotic or in a high or low position.7,8
The use of TVS has been documented for other gastroenterological conditions. Inflammatory bowel disease (IBD) usually presents as a lower gastrointestinal inflammatory process with a distended gastrointestinal wall; thickened, irregular mucosa; and deep ulcerations. 9 In Crohn disease, fistula formation, strictures, and inflammatory process such as pelvic abscess and perianal lesions can be identified. A bowel loop with edema, increased thickness, and the presence of diverticulitis in the descending colon on the left side near the left adnexa may suggest diverticulitis. 10
Although transabdominal sonography often does not identify the normal appendix, TVS in women of childbearing age with fever, pelvic pain, or pelvic mass can lead to a correct diagnosis of acute appendicitis by differentiating it from gynecologic and gastrointestinal disease. 11
Staging of colorectal carcinoma can be defined by the following characteristics, including the depth of tumor penetration through the rectal wall, lymph node involvement, and presence of distant metastatic disease:
Stage I: The cancer has grown through the muscularis mucosa into the submucosa.
Stage II: The cancer has grown into the outermost layers of the colon or rectum or through the wall of the colon or rectum. It might also be attached to or has grown into other nearby tissues or organs.
Stage III: It has spread to nearby lymph nodes.
Stage IV: It has spread to one or more distant organ.
Preoperative staging is used to determine the indication for neoadjuvant therapy, as well as deciding between local excision and radical cancer resection. 12 Endorectal sonography is usually preferred to computed tomography and conventional magnetic resonance imaging in the preoperative local staging of rectal tumors.6,9,13,14 According to currently available data, endorectal sonography is 72% to 95% accurate for tumor staging and 61% to 83% accurate for nodal staging. 15 Yet, it is limited by its steep learning curve, interobserver variability, and limitations for staging of near-obstructing tumors.
The limitations of this study include being a limited pilot retrospective study, with a small sample size, that is applicable only to women and only those with gastrointestinal lesions proximal to the vaginal canal. Further prospective studies with larger sample sizes are needed to determine the specificity and sensitivity of TVS compared to other diagnostic methods in the evaluation of lower gastrointestinal malignancies.
Conclusion
Gastrointestinal lesions, especially rectosigmoid lesions, are included in the differential diagnosis of gynecological pathologies. General surgeons and gastroenterologists should be familiar with the applicability of TVS for the inspection of the rectosigmoid during gynecological examinations.
The addition of a rectosigmoid inspection to a routine gynecological TVS examination seems a useful diagnostic measure for discovering unsuspected rectosigmoid cancer or other gastrointestinal pathologies and therefore should be included in the routine female pelvis sonographic examination.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.