
Abstract
Objective:
Community-acquired pneumonia (CAP) is a common respiratory infection, and diagnosis is frequently performed using a chest radiography (CXR). Sonography is an available method with less radiation exposure, but has not been confirmed for diagnosis of CAP. The objective was to compare the diagnostic accuracy of sonography.
Materials and Methods:
In this cross-sectional study, 90 adult patients (aged >18 years) were admitted to the emergency department of two university-affiliated hospitals in Southwest Iran, from July to December 2019, with a confirmed diagnosis of CAP. The patient symptoms and CXR results were included as part of this study. Within 24 hours after obtaining a CXR, a lung ultrasonogram (LUS) was performed. The diagnostic accuracy of semiquantitative LUS (SQLUS) was compared with CXR results using the Pearson chi-square test and Fisher’s exact test.
Results:
The mean age of participants was 52.98 ± 16.77 years. 51 were men (56.7%). 28 patients (31.1%), who had abnormal SQLUS results, were not associated with CXR findings (P = .296). SQLUS showed poor diagnostic accuracy for LUS (31.11%).
Conclusion:
This study results could not confirm LUS as an accurate method for diagnosing CAP in adult patients; although due to the convenient sample of adults and clinical-based diagnosis of CAP, any generalization of the results should be made with caution.
Community-acquired pneumonia (CAP) is a respiratory infection that involves small airways and pulmonary parenchyma, and has an overall incidence of 1.54 to 1.7 per 1000 population, increasing with age, resulting in an incidence of 14 per 1000 person-years in the elderly (aged ≥65 years). 1 It is mainly a disease in an outpatient setting; however, severe cases may require an inpatient admission or to the intensive care unit (ICU). Of these admissions, some may end with death or morbidities, 2 which is considered the most common cause of death, due to infection, in developed countries and one of the leading causes of overall mortality in developing countries, especially in children aged below 5 years. 3 The mortality rate of CAP is also high in critically ill patients, patients with comorbidities, and the elderly. 4
Early diagnosis and timely initiation of appropriate antibiotics are associated with prognosis and mortality. 5 Nevertheless, the absence of reliable diagnostic tools is one of the main challenges in low- and middle-income countries. 6 Although a chest radiograph (CXR) is considered a reliable method for diagnosis of CAP 7 and introduced as a valuable tool for differential diagnosis of CAP from coronavirus disease 2019 (COVID-19), 8 it has some inefficiencies in distinguishing CAP from other types of pneumonia, diagnosis of pleural effusion, its interpretation depends based on the reader, and it may also not be available at all centers. 9 Accordingly, sonography has been suggested as an alternative diagnostic method, especially in resource-limited settings 10 and in children. 11 Lung ultrasonography (LUS) has been suggested to distinguish the etiology of CAP in children 12 and may also be effective in monitoring the children’s response to treatment. 13
LUS has also been suggested as superior to a computed tomogram (CT), of the chest, for the diagnosis of CAP. 14 Some have proposed that LUS is beneficial and superior to CXR for the diagnosis of CAP. Besides the availability, fast access, and performance duration, as well as less radiation exposure, it is a valuable diagnostic tool 15 that could soon replace the CXR. 16 However, a meta-analysis of studies has cast doubt on the quality of the studies and has suggested LUS as an additional and adjuvant diagnostic tool. 17 It is not yet included in the clinical guidelines for the diagnosis of CAP. Different studies has shown that CXR for detection of pulmonary opacities and pneumonia had a sensitivity of 43.5%–67%, specificity of 85%–93.0%, a positive predictive value of 26.9%, and a negative predictive value of 96.5%.18,19 The LUS examination has a sensitivity of 82.8%–98% and specificity of 95%–97.7% for diagnosing pneumonia.19–21 Other imaging techniques such as a chest CT and LUS are not accessible, and trained and experienced people for evaluation and doing those are not present in all areas. Hence, a CXR is the preferred screening method. The present study was designed as a pilot study to explore the diagnostic accuracy of imaging techniques, as additional diagnostic support for a clinical-based CAP diagnosis.
Materials and Methods
Study Design
In the present cross-sectional study, adult patients (aged >18 years) were admitted to the emergency department of a hospital in Southwest Iran, from July to December 2019. Patients were admitted with a confirmed diagnosis of CAP, based on clinical signs and symptoms (including cough, sputum, shortness of breath, with fever or shivering) and CXR findings (consolidation/air-space opacification) were included. The posterior–anterior (PA) radiographic view was performed for all patients, and a pulmonologist and a radiologist assessed the results if there was uncertainty.
All patients with the inclusion criteria (age >18 years, clinical symptoms including cough, sputum, shortness of breath, fever or shivering, and CXR findings compatible with pneumonia) were enrolled in the study. The patients were selected using a nonrandom method and formed a convenient sample. The Ethics Committee of Shiraz University of Medical Sciences approved the study protocol (code: IR.SUMS.MED.REC.1398.264). The study objectives and steps were explained to the eligible patients, and the written informed consent was provided to them to read and sign. All ethical considerations of the latest version of Helsinki’s declaration on human studies were met throughout the study.
Within 24 hours after a CXR, a radiologist performed a LUS for the patients using a Esaote ultrasound equipment system (Esaote Medical Systems, Firenze, Italy) and a 3.5–5 MHz convex transducer. The radiologist who performed the LUS was unaware of the results of the patients’ CXR results. The posterior part of the chest was examined in the sitting or lateral decubitus position and the anterior section in a lying or semi-sitting position. All intercostal regions were examined. Each hemithorax was examined for each intercostal space in line with midclavicular, parasternal, axillary, and paravertebral lines. The reported outcomes included necrotic areas, air bronchogram, and local pleural effusion if present. Normal aeration was defined as the presence of lung sliding with A lines or fewer than two isolated B lines and was scored as 0; Multiple, well-defined B lines were considered as moderate loss of lung aeration and were scored as 1; Multiple coalescent B lines considered as severe loss of lung aeration and was scored as 2; lung consolidation defined as the presence of a tissue pattern characterized by dynamic air bronchograms and was scored as 3. 22 The inferior sections of the lungs were also examined. The main objective was the diagnostic accuracy of semiquantitative lung ultrasonogram (SQLUS), positive and negative, compared with their CXR.
The researcher recorded patients’ information in the study’s checklist, which included patients’ demographics (age and gender), underlying diseases, including diabetes mellitus (DM), hypertension (HTN), chronic kidney disease (CKD), ischemic heart disease (IHD), chronic obstructive pulmonary disease (COPD), as well as cigarette and hookah smoking presence of any consolidation on their CXR was recorded.
Statistical Analysis
The variables were described by mean ± standard deviation (SD) or number (percentage). The categorical variables were compared using the Pearson chi-square test and Fisher’s exact test. The continuous variables were compared between the groups using nonparametric tests, the Wilcoxon or Friedman test, according to the results of the one-sample Kolmogorov–Smirnov test; the sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and diagnostic accuracy using standard equations. IBM SPSS Statistics for Windows version 21.0 (IBM Corp. 2012. Armonk, NY, IBM Corp.) was used for statistical analysis. Statistical significance was set at a P value of <.05 and this was determined a priori.
Results
During the study period, 286 patients were assessed for possible diagnosis of pneumonia, and 90 patients with a confirmed diagnosis of CAP based on the constellation of suggestive clinical features, radiologic findings, and clinical decisions by the physician were included in this study with a mean age of 52.98 ± 16.77 years (minimum of 19 and maximum of 90 years). Among all patients, 51 were men (56.7%). The mean age of male patients was 52.02 ± 17.32 and that of females was 54.23 ± 16.16 years (P = .368). The frequency of underlying diseases was as follows: IHD in 19 patients (21.1%), DM in 15 patients (16.7%), HTN in 11 patients (12.2%), COPD in nine patients (10%), and CKD in seven patients (7.8%). Among all patients, 58 never smoked, 23 were current smokers, three were ex-smokers, and seven (7.8%) smoked hookah routinely. Seventy-eight patients (86.7%) had cough, 67 patients (74.4%) had dyspnea, and 63 patients (70%) had fever.
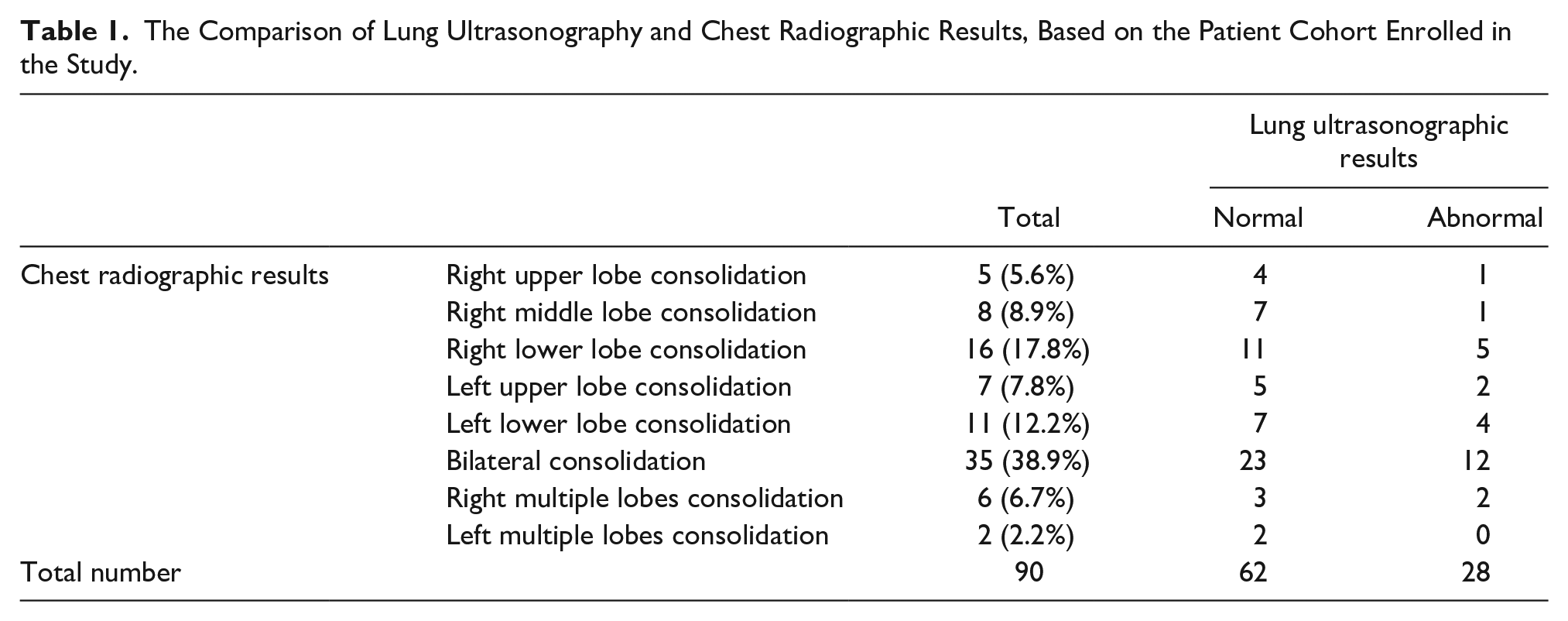
According to the results of QLUS, 28 patients (31.1%) had abnormal LUS results. Comparing the results of normal/abnormal ultrasound with CXR results (see Table 1). There was neither significant association between the results of CXR and LUS in general (P = .296; Table 1) nor according to patients’ sex (P = .368; data not shown). The findings of LUS were as follows: B line was present in four patients (4.4%), air bronchogram in 12 (13.3%), pleural effusion in six (6.7%), consolidation in six patients (6.7%), and 62 patients had normal test results (68.9%) (see Table 2). Six cases had pleural effusion on LUS, while two had effusion on their CXR.
The Comparison of Lung Ultrasonography and Chest Radiographic Results, Based on the Patient Cohort Enrolled in the Study.
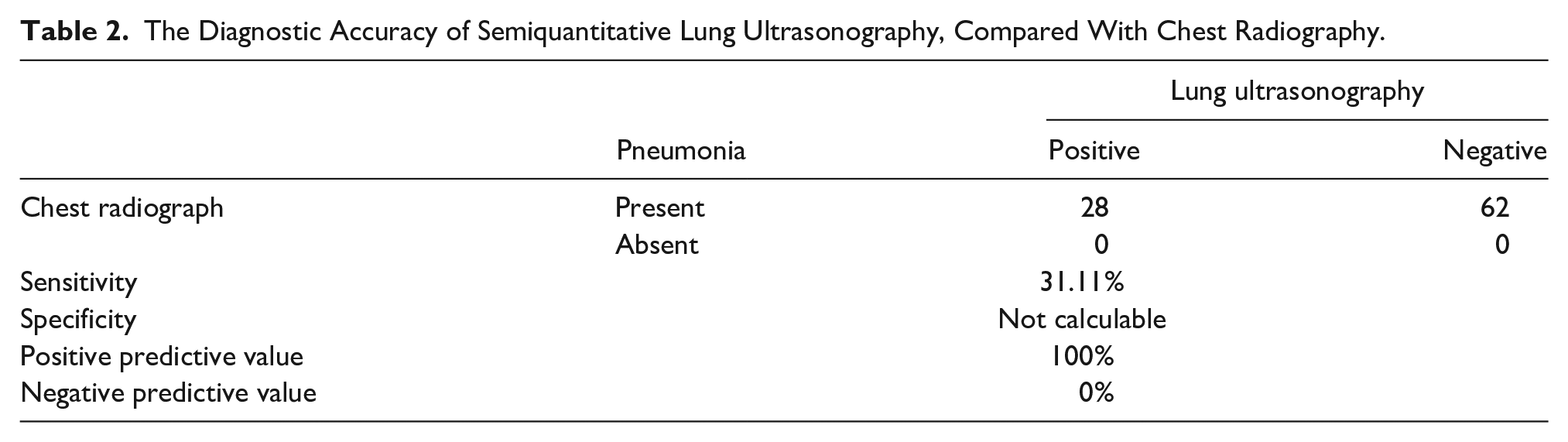
The Diagnostic Accuracy of Semiquantitative Lung Ultrasonography, Compared With Chest Radiography.
Discussion
In this study, examination of adult patients with CAP, whose diagnosis was confirmed by clinical signs and CXR results, showed that LUS could neither be an accurate diagnostic tool in the diagnosis of cases with or without CAP nor in the identification of consolidation and other imaging signs of CAP, compared with CXR. These results would suggest that LUS could not be suggested as an appropriate alternative for CXR in the diagnosis of CAP, which seems to be in contrast with most of the previous studies in this regard, reporting a high diagnostic accuracy for LUS in patients suspected of CAP.10,11,13,15,23 Some studies have focused on the pediatric population,11,12,24 which were not reviewed, as the diagnostic approach of pediatric CAP is different from that of adults,3,25 which was the target population of this study. Other studies have also reported a higher diagnostic accuracy for LUS in the diagnosis of pneumonia, in general,17,23,26–28 which were not discuss here, as we only focused on the diagnosis of CAP.
In this study, 28 of 90 patients were diagnosed with CAP based on sonography, which resulted in a sensitivity of 31.11%, and consolidation was only reported in six cases by LUS, compared with 90 cases by CXR. If the cases with air bronchogram on LUS are considered as consolidation, 18 cases were diagnosed by LUS, which is then much lower than that reported by the CXR (90 patients). These results would suggest an inaccuracy of LUS in the diagnosis of CAP compared with CXR. In a study performed in East Azarbaijan, a comparison of LUS results with CXR-confirmed CAP patients showed a sensitivity of 93.1% for LUS, 29 which contradicts this study results. However, that study only included 30 patients, and the results might be unreliable due to the small sample size. One of the differences between the current study results and previous research can be attributed to patients’ methodology and inclusion criteria, as we only included patients with a confirmed diagnosis of CAP by CXR.
In contrast, other studies have considered all patients suspected of CAP based on clinical signs and symptoms. Some others have also included other diagnostic methods, like CT, in their study. In a study on 62 patients suspected of CAP according to clinical signs and symptoms, LUS showed higher diagnostic accuracy for diagnosis of CAP-related consolidation than CXR (74.2% vs 51.6%, respectively), 15 which is contrary to the results of this study. In the study by Reissig and colleagues, investigating 262 patients suspected of CAP with LUS showed a sensitivity of 93.4% and specificity of 97.7%, compared with the reference test, a two-plane radiograph, or CT scan in cases with a negative radiograph, but positive LUS results. 21 In a low-income country, 44 patients with CAP, confirmed by CT, were compared with LUS and CXR. The results showed that LUS had a higher sensitivity and specificity for the diagnosis of CAP (91% and 61%, respectively), compared with CXR (73% and 50%, respectively), in adult patients who were referred to the emergency department (ED) and were suspected of pneumonia based on clinical signs and symptoms. 10 In a pilot study on 32 patients suspected of CAP, a comparison of the results of QLUS and CXR with the CT showed that considering QLUS resulted in the highest sensitivity and specificity (93% and 95%, respectively). 30 Interestingly, the visual sonography had a lower sensitivity and specificity (68%), which was close to that of CXR (64%); even, the sensitivity and specificity of combination of QLUS and the visual sonographic method (77%) were lower than QLUS alone. 30 Accordingly, another reason for the difference in the results of the studies could be related to the consideration method of positive CAP on LUS, as we considered QLUS for calculating the diagnostic accuracy.
In contrast, others have considered visual sonography results or have not reported the diagnostic method in their article.10,11,13,15,21,23 In addition, both diagnostic methods, CXR, and LUS, are operator-dependent, and the different levels of experience of the LUS operator and CXR interpreter can affect the results of studies. More studies are required for a definite conclusion on this issue because of the differences in the methodology, inclusion criteria, evaluation method, and operator’s precision among studies.
Another notable aspect of the present study’s findings was related to the LUS findings that could not be reported by CXR, including B line and pleural effusion. Other studies have also reported LUS findings in patients with CAP as important diagnostic measures, 21 which, in line with this study results, shows that CXR also has its inefficiencies. The B lines are considered an essential sign of subpleural interstitial edema and correspond to ground-glass opacities on the chest CT, 31 which has been noted as important for differentiation of pneumonia from COVID-19, however not be detected by CXR. 32 Taghizadieh et al 29 also reported that a CXR had a lower sensitivity for pleural effusion diagnosis than LUS (66.7% vs 92.3%, respectively). Others have also confirmed the low sensitivity of CXR in the diagnosis of pleural effusion and pneumothorax, compared with LUS, 33 which are in line with the present study results. Amatya et al have advocated that neither LUS nor CXR could diagnose lesions in the middle of the lung parenchyma, without extension to the pleura. 10 In a meta-analysis of five articles (742 patients with CT-confirmed CAP), the results of comparing LUS and CXR with CT showing higher sensitivity and specificity for LUS (95% and 86%, respectively) compared with CXR (77% and 91%, respectively). 14 Although these results confirm the high diagnostic accuracy of LUS for CAP, which is contrary to this study results, this meta-analysis refers to the fact that CXR also has several limitations in the diagnosis of CAP, which confirms the results of this study, as discussed above.
One of the strengths of this study was the inclusion of patients with a definite diagnosis of CAP, based on CXR results, for calculating the diagnostic accuracy of LUS. In contrast, previous studies have considered patients suspected of CAP based on clinical signs/symptoms, including other differential diagnoses.
Limitations
The study sample size gives limited information about the diagnostic accuracy of LUS. In addition, this was a convenient sample of adults, which makes any generalization of the results questionable. Another limitation of the study is selection bias related to the fact that we have collected the data from two teaching hospitals in one city; thus, the studied patients may not be representative of the whole Iranian population. However, as the two hospitals are two of the leading referral centers, therefore it is possible that the study population represented a significant cohort within Shiraz. In this study, all LUSs were performed by one expert sonographer to reduce the bias. Nevertheless, their operator-dependence nature affects the preciseness of the results of both of the studied methods, CXR and LUS.
Conclusion
This study results could not suggest LUS as an accurate method for diagnosing CAP in adult patients admitted to the internal ward, contrary to the results of previous studies. Although, convenient sampling methods and clinical-based study design make to consider any generalization with caution. Further studies on other target populations are required, such as outpatients and children.
Footnotes
Acknowledgements
The present study was extracted from the thesis written by Jila Rahmanian.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Vice-chancellor for research of Shiraz University of Medical Sciences financially supported the present study (grant no. 19654).
Ethics Approval
Ethical approval for this study was obtained from the Ethics Committee of Shiraz University of Medical Sciences (code: IR.SUMS.MED.REC.1398.264).
Informed Consent
Informed consent was not sought for the present study because all case data were de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).
Animal Welfare
This research did not involve the use of animals.
Trial Registration
Not applicable.