
Abstract
Objectives:
A chest radiograph (CXR) is still the preferred diagnostic method when pneumonia is suspected, although the sensitivity is relatively low. The aim of this study was to compare the diagnostic sensitivity, specificity, and accuracy of ultrasonography (US) for the diagnosis of community-acquired pneumonia (CAP), compared with CXR.
Materials and Methods:
A principled search was conducted to identify original English articles using PubMed, EMBASE, Web of Science, Scopus, and the Cochrane library, with the end date of October 2020. A combination of keywords, such as “ultrasound” or “ultrasonography,” “pneumonia,” “sensitivity,” and “specificity,” was used. Methodologic quality was assessed using Quality Assessment of Diagnostic Accuracy Studies 2 criteria. Statistical analysis was completed on the resulting study data.
Results:
The search produced 16 eligible articles that reported on 2040 patients. The overall pooled sensitivity for US and CXR, to diagnose pneumonia, was 0.96 and 0.65, respectively. The overall pooled specificity for US and CXR was 0.85 and 0.81, respectively. The overall pooled positive likelihood ratio for US and CXR was 9.74 and 3.67, respectively. The negative likelihood ratio for US and CXR was 0.05 and 0.42, respectively. In addition, summary receiver operative characteristics areas under the curve were 0.98 for US and 0.77 for CXR.
Conclusion:
This review demonstrated that lung US is a useful technique for the diagnosis of pneumonia. This diagnostic method can be used by emergency physicians with high accuracy, sensitivity, and specificity. Among an elderly population, this diagnostic method may be a better choice than CXR. The rapid performance of lung US may facilitate a quick, cost-effective, and safe diagnosis of this potentially fatal disease.
Pneumonia is a common and potentially life-threatening disease, which is associated with increased morbidity, mortality, rate of hospitalization, and health care costs. Community-acquired pneumonia (CAP) is the most common type of pneumonia. The incidence of CAP has remained stable over the past few decades, affecting 3–5 of every 1000 people. 1 The diagnosis of CAP is mainly based on a history of cough, pleuritic pain, dyspnea, and physical examination, depending on patient cooperation. In general, hospitalization testing is reserved for adults in poor general condition with several underlying diseases and complications, and this results in a majority of test results on elderly patients.2 –4 According to US guidelines, the presence of an infiltrate, in the lung parenchyma, demonstrated on chest imaging is diagnostically required to confirm pneumonia.3 –5 Currently, chest radiography (CXR) is still the desired diagnostic method when pneumonia is suspected, although its sensitivity is relatively low (reported to be 43.5%–82.8% in studies).6 –9 Exacerbation of the patient’s clinical condition determines whether a CXR should be performed in the upright or recumbent position. Elderly patients who need hospitalization due to pneumonia are often disabled. This limits the diagnostic quality of the CXR, in the anterior-posterior view, for patients with limited mobility. As a result, the sensitivity and specificity of the CXR, for pneumonia, are further reduced.10,11
Additionally, there are problems with intrahospital transfer of an elderly patient for an imaging examination. However, many clinical units, including emergency and internal medicine departments, are now equipped with ultrasonography (US). Lung US has been shown to be more appropriate for diagnosing pneumonia, especially when performed on a hospitalized patient.6,9,12 –14 Another imaging method is computed tomography (CT), which has been considered as the diagnostic gold standard for the evaluation of lung parenchyma disease. However, there are several limitations that can affect the feasibility of this diagnostic tool, such as radiation, expense, limitations for critically ill patients, and those who have difficulty moving due to severe ventilatory support. US is a rapid and noninvasive examination that is frequently used in emergency department (ED). Several studies have shown that bedside US can help in diagnosing cardiogenic pulmonary edema, pneumothorax, and pulmonary embolism.15 –18 Currently, the diagnosis of CAP, via bedside US, is dependent on the detection of a consolidation (defined as a normally compressible region that is filled by liquid instead of air).19,20 However, patients with CAP do not always have a consolidation, but may have interstitial pneumonia or sporadic pulmonary infiltration. Even if consolidation is not diagnosed, other anomalies might be found by US, such as focal interstitial pattern and pleural anomalies. The objective of this study was to compare the diagnostic sensitivity, specificity, and accuracy of US on the diagnosis of CAP, compared with CXR.
Materials and Methods
Research Design and Source of Data
This systematic review was conducted according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). It was designed as a search for original English articles using PubMed, EMBASE, Web of Science, Scopus, and the Cochrane library, from January 2000 to October 2020. A combination of keywords, such as “ultrasound” or “ultrasonography,” “pneumonia,” “sensitivity,” and “specificity,” was used. All eligible studies were retrieved, as part of the systematic search. The bibliographies of the retrieved articles were independently searched and approved as a source for additional articles. These measures were completed to ensure the completeness and quality of the analysis. Studies that were published only in the form of abstracts were not included in the study. The articles were evaluated by both researchers in terms of having eligibility criteria, and in cases of disagreement, the opinion of the third party was considered as the final opinion.
Competence of Study
Inclusion criteria of the studies consisted of enrolling adult patients aged 18 years and older for suspected pneumonia. This was based on respiratory signs or symptoms or acute respiratory failure, and the assessment of pneumonia was based on a combination of clinical data, laboratory results, and chest imaging. The chest could have been imaged with a CXR or a chest CT. Articles that enrolled children with suspected chest pathology were excluded.21,22 Two researchers (B.S.H. and F.P.) independently reviewed all relevant studies, in terms of competence criteria, and performed integrated analysis. The data retrieved from these studies were compared by both researchers, and in cases of disagreement, the opinion of the third party was considered as the final one.
Methodological Qualitative Evaluation
Methodological quality was assessed using the QUADAS-2 (Quality Assessment of Diagnostic Accuracy Studies) criteria, which provide a standard approach for grading the quality of studies, for the purpose of a diagnostic accuracy meta-analysis. QUADAS-2 classifies the risk of bias and study generalizability as low, uncertain, or high. Both reviewers (B.S.H. and F.P.) rated the 7-item tool independently, and disagreements were resolved by consensus. These discussions required a face-to-face discussion on differences.
Biostatistics Methods
The main objective was estimation of integrated diagnostic accuracy measurements: integrated sensitivity and specificity using the Mantel-Haenszel method 23 and integrated positive likelihood ratio (PLR) and negative likelihood ratio (NLR) using the DerSimonian-Laird method. 8 It was also important to calculate a general area under the receiver operating characteristic (ROC) curve. Heterogeneity was calculated by the Cochran Q statistic and I2. An I2 >20% was considered as a sign of significant changes. In sensitivity analyses, a subgroup was evaluated to determine the stability of the findings. These statistical analyses were performed using Meta-DiSc 1.4 24 and R (www.r-project.org).
Results
Literature Search
A flow chart of the selection process trial is provided in Figure 1. The initial literature pull identified 663 studies by title and abstract screening, according to the search strategy. However, 264 were excluded as they were deemed not relevant to the analysis, leaving 84 articles for further evaluation. Eventually, 16 eligible studies involving a total of 2040 patients were included in the final analysis.
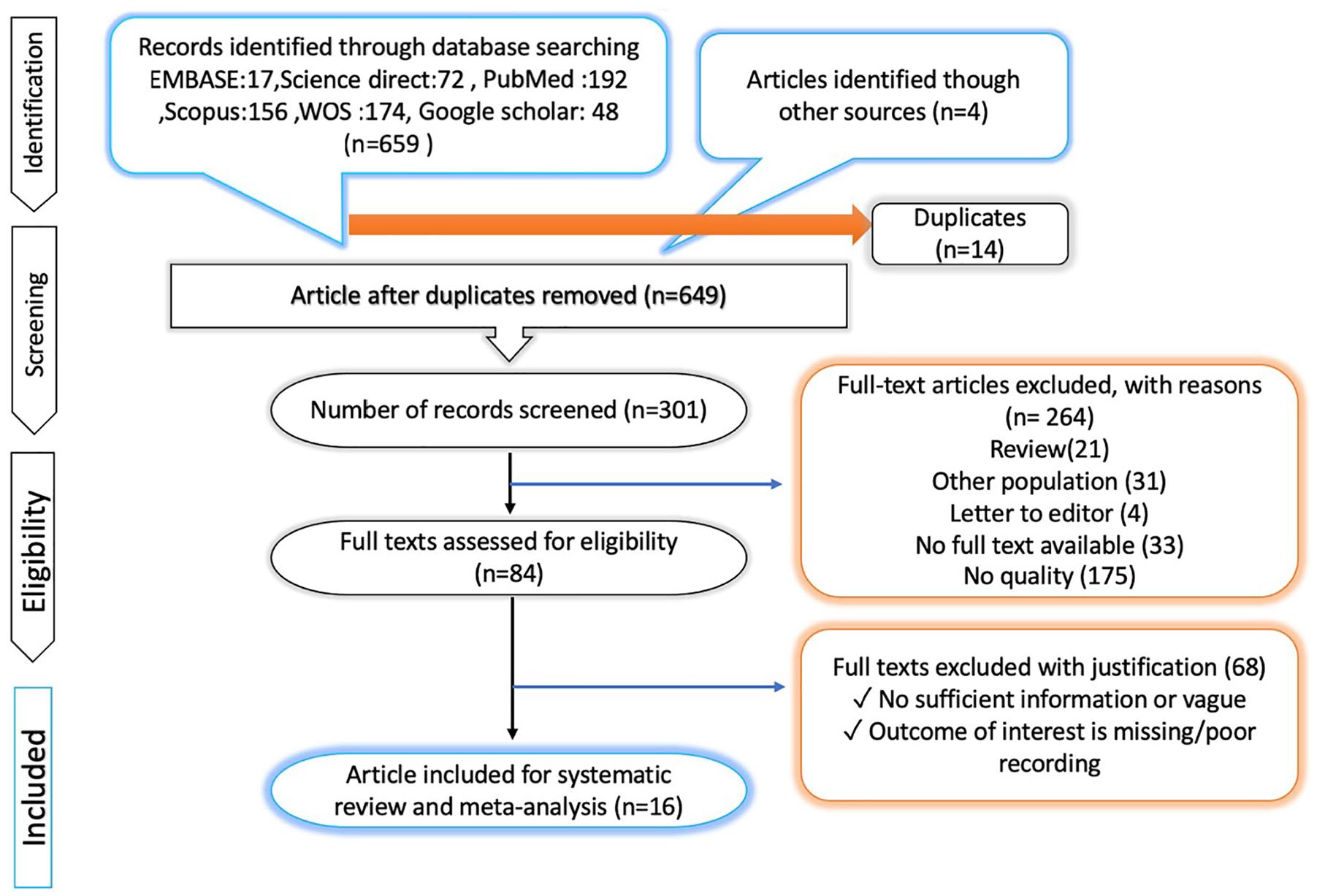
PRISMA flow diagram for the extraction of the publications for this systematic review. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; WOS, Web of Science.
Characteristics of Selected Studies
Among all 16 studies, 14 were carried out in an ED or on a hospital nursing unit10,15 –22,25,26 and 2 were conducted in an intensive care unit (ICU).14,27,28 Briefly, all studies were prospective and used a blinded research design. Five studies were performed in Italy, two in Turkey, two in Iran, and one study was conducted in Poland, France, China, Nepal, Kuwait, Egypt, and Greece, respectively. The mean age of included patients was 69.6 years, with 57% of patients identified as male. Regarding the diagnostic gold standard for diagnosing pneumonia, eight studies considered chest CT as the sole criteria, while the other eight studies used clinical presentations combined with imaging. Lung US was performed by experienced physicians in the ED or ICU, except for two studies where US was completed by radiologists 26 (see Tables 1 and 2). The details of the quality assessment are shown in Figure 3. The eligible studies achieved most of the quality items in QUADAS-2.
Characteristics of Those Studies Selected for the Meta-Analysis.

Note. Pros, prospective; Retro, restrospective.
Systematic Review of the Characteristics of the Imaging Techniques.

Abbreviations: Ant, anterior; AP, anteroposterior; CAP, community-acquired pneumonia; CT, computed tomography; CXR, chest radiograph; ED, emergency department; EP, emergency physician; ICU, intensive care unit; Lat, lateral; PA, posteroanterior; Pos, posterior; US, ultrasonography.
Statistical Outcomes
The overall diagnostic accuracy of lung US compared with CXR, for the diagnosis of pneumonia, was analyzed. Table 3 demonstrates the pooled sensitivity, specificity, Diagnostic Odds Ratio (DOR), PLR, NLR, and the summary receiver operative characteristics (SROC) curves for diagnostic performance of lung US and CXR to detect pneumonia. The overall pooled sensitivity of US and CXR, for the diagnosis of pneumonia, was 0.96 (95% confidence interval [CI], 94%–97%) and 0.65 (95% CI, 63%–68%), respectively. The overall pooled specificity for US and CXR for the diagnosis of pneumonia was 0.85 (95% CI, 84%–87%) and 0.81 (95% CI, 79%–83%), respectively (Figure 2). The overall pooled PLR was 9.74 (95% CI, 5.11–18.59) for US and 3.67 (95% CI, 2.35–5.75) for CXR. The overall pooled NLR was 0.052 (95% CI, 0.034–0.079) for US and 0.42 (95% CI, 0.34–0.53) for CXR. In addition, SROC areas under the curve (AUCs) were 0.9793 for US and 0.7667 for CXR (see Figures 4 and 5).
Diagnostic Performance of Lung US and CXR for Patients Suspected of Pneumonia.

Abbreviations: AUC, areas under the curve; CI, confidence interval; CXR, chest radiograph; DOR, diagnostic odds ratio; ED, emergency department; ICU, intensive care unit; NLR, negative likelihood ratio; NPV, negative predictive value; PLR, positive likelihood ratio; PPV, positive predictive value; SROC, summary receiver operative characteristics; US, ultrasonography.
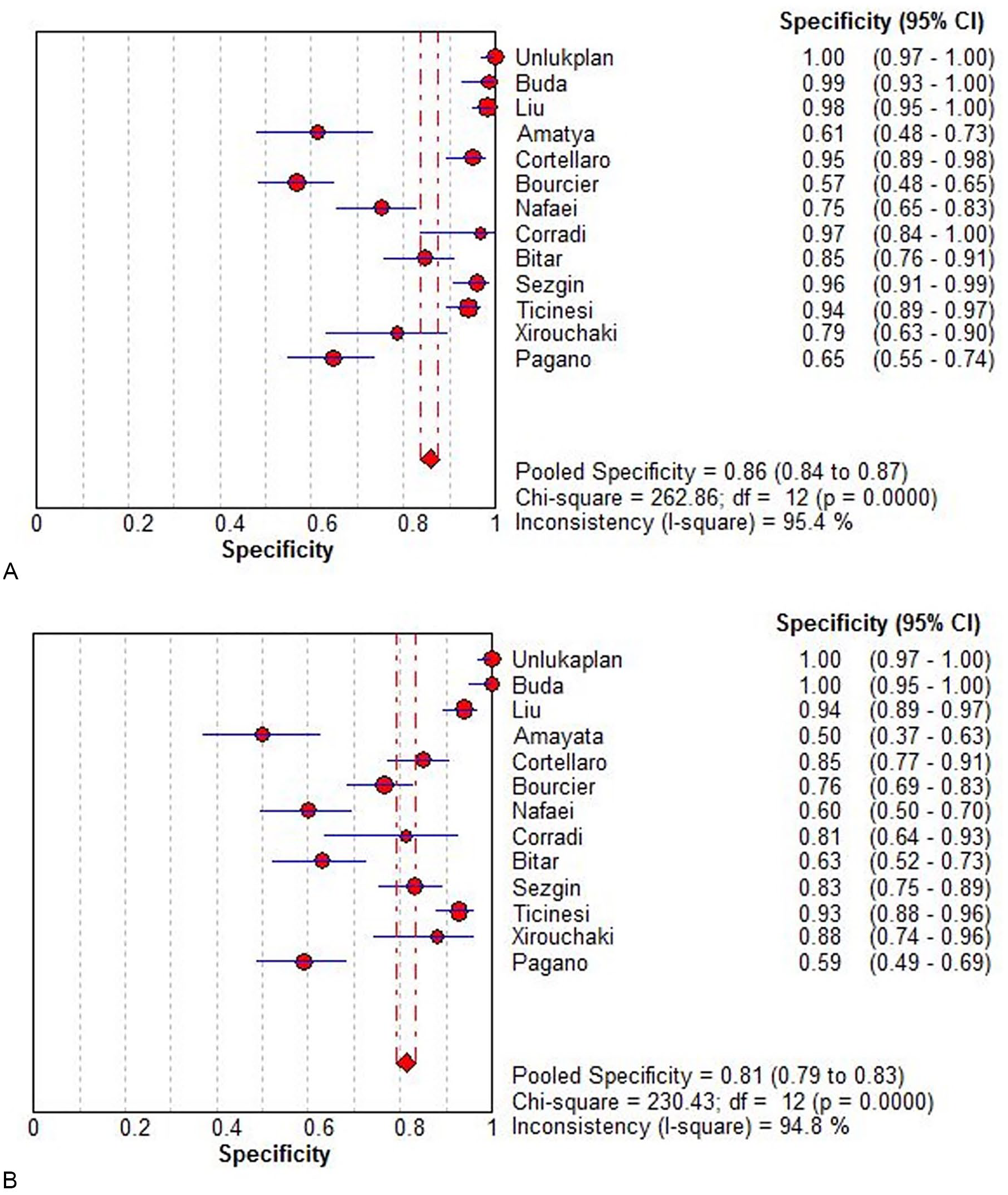
Specificity of lung US (A) and CXR (B) for patients suspected of pneumonia. CI, confidence interval; CXR, chest radiograph; US, ultrasonography.
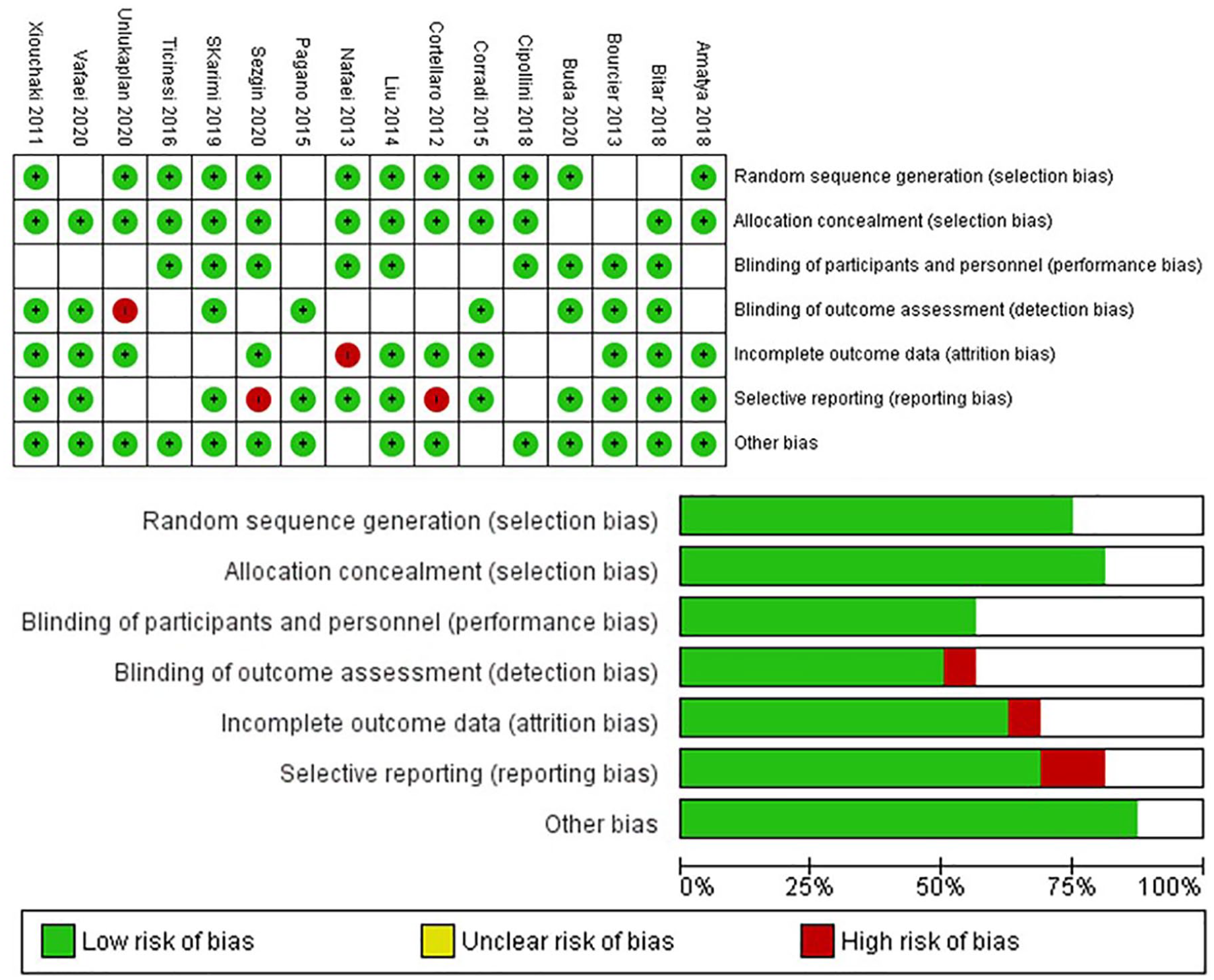
The risk of bias in the studies conducted was measured using QUADAS-2 tool. The risk of bias shown in Equation 2 of the above image model of each diagram indicates the number and percentage of studies with high (red), medium (yellow), and low (green) risk of bias in four groups of the QUADAS-2 tool. QUADAS, Quality Assessment of Diagnostic Accuracy Studies.
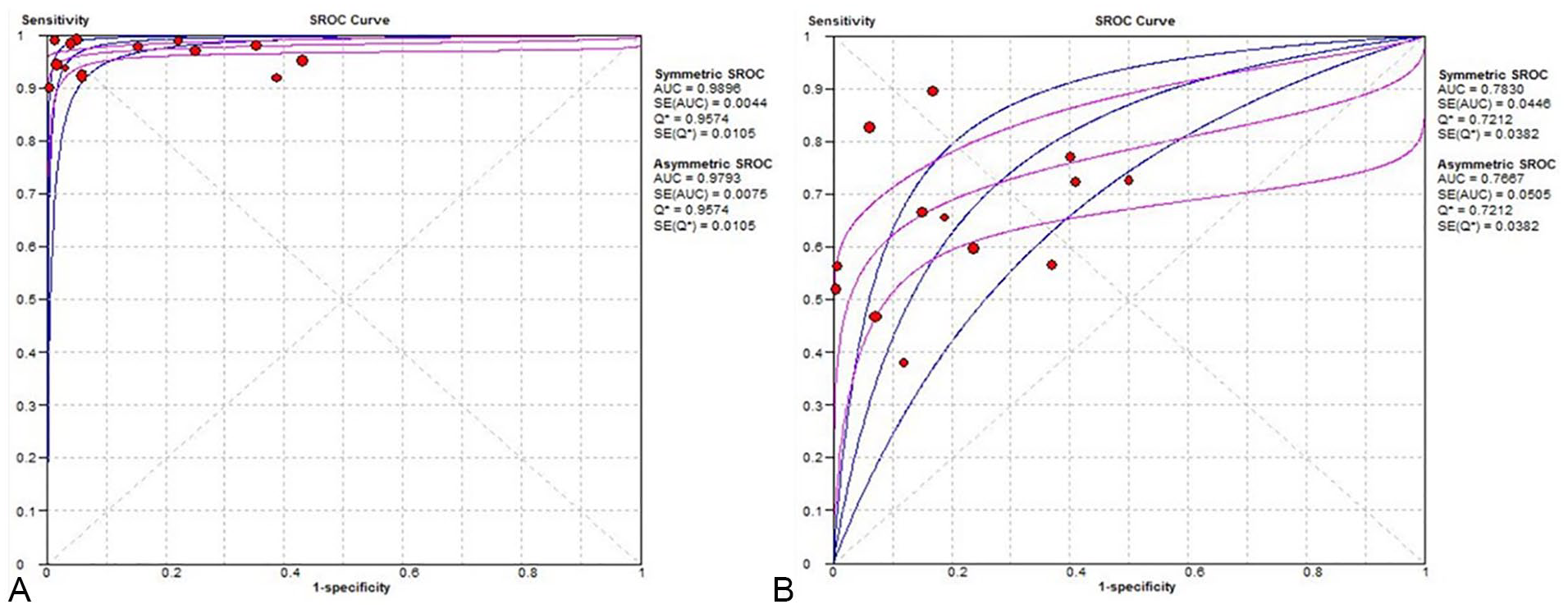
Summary receiver operative characteristics (SROC) curve of US (A) and CXR (B) in patients suspected of pneumonia. AUC, areas under the curve; CXR, chest radiograph; SE, standard error; US, ultrasonography.
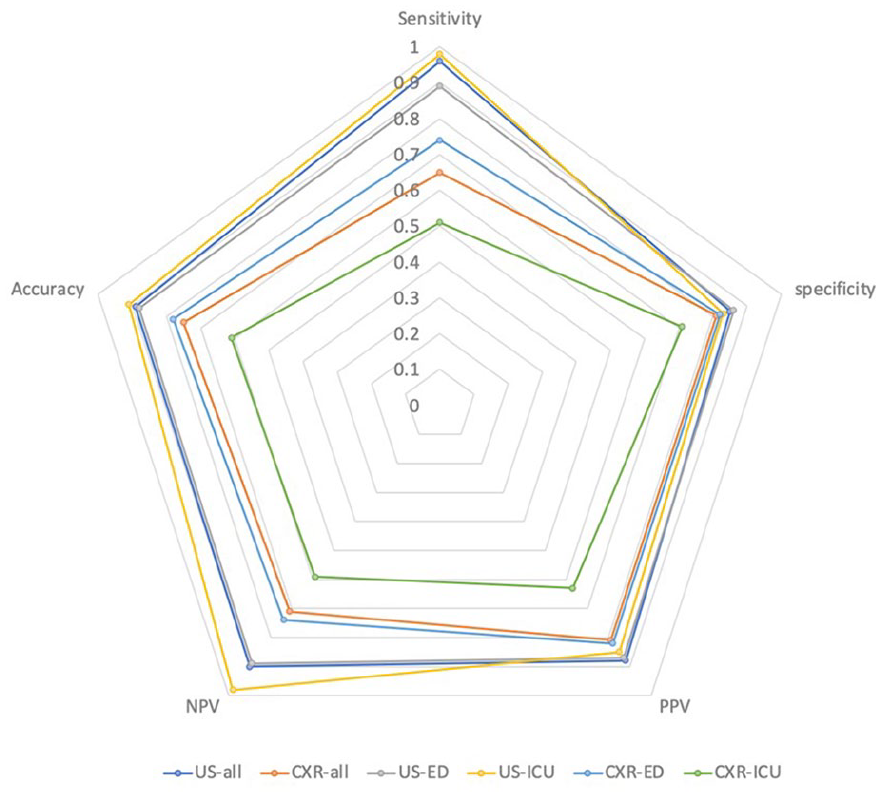
Radar chart of diagnostic performance of US and CXR in patients suspected of pneumonia. CXR, chest radiograph; ED, emergency department; ICU, intensive care unit; US, ultrasonography.
Subgroup Analysis by Lung US Versus CXR Performance
First, it was important to evaluate the accuracy of US and CXR for detecting pneumonia, based on three different hospital nursing units. For studies conducted in the ED (n = 12), the pooled sensitivity for US was 0.89 (95% CI, 87%–91%) compared with 0.74 (95% CI, 72%–77%) for CXR. The pooled specificity for US was 0.86 (95% CI, 83%–88%) compared with 0.82 (95% CI, 80%–84%) for CXR. In studies that evaluated critically ill patients, in the ICU (n = 2), the pooled sensitivity for US was 0.98/5 (95% CI, 95%–99%) compared with 0.51 (95% CI, 42%–59%) for CXR. The pooled specificity for US was 0.83 (95% CI, 75%–89%) compared with 0.71 (95% CI, 62%–78%) for CXR. One study evaluated elderly patients in a geriatric hospital (n = 1); the sensitivity for US was 72.2% (95% CI, 64.5%–79.0%) compared with 76% for CXR. The specificity for US was 86.0% (95% CI, 81.2%–90.0%) compared with 46% for CXR. In another study which was conducted in an internal medicine department (n = 1), the sensitivity of US was 72.2% (95% CI, 64.5%–79.0%) compared with 76% for CXR. In that same study, the specificity for US was 86.0% (95% CI, 81.2%–90.0%) compared with 46% for CXR (see Table 2).
Subgroup Analysis by Diagnosing Strategy and Study Origin
In the eight studies that used chest CT as the sole criteria, lung US exhibited a pooled sensitivity of 90.9% (95% CI, 87.5%–93.6%) and a pooled specificity of 89.7% (95% CI, 86.7%–92.3%). In studies (n = 8) that used the combination of chest imaging and clinical criteria as the gold standard, lung US revealed a pooled sensitivity of 95.0% (95% CI, 92.8%–96.6%) and a pooled specificity of 91.3% (95% CI, 87.9%–94.0%). The highest pooled sensitivity for lung US was reported in a Polish study, which was followed by four studies based in Italy and finally by two studies based in both Iran and Turkey, respectively. These studies conducted in Iran and Turkey reported the lowest sensitivity for US in the diagnosis of pneumonia (see Figure 6).
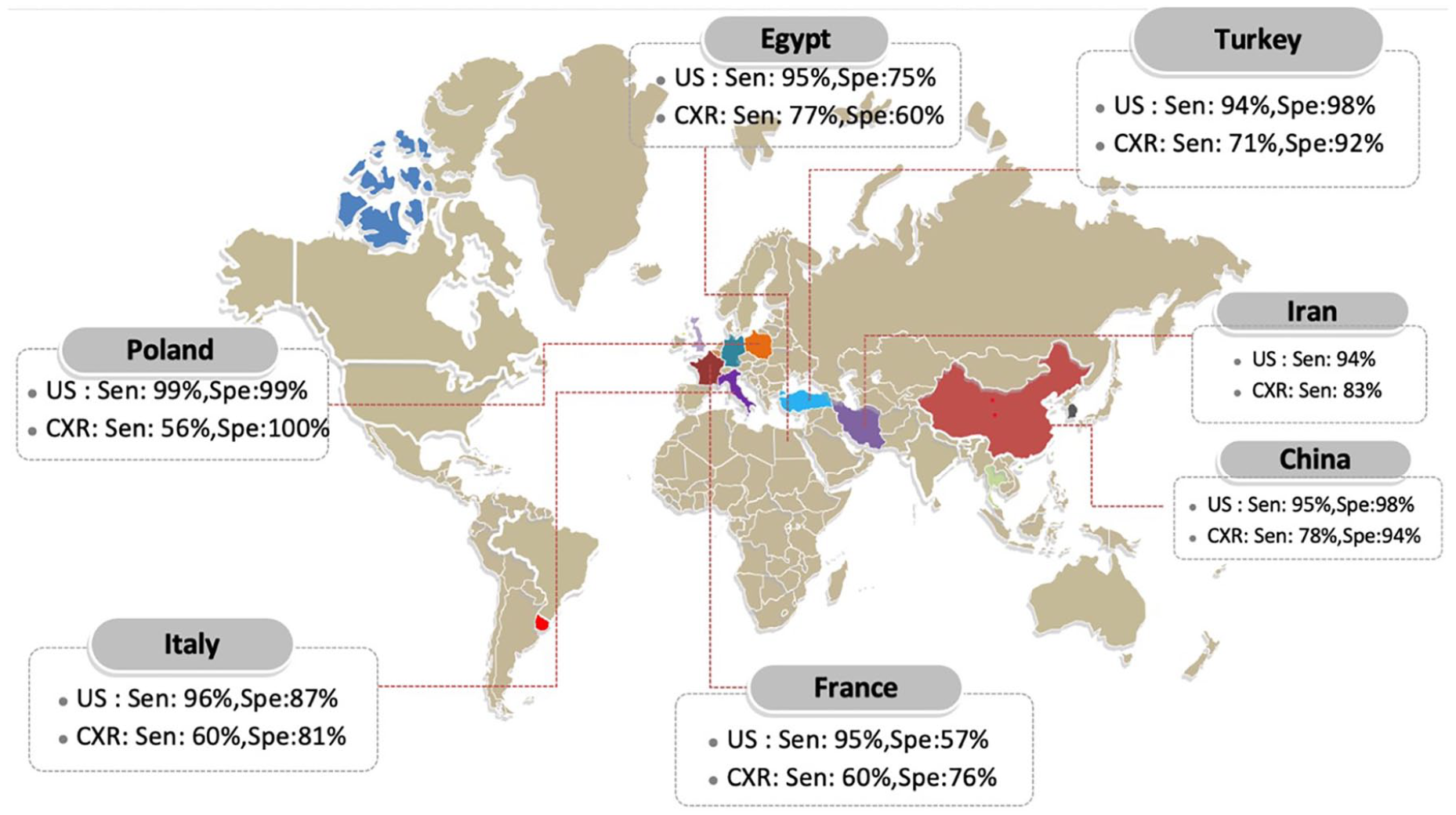
Sensitivity of lung US and CXR in diagnosing pneumonia based on country. CXR, chest radiograph; US, ultrasonography.
Discussion
Pneumonia is an acute lung disease including CAP, hospital-acquired pneumonia, and viral-acquired pneumonia (VAP). 1 It has been proved that lung US is a critical diagnostic instrument for intensive care physicians to detect pneumothorax, acute pneumonia, pleural effusions, and other lung diseases. 2 Using lung US is investigated for the diagnosis and follow-up of pneumonia in view of CXR limitations. 3 The diagnosis of pneumonia in adults needs further affirmation within radiology departments. Although it has been proved that a CXR has limited sensitivity, it can be regarded as a diagnostic choice when a physician needs to diagnose pneumonia. The lower detection rate with CXR, observed in this study, might be due to the inability to obtain a lateral CXR projection of the chest. The diagnostic limitations for a CXR are clear when it is performed to detect severe chest diseases, in an ICU or ED clinical unit. This may be due to the CXR procedure being performed in an open ambient environment and mostly with a x-ray equipment parked next to the bed. 4 In ED, it has been found that a bedside lung US is a reliable method for detecting lung densities, rather than with a CXR. Besides, it should be mentioned that the majority of the aforementioned studies use a binary reference standard (positive or negative). It should also be noted that the CXR results were commonly indeterminate for diagnosis. 5 Using CXR for diagnosing pneumonia may cause significant rates of misdiagnosis. The most common reason for choosing CXR as a diagnostic method is that it is widely available in a hospital setting. The CXR is a procedure that global medical personnel are trained to do and interpret the test. It is also important to underscore that a CXR is very cost-effective and the ionizing radiation is considered to be as low as reasonably achievable (ALARA). However, it has some very specific limitations, such as being time-consuming from exposure to providing the diagnostic report. There is also a high heterogenicity based on inter-rater and intra-rater reliability among radiologists, which can effect CXR reproducibity. 6 There is also a low diagnostic value for the CXR completed on a disabled patient. 8 Besides, the CXR can be dependent on the level of hydration, which is vital among the elderly and leads to a false-negative CXR result in the acute phase of the disease. The chest CT minimizes the risk of misdiagnosis when matched to the patient’s CXR. Hence, it can be regarded as an ideal standard to diagnose inflammatory lung injuries. 7 Despite this, chest CT is not used routinely for the diagnosis of pneumonia due to the higher rate of radiation, higher costs and the additional examination time, need for experienced CT personnel, and methods for patient transportation, which are extremely problematic for disabled patients. In this meta-analysis, it has been found that compared with chest radiography, lung US has a sensitivity of 88% and specificity of 86%, in the adult diagnosis of pneumonia. Bourcier et al 9 confirmed a high diagnostic value for lung US in detecting pneumonia. This study also demonstrated a very high sensitivity for lung US, in the diagnosis of acute pneumonia, compared with chest radiography (95% vs 60%, P > .01). The DOR is the PLR ratio to NLR; the higher the DOR, the higher the accuracy of this method for the diagnosis of pneumonia. In this study, the DOR was estimated as an indicator for test precision based on sensitivity and specificity. 41 The AUC was obtained at 0.95, which shows the high precision of lung US. In this meta-analysis, the average DOR was equal to 65.46 (95% CI, 29.24–146.56), which shows the significant accuracy of this method. However, LRs are more significant clinically. Integrated PLR at 5.37 shows that patients with pneumonia have five to six times higher chance for positive lung US compared with patients without pneumonia. On the contrary, the integrated NLR at 0.013 shows that if a lung US is negative, the probability of pneumonia is about 13% (Figure 7). A meta-analysis implemented by Chavez et al 23 investigated the clinical symptoms, laboratory results, and CXR, with a CXR or a chest CT as the diagnosis criterion. They reported a clear advantage for lung US over standard radiography in diagnosing pneumonia, based on a PLR, NLR, and AUC, respectively, at 16.8 (95% CI, 7.7–37.0), 0.07 (95% CI, 0.05–0.10), and 0.98 (95% CI, 0.98–0.99). The present meta-analysis has some limitations. First, the study ignored the papers not published in peer-reviewed journals. It is also important to underscore that the number of included studies was limited. However, this may be compensated by the intermediate to large number of patients (N = 2040), included in the analysis. In addition, the majority of global cases and complications of pneumonia were easily defined. Finally, not all of the included studies examined the entire lung area. As some patients were hospitalized, it was hard to examine the posterior chest lobes.

Fagan’s nomogram for the calculation of posttest probabilities. A pretest probability of 50% for all three diagnostic tools was fixed, which was estimated by the number of symptomatic cases in selected studies. (A) US-all had a posttest probability of 80.8%. (B) For US-ED, the posttest probability was 80.8%.(C) For US-ICU, the posttest probability was 80.8%. (If this patient tests positive, the posttest probability that she truly has pneumonia would be (A) 30.1%, (B) 14.4%, or 34% (C) [solid line in red]). ED, emergency department; ICU, intensive care unit; US, ultrasonography.
Conclusion
This study demonstrated that lung US is a useful diagnostic technique for the diagnosis of pneumonia. This method has many advantages, which can be used by ED physicians with high accuracy, sensitivity, and specificity. The solution enables a fast evaluation of unstable patients, without using ionizing radiation. Among the elderly population, this diagnostic method has the potential to produce better results than a CXR for pneumonia. The quick performance of a lung US may facilitate the rapid, cost-effective, and safe diagnosis of pneumonia which can be a fatal disease. Hence, the use of lung US has the opportunity to expedite a patient’s treatment and prognosis for those affected with pneumonia.
Footnotes
Ethics Approval
There was no need for ethical approval as this study was a systematic review and meta-analysis.
Informed Consent
There was no need for informed consent as this study was a systematic review and meta-analysis.
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because the study did not include any animal participants directly.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Trial Registration
Trial registration was not applied due to study type.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.