
Abstract
Plain radiography is often considered a first-line diagnostic tool and gold standard for bony fractures. This case series and brief literature review highlight the need for increased training in musculoskeletal sonography. A case is presented of a distal radial fracture that was not detected on radiography but diagnosed with sonography on the same day. Similarly, two fractures of the distal fibula were diagnosed using sonography after negative radiographs at follow-up appointments, led to misdiagnoses and mismanagement. A fourth case is presented to show an acute rib fracture diagnosed by sonography. These cases emphasize the importance of musculoskeletal sonography training in the diagnosis of acute fractures and its underutilization at the bedside. Collaboration between sonographers and physicians may increase utilization of musculoskeletal sonography which in turn may improve patient care and outcomes.
Musculoskeletal complaints account for 20% of emergency department and primary care visits in the United States. 1 Over the years, several studies have demonstrated the increased utilization of diagnostic musculoskeletal sonography in the detection of acute fractures with high accuracy, but unfortunately musculoskeletal sonography is still underutilized in clinical settings.1–5 There continues to be growing evidence for the use of musculoskeletal sonography in the diagnosis and management of acute fractures and even stress fractures. The best evidence supports its use in the lower extremities where these fractures are commonly missed.5–10 Bedside musculoskeletal sonography is relatively still new to the physician community and the sonologist may be best suited to help fill in these gaps in urgent and emergent clinical settings.3,11,12 As musculoskeletal sonography is increasingly being requested by both patients and physicians, having a lead radiologist(s) or other physician specialty to help pioneer and develop this service may be key in the multidisciplinary approach needed for interdepartmental cross-training and communication. 13
Case Reports
Distal Fibular Fracture
A 45-year-old woman presented to the sports medicine clinic for follow-up after a right ankle sprain was diagnosed in the emergency room of a community hospital four days prior. At the time, she had negative radiographs (Figure 1), was given an air cast and crutches, and advised to weight-bear as tolerated.
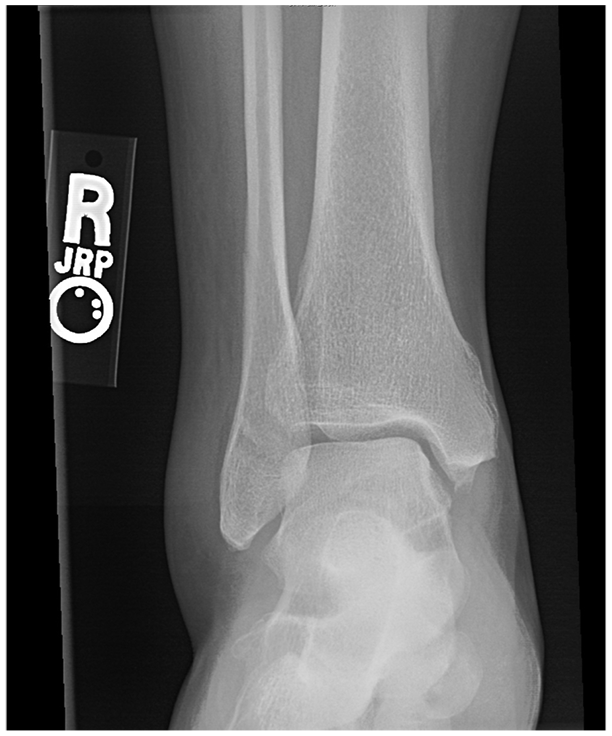
Anteroposterior radiographic view of the right ankle. No fracture reported on the official radiologist report.
On presentation, the patient complained of worsening lateral right ankle pain after her injury from sleepwalking and waking up against her door jamb. She had persistent, sharp, right lateral ankle pain with swelling and bruising that was aggravated with ambulation. Three-view plain radiographs done in the emergency department reported no fracture and a right ankle sprain. On examination, range of motion (ROM) of the right ankle was limited secondary to pain. She had point tenderness overlying the right lateral malleolus. Pulses, strength, and sensation were intact. There was significant edema and ecchymosis.
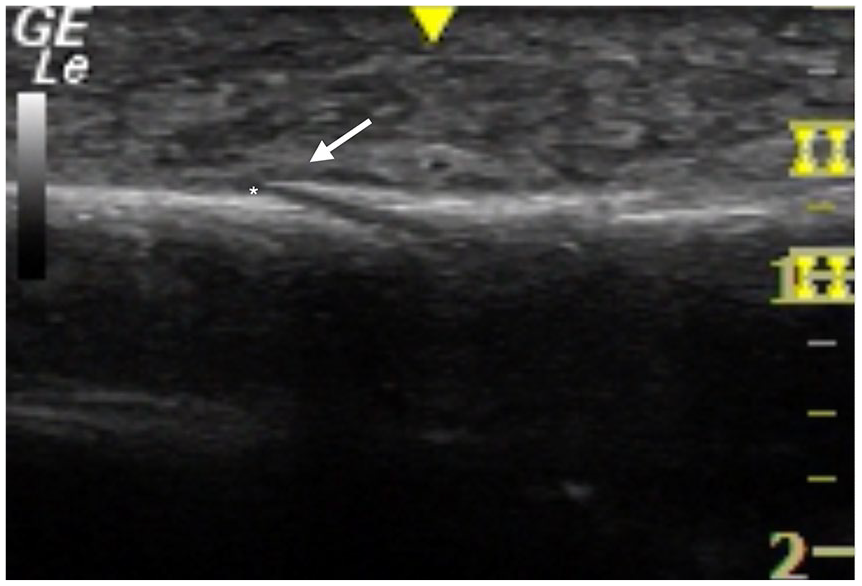
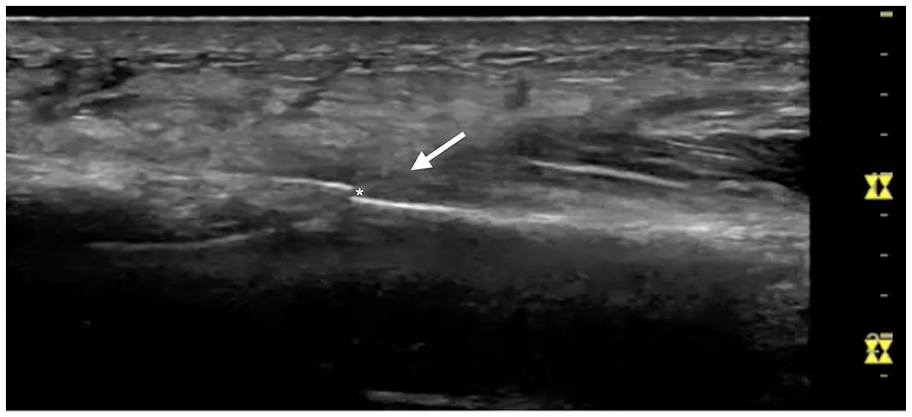
Sonography was performed using a GE Logiq S7 and ML6-15 linear probe. The right ankle was evaluated in both longitudinal and transverse views. Examination of the right lateral ankle showed a cortical step-off at 5 cm proximal to the lateral malleolus in transverse view (Figure 2). On longitudinal view, a cortical step-off, a small hematoma, and subcutaneous edema of the distal fibula were detected (Figure 3). The patient was significantly tender to sono-palpation at this sight, confirming the location of her pathology.
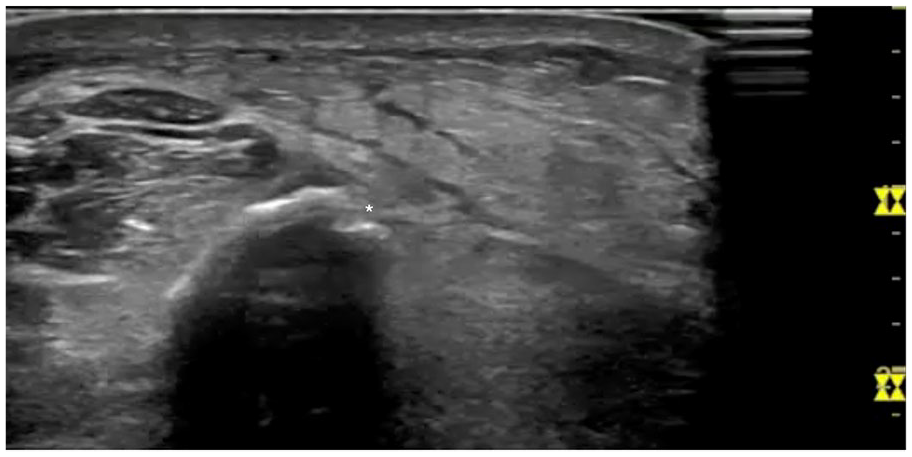
Short axis image of lateral malleolus showing a cortical step-off (asterisk). Maximal tenderness to sono-palpation was noted in this area.
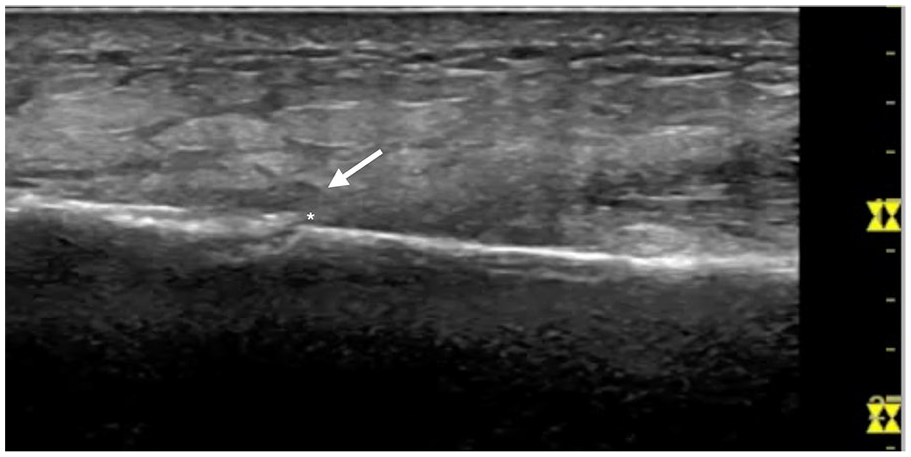
Longitudinal axis view of the lateral malleolus showing a cortical step-off (asterisk), a small hematoma (white arrow), and subcutaneous edema.
This patient was given a non-weight-bearing (NWB) boot and crutches. She was prescribed nonsteroidal anti-inflammatory drugs (NSAIDs) for management of pain and inflammation. On 2-week follow-up, the patient eliminate had expressed improvement in her pain and swelling. Repeat radiographs at the time revealed a minimally displaced oblique fracture of the right distal fibula (Figure 4). During her 6-week follow-up, the patient’s ankle pain was nearly resolved, with minimal tenderness to palpation over the distal fibula. The patient was recommended ambulation with a short walking boot without crutches and ROM exercises at home and referred to physical therapy. One month later, she had resolution of all pain and near complete return of her ROM.
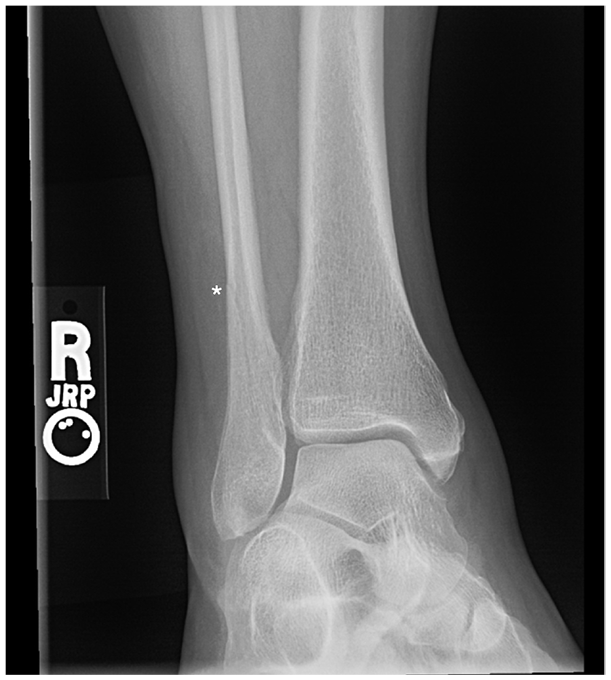
Repeat anteroposterior radiographic view of the right ankle over 2 weeks after initial injury revealing an oblique fracture (asterisk) of the right distal fibula.
Distal Fibular Fracture
A 70-year-old woman presented to a sports medicine clinic who complained of severe right ankle pain after being seen in the emergency room at a community hospital three days prior after rolling her ankle off a curb. Radiographs were done in the emergency room and demonstrated no acute fracture (Figure 5). She was diagnosed with a lateral right ankle sprain and sent home with an ACE wrap, no crutches, and told to take Tylenol over the counter.

Anteroposterior radiographic view of the right ankle. No fracture was reported on the radiologist’s official report.
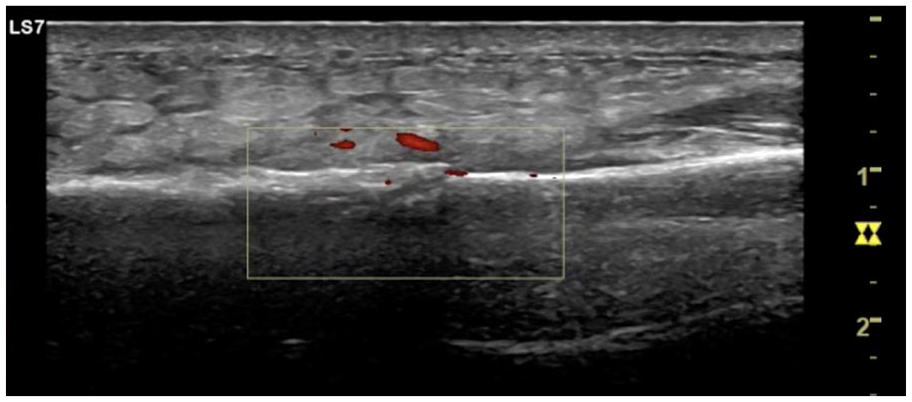
On physical examination, the patient had point tenderness to the lateral malleolus of the right ankle with mild overlying edema. ROM was limited due to pain, but pulses and sensation were intact. Sonography was performed using a GE Logiq e9 and 12L-SC linear probe. The right ankle was evaluated in both longitudinal and transverse views. Examination of the right lateral ankle showed a cortical step-off at 1 cm proximal to the lateral malleolus in long-axis view (Figure 6). On transverse view, a cortical step-off and small hematoma was also noted in the same region. Using power Doppler, hyperemia was confirmed at fracture sight and within the cortex (Figure 7). The patient was also tender to sono-palpation at this sight, confirming the location of her pathology.
Longitudinal axis view of the lateral malleolus showing a cortical step-off (asterisk), a small hematoma (white arrow), and subcutaneous edema.
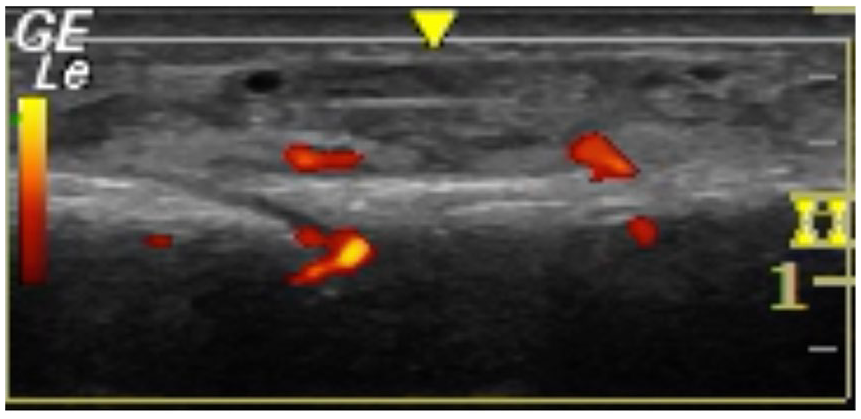
Power Doppler in longitudinal axis view of the lateral malleolus showing hyperemia at the location of the hematoma and within the cortex.
This patient was not able to tolerate a boot, so she was casted, given crutches and a temporary handicap parking pass for six weeks. She was prescribed NSAIDs for pain management and advised to follow-up in 2 weeks. On follow-up, radiographs confirmed and revealed a nondisplaced right distal fibular fracture. At her four-week follow-up, her ankle pain was much improved, and she was able to tolerate a short walking boot without crutches. She was later referred to physical therapy and returned to normal activity in eight weeks.
Distal Radial Fracture
An 81-year-old woman presented to the family medicine clinic with right forearm pain that began after a heavy suitcase fell on her lateral right forearm. On examination, her pain was located on the radial aspect of her distal right forearm. She did not have any overlying edema or ecchymosis and no wrist or hand weakness was noted. Pulses, sensation, and strength were intact in the right arm, wrist, and hand. Anteroposterior and lateral right forearm radiographs were obtained, which showed soft tissue edema but no acute fracture of the radius and ulna (Figure 8).

Oblique radiograph of the right wrist. No fracture was reported on the radiologist’s official report.
Considering this patient’s significant point tenderness on examination, sonography was performed using a GE Logiq S7 and ML6-15 linear probe. Longitudinal and transverse views were used to detect a cortical step-off deformity of the distal right radius, a small hematoma, and subcutaneous edema (Figure 9). The fracture site also demonstrated increased hyperemia with power Doppler (Figure 10). The patient was appropriately tender to sono-palpation at the site of her cortical irregularity. A radial gutter splint was placed with the wrist in slight extension. The patient was advised to take Tylenol for pain relief and elevate the arm to avoid swelling. On two-week follow-up, the patient reported improved right forearm pain. She continued to have tenderness to palpation overlying the lateral distal right radius. Repeat radiographs showed an acute minimally displaced, oblique, intra-articular fracture of the lateral distal right radius (Figure 11). The patient continued with a radial gutter splint, elevation, and pain management for 2 weeks and was transitioned to a wrist brace thereafter and did well at her 6-week follow-up appointment.
Long-axis view of the distal radius showing a cortical step-off (asterisk), a small hematoma (white arrow), and subcutaneous edema. Maximal tenderness to sono-palpation was noted in this area.
Power Doppler in longitudinal axis view of the right distal radius showing hyperemia at the location of the hematoma and in the area of the cortical step-off.

Repeat oblique radiographic view of the right wrist showing a minimally displaced, oblique, intra-articular fracture (asterisk).
Rib Fracture
A 58-year-old man presented to the sports medicine clinic for complaints of right-sided flank/chest wall pain. Two weeks prior, his side landed on a joist after a fall while repairing his deck. He went to the emergency room where radiographs of his chest and shoulder were negative for fracture (Figure 12). His pain continued to be exacerbated by movement and deep breathing and noted significant rib bruising. On physical examination, the patient had ecchymosis and tenderness to palpation along the right chest wall, without obvious deformity. Based on the clinical history and examination, the top differential diagnosis was a fractured rib. Given the known data on the superiority of sonography in comparison with radiographs in the detection of rib fractures, the decision was made to proceed with sonography, rather than a radiograph.7,11
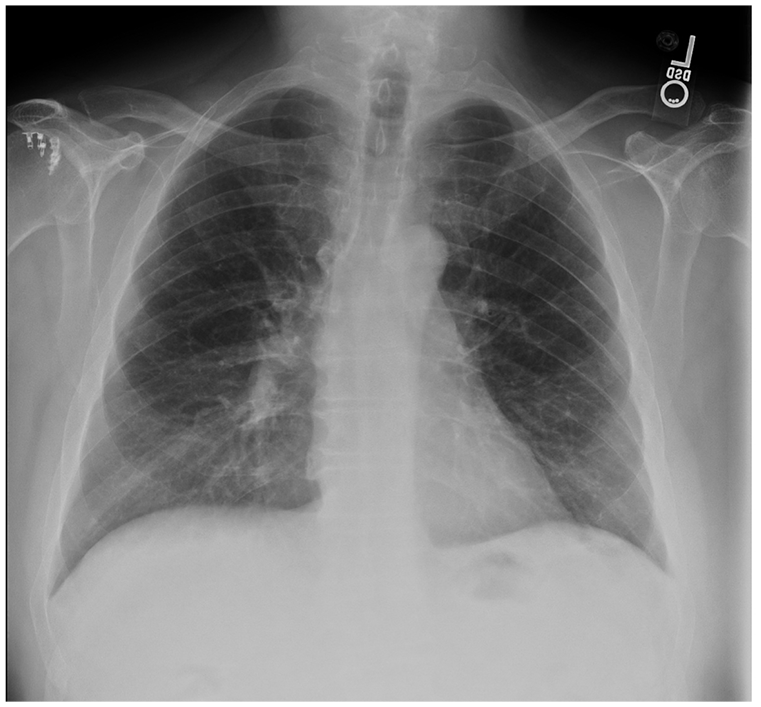
Posteroanterior chest radiography. There were no rib fractures reported by the radiologist on the official report.
Sonography was performed using a GE Logiq e9 and 12L-SC linear probe. The right 7th and 8th ribs were tender to sono-palpation and further evaluated in both longitudinal and transverse views. Examination of the right 7th and 8th ribs revealed cortical discontinuity and a collagen capsule (Figure 13). This was also seen on transverse view where their pain was reproducible on sono-palpation.
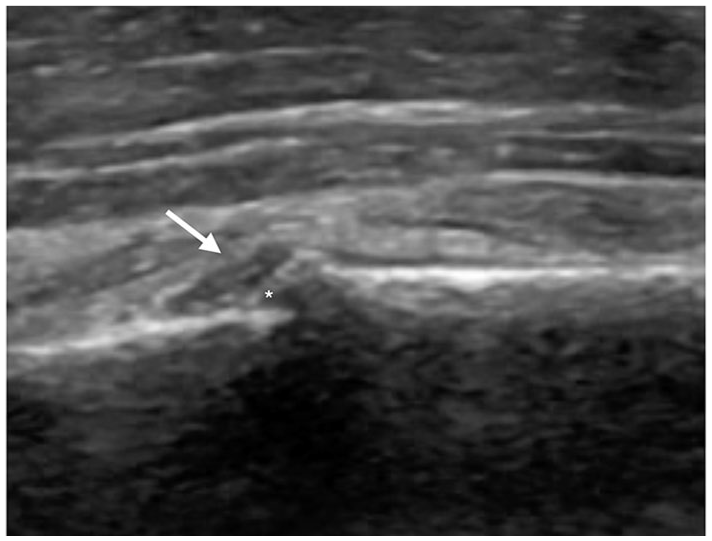
Long-axis view of the 7th ribs showing cortical discontinuity (asterisk) and a collagen capsule (white arrow). Maximal tenderness to sono-palpation was noted in this area.
This patient was reassured that imaging or intervention was not indicated at this time. The patient was given work accommodations for light duty and advised to take NSAIDs for pain management and did well. Three months later, the patient went to the emergency room for chest pain and a computed tomography (CT) of his chest confirmed numerous right-sided healing, subacute fractures (Figure 14).
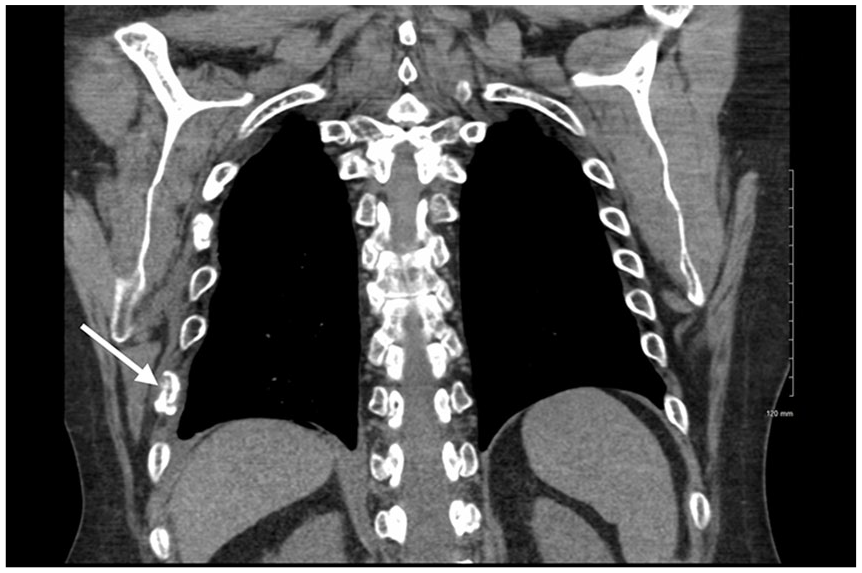
Coronal view of rib fracture (white arrow).
Discussion
These cases illustrate the successful diagnosis of acute fractures using musculoskeletal sonography. In these specific cases, sonography demonstrated superior accuracy to plain radiographs in detecting acute fractures and these findings are consistent with the literature.1,2,5-11,14-16,22 Although the literature has become more clear of the benefits and superiority of sonography over radiographs in the detection of fractures, there continues to be a gap in its utilization to optimize patient outcomes and the implementation of, within clinical practice.1,17 Up to 30.6% of all musculoskeletal diagnoses made using magnetic resonance imaging (MRI) could be diagnosed using musculoskeletal sonography.1,18
Although point-of-care sonography has been shown to decrease the length of time to diagnosis and discharge and decrease failure rates to treatment, radiographs continue to be the first-line diagnostic tool in evaluating patients with acute upper or lower limb injuries. 19 In many cases, CT or MRI continues to be ordered if there is still a high index of suspicion for fracture with negative radiographs. Not only is this costly, but it involves exposure to excessive amounts of radiation and increases cost and utilization of health care resources.
Systematic reviews have shown that extremity fractures can be detected on a sonogram with sensitivities and specificities up to 93% and 92% respectively, for upper limb fractures and 83% and 93% respectively, for lower limb fractures.5,6 A sonogram to detect rib fractures has also been shown to be superior to radiography. The data have shown that physical examinations, radiographs, and sometimes even CT can detect only about half of rib fractures. One study found the sensitivity of sonography in detecting rib fractures to be 98.3% in comparison with 40.7% to 45.8% with chest radiography. 6 In contrast to upper and lower extremity musculoskeletal sonograms, when performing sonography of the ribs, it is important to be mindful of their anatomical positioning. Ribs slant caudally at an angle when extending from posterior to anterior. A linear transducer should be used in both in-plane and out-of-plane alignments along the long axis of the ribs, which is a similar technique used when evaluating upper and lower extremity fractures. 11 While a chest radiograph is beneficial in evaluating a patient with chest wall pain, sonography could be considered a better tool to rule out acute rib fractures as well. 11
If a sonologist could have performed a musculoskeletal sonogram, in the emergency room or at the bedside, on initial presentation of these case-series patients, these fractures may not have been missed. In addition, these patients could have received more appropriate diagnoses and treatment. Another possible scenario would be that the initial evaluating physician could have used point-of-care musculoskeletal sonography in the early detection of these acute fractures. Unfortunately, training and experience in sonography for physicians have been relatively newly implemented. Compared with sonography organizations like the Society of Diagnostic Medical Sonography, founded in 1970, the American College of Emergency Physicians established their Emergency Ultrasound section in 1995, and at that time only ten emergency physicians in the country were practicing point-of-care sonography. 12 Even within other primary care specialties, family medicine, for example, physicians have been using point-of-care sonography for decades, but it was not until 2016 that the American Academy of Family Physicians Congress of Delegates adopted a resolution to increase point-of-care sonography into Family Medicine education. 3 Although there are some sports medicine physicians who are being trained in diagnostic musculoskeletal sonography, many are electing to focus more on ultrasound-guided procedures.
Although the evidence is clear that there are cases when musculoskeletal sonography is superior to radiography, these cases highlight its continued underutilization and slow widespread adoption which may also be due to lack of subspecialty expertise or adequately trained personnel. 1 Sonologists may be best suited to potentially help fill this gap by collaborating with physicians of various medical specialties with helping establish sonography electives and hands-on practical assessments for physicians in training.13,20 A general opinion along with others practicing point-of-care sonography is that this tool has increased the appreciation for sonographers and their unique skill set, which cannot be replaced. 20 This is especially true when physicians are tasked to evaluate and treat more than 20 to 30 patients a day and there is not enough time to perform a complete ultrasound study. Point-of-care sonography has also allowed physicians to order the appropriate imaging study needed for a patient more often, 19 which many times can be a formal sonographic study. Point-of-care sonography adoption has grown rapidly and even more so in the era of COVID-19, as its utilization has gained the support of both cardiologist and radiologist. 21
Missed or delayed diagnoses in fractures can result in poor bone healing, longer duration of pain, poorer prognosis, decreases in quality of life, as well as the long-term impact on patient mobility. Complications of delayed diagnosis of fractures include bony nonunion, avascular necrosis, secondary osteoarthritis, and neurovascular injury. Thus, early diagnosis and intervention is essential to achieve optimum recovery with minimal complications. With a conservative approach, a nondisplaced fracture can be suspected in a symptomatic patient with the appropriate clinical findings and mechanism of injury, despite negative radiographs, but definitive diagnosis will lead to faster recovery times and appropriate treatment. Pediatric and elderly populations are also at highest risk of fractures and increased complications of missed diagnoses.8,15,16 Complications involved in elderly fractures can even lead to increased mortality and functional decline, leading to a loss of independence.8,23 Based on these risk factors and cases highlighted, it is crucial to reach early diagnosis in patients in the management of fractures, despite having negative radiographs, not only to inform the patient, but also to affect the management plan going forward for the best possible outcome.
Conclusion
Acute fractures are most often diagnosed through the use of radiography. Although the adoption of musculoskeletal sonography continues to increase, there continues to be a gap in its utilization and adoption. Radiography is still considered the gold standard in the detection of bony fractures and these fractures continue to be missed which lead to decreases in quality of life for patients. The use of musculoskeletal sonography can be used in the acute-care setting to diagnose fractures, but at this time there is a void in medical personnel to perform these examinations. Increasing the collaboration and training between sonographers and physicians, in diagnostic musculoskeletal sonography, may address the unique needs of their community. It may also foster an increase in the availability of sonography to more rapidly and appropriately diagnose and manage patients with fractures. This nonionizing diagnostic tool could be a low-cost, high-yield solution for health systems that already have skilled sonographers. A collaborative effort from sonologists, physicians in training, and attending physicians may be needed to fill in these gaps.
Footnotes
Ethics Approval/Informed Consent
Ethics approval and informed consent was not needed as no vunerable patient populations were included, no patient information was collected and images were deidentified. In addition for all procedures in our academic clinic all patients are required to sign consent to photography and videotaping of all or any part of their treatment/procedure for medical and/or educational purposes with the understanding that their identity will not be revealed in any photographs or videos.
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because no animals were involved.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Trial registration
No intervention done with these case reports and this was not a clinical trial.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.