
Abstract
Although polyp size and stalk diameter are significant for the differential diagnosis of a gallbladder polyp, it is necessary to catch genuine polyp characteristics to differentiate a giant fibrous polyp from gallbladder carcinoma (GBC). This case report analyses the images and their correlation with the pathology. Transabdominal sonography revealed gallstones and a giant pedunculated gallbladder polyp measuring 32 × 18 × 14 mm with a thick stalk. The polyp lacked a hyperechoic surface line and was not delineated by either a deep hypoechoic area or a conically thickened outermost hyperechoic layer. Contrast-enhanced ultrasonography (CEUS) depicted a periphery-dominant enhancement, during the post vascular phase. A noncontrast computed tomogram (CT) did not demonstrate a gallbladder mass; meanwhile, a dynamic study revealed an enhanced polyp showing a periphery-dominant enhancement. Hence, without diagnostic findings suggestive of an obvious advanced GBC or excluding an early GBC, a full-thickness laparoscopic cholecystectomy was performed. The histopathology demonstrated a fibrous polyp with a thick stalk. In conclusion, a giant gallbladder polyp with a thick stalk showing a periphery-dominant contrast enhancement could suggest a fibrous polyp.
A fibrous polyp, of the gallbladder, is an unusual benign condition indicating a pedunculated or semi-pedunculated construction. Recently, clinicians had the experience of imaging a giant fibrous polyp that was more than 3 cm in diameter. In the case of a large fibrous polyp, it is difficult to differentiate it from a gallbladder carcinoma (GBC) 1 even through the process of evaluating the polyp size and stalk diameter. For that reason, these clinicians considered it necessary to determine genuine gallbladder polyp characteristics. The clinicians were interested in determining whether a polyp’s diagnostic findings could be suggestive of a giant fibrous polyp; therefore, they conducted a literature search. This case report reviews and analyses the images and how they correlated with the pathology.
Case Report
An 82-year-old woman presented to the hospital due to her nausea and vomiting. The patient’s laboratory results indicated no abnormalities, which included values for carcinoembryonic antigen and carbohydrate antigen 19-9.
A transabdominal sonogram was performed using a Toshiba SSA-770A ultrasound equipment system and a 5.0 MHz convex transducer (Toshiba, Tokyo, Japan). The sonographic study depicted gallstones and a giant pedunculated gallbladder polyp measuring 32 × 18 × 14 mm, with a thick stalk. The polyp was not delineated by either a hyperechoic surface line, a deep hypoechoic area, or a conically thickened outermost hyperechoic layer (see Figure 1A). A color Doppler sonogram (Superb microvascular imaging) showed a dendritic vascular signal (see Figure 1B). Contrast-enhanced ultrasonography (CEUS) was conducted with a rapid intravascular 0.5 mL dose of Sonazoid and this depicted a dendritic enhancement, during the early vascular phase. It also showed a periphery-dominant enhancement during the post vascular phase (see Figure 1C, D).
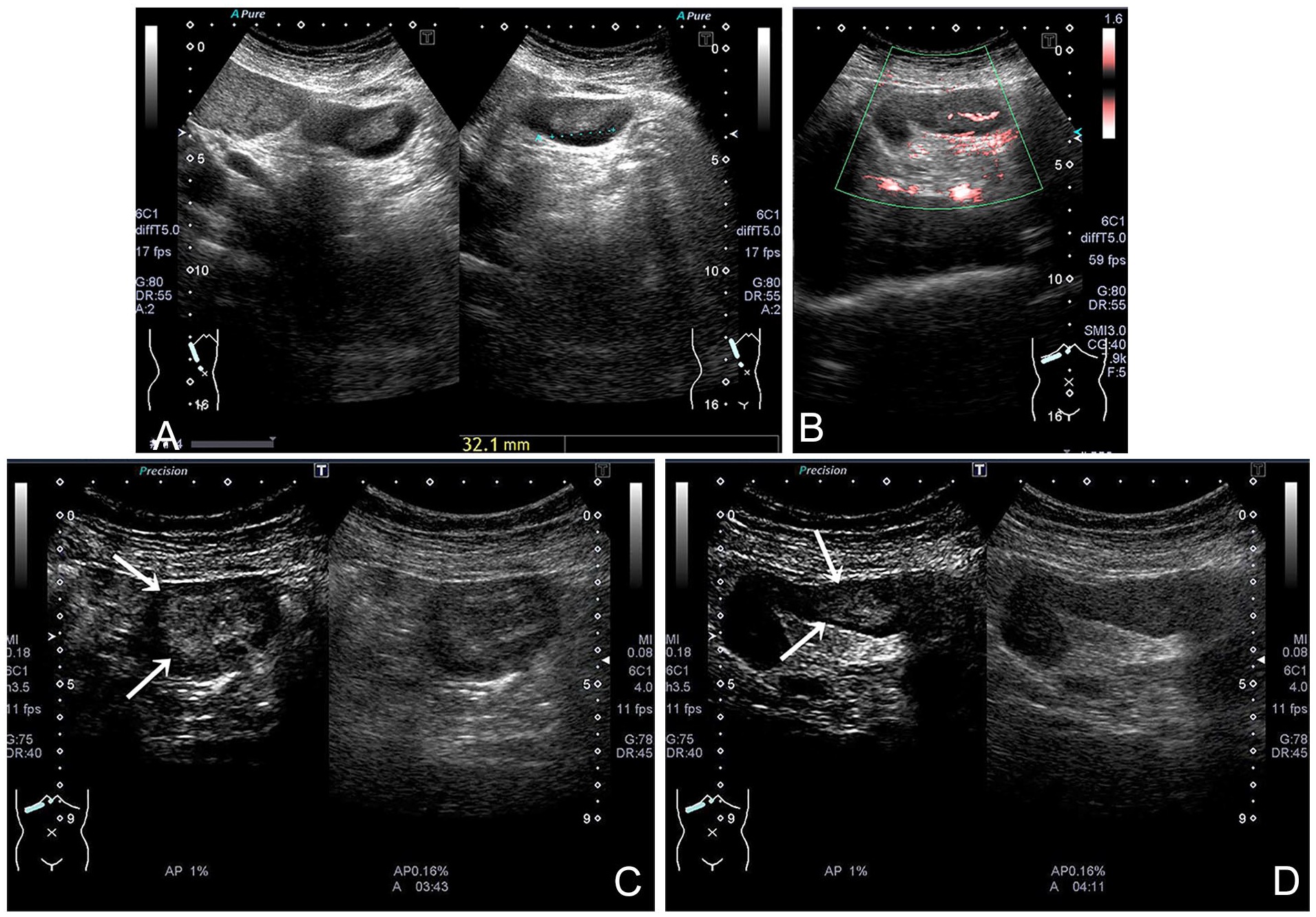
(A) A transabdominal sonogram is provided and demonstrates a gallbladder polyp measuring 32 × 18 × 14 mm with a thick stalk, 5 to 6 mm in diameter, in the fundus. The contour is regular, and the internal echo is almost homogeneous. The polyp is not delineated by a hyperechoic surface line, a deep hypoechoic area, or a conically thickened outermost hyperechoic layer. (B) Color Doppler evaluation demonstrates a dendritic bloodstream signal. (C, D) Contrast-enhanced ultrasonography (CEUS) depicts a periphery-dominant enhancement (arrows) during the post vascular phase (left: CEUS, right: control).
A noncontrast computed tomogram (CT) did not demonstrate a gallbladder mass except for gallstones (see Figure 2A); meanwhile, a contrast CT revealed an early enhanced polyp. Interestingly, the contrast enhancement was not homogeneous but more prominent in the periphery, than in the center (see Figure 2B). There was no evidence of gallbladder wall invasion and enlarged lymph nodes were not found.
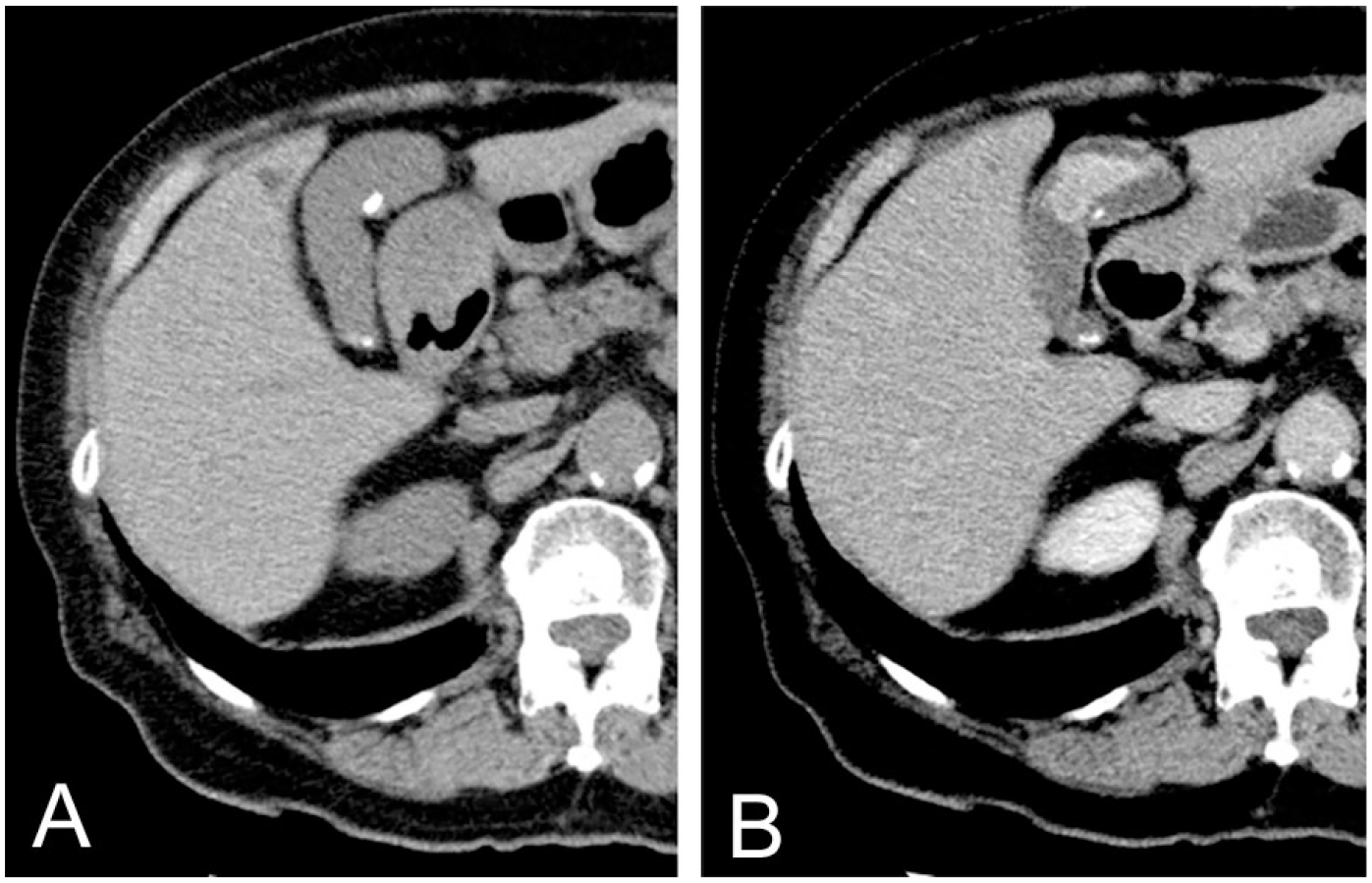
(A) A computed tomogram (CT) is provided and on the noncontrast study, it does not demonstrate a gallbladder mass except calcified stones. (B) However, the contrast CT study reveals an early enhanced polyp. The contrast enhancement is not homogeneous but more prominent in the periphery than in the center (delayed phase).
Magnetic resonance imaging (MRI) disclosed a low-intensity lesion, compared with the liver, during the T1-weighted image. In addition, a high-intensity lesion, compared with the liver, was noted on the T2-weighted image but no decreased-diffusion lesion was noted on the diffusion-weighted image (DWI). Hence, without diagnostic findings suggestive of an obvious advanced GBC or excluding an early GBC, a full-thickness laparoscopic cholecystectomy was performed.
A pedunculated polyp measuring 30 × 13 mm with a thick stalk, 2 to 3 mm in diameter, was apparent in the fundus, of the resected gallbladder (see Figure 3). The histopathology demonstrated a fibrous polyp. The polyp stroma consisted of edematous connective tissue containing gland- or duct-like elements and scattered inflammatory cell infiltrates. Capillaries were relatively evident in the periphery and larger blood vessels in the center (see Figure 4A–D).
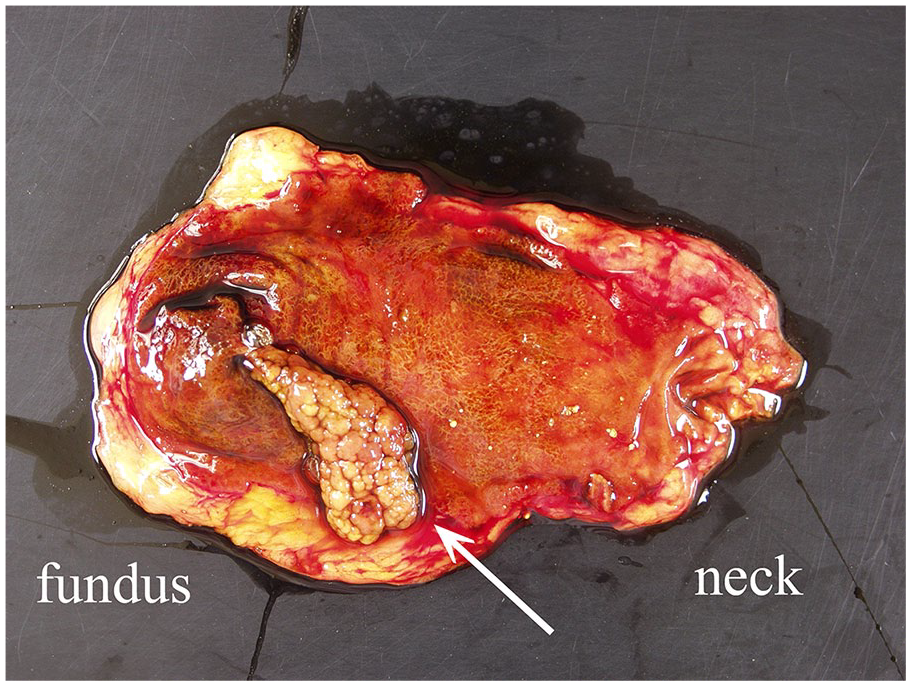
A fresh specimen is provided and it is opened on the peritoneal side along the long axis. A pedunculated polyp measuring 30 × 13 mm with a thick stalk, 2 to 3 mm in diameter, is apparent in the fundus of the resected gallbladder (see arrow).
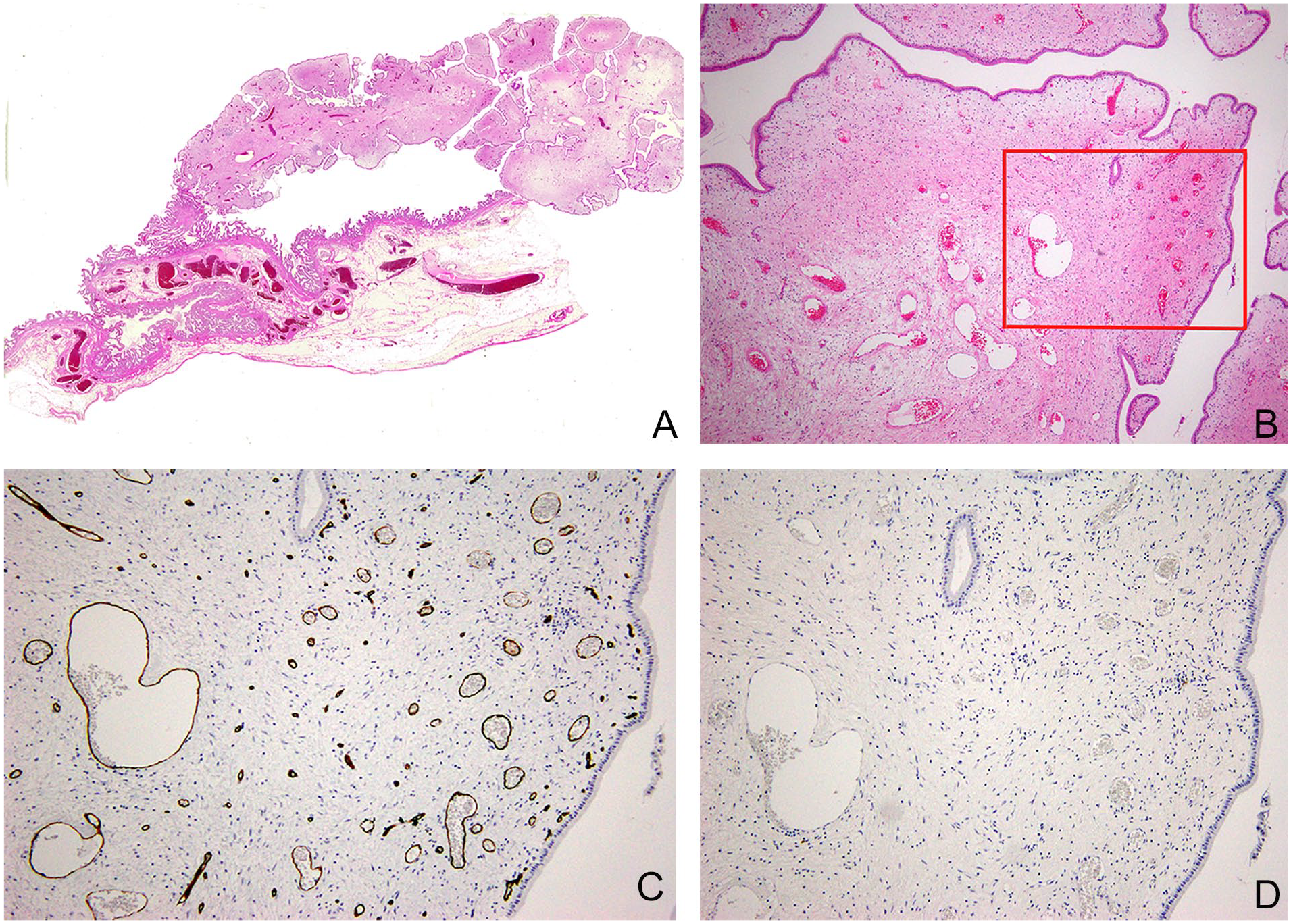
Histopathological findings are provided. (A) Loupe view (H&E) of the cut surface of the polyp. (B) Low power view (H&E). The histopathology indicates a fibrous polyp with a leaf-like configuration, consisting of edematous connective tissue stroma containing gland- or duct-like elements, different-sized vessels, and scattered inflammatory cell infiltrates. Capillaries are evident in the periphery and larger blood vessels in the center. (C, D) Medium-power view corresponding to the red frame of “B” (CD34, S-100 protein, respectively). The interstitial eosinophilic spindle cells are negative for both CD34 and S-100 protein, suggesting neither pericytic nor neurogenic in origin.
Discussion
A fibrous polyp of the gallbladder is very rare. The true incidence of this lesion is unknown. 2 Although fibrous polyps are usually smaller than 10 mm in diameter, they can occasionally be much larger. 1 Regarding signs and symptoms of a fibrous polyp, the patient shows no symptoms with little relevance to polyp size. The patient who was evaluated demonstrated nausea and vomiting, which was derived from her associated gallstones. A fibrous polyp is a benign condition and typically provides a good prognosis. A definite diagnosis of a fibrous polyp allows for no further treatment, if the patient has no symptoms, as well as a cholesterol polyp. However, a definite diagnosis is not easily ascertained. Hence, a large fibrous polyp requires a differential diagnosis and surgery to rule out gallbladder carcinoma.
Polyp size and stalk diameter are significant in the determination between a gallbladder polyp that might be benign or malignant. A polyp larger than 15 mm in diameter with a thin stalk would suggest a T1a carcinoma. 3 Meanwhile, a same-sized polyp with a thick stalk could be considered a T2 carcinoma, under certain conditions, namely, a polypoid gallbladder tumor with a deep hypoechoic area and a conically thickened outermost hyperechoic layer suggests a shallow T2 carcinoma. 4 However, a particular benign protruded lesion may rarely demonstrate similar sonographic findings as a shallow T2 carcinoma. 5 Although a hyperechoic surface line of the gallbladder polyp is reportedly characteristic of a fibrous polyp, 1 it was lacking in the present case. In addition, the polyp was not delineated by either a deep hypoechoic area or a conically thickened outermost hyperechoic layer. 4 Contrast-enhanced ultrasonography (CEUS) depicted a dendritic enhancement during the early vascular phase and a periphery-dominant enhancement during the post vascular phase. This has not been reported, with regard to a fibrous polyp. Even if endoscopic sonography was conducted for further investigation, it would not provide additional information regarding the polyp characteristic and the layer structure of the gallbladder wall.
Generally, a gallbladder polyp, which a noncontrast CT does not detect, could be a benign condition, 6 and a similar situation is expected with the reported MRI findings of a negative DWI. Regarding gallbladder carcinoma, a contrast CT shows a homogeneous enhancement. Meanwhile, as for the present case, a dynamic CT revealed a periphery-dominant enhancement, which was unique and noticeable. Nobuoka et al. has reported a similar periphery-dominant enhancement of a large fibrous polyp of the gallbladder on dynamic CT or MRI for the first time. 7
Overall, the imaging results in the present case suggested neither an obvious advanced GBC nor excluded an early GBC. Meanwhile, the case showed a periphery-dominant enhancement on dynamic CT and during the post vascular phase of CEUS, which could suggest a fibrous polyp. It was also noted that these findings correspond to the following pathophysiological findings. The polyp stroma consisted of edematous connective tissue with capillaries in the periphery and larger blood vessels in the center. The contrast material retention time is longer in capillaries than in large blood vessels. Consequently, a periphery-dominant contrast enhancement could be a pathognomonic image finding of a giant fibrous polyp of the gallbladder. The significance of this finding needs further studies by accumulating additional cases of this typology. Currently, as for a giant gallbladder polyp with a thick stalk showing a periphery-dominant contrast enhancement, a full-thickness laparoscopic cholecystectomy, and histopathologic examination of the resected gallbladder should be performed to avoid extensive surgery.
Conclusion
A giant gallbladder polyp with a thick stalk showing a periphery-dominant contrast enhancement could suggest a fibrous polyp and requires a full-thickness laparoscopic cholecystectomy and histopathologic examination of the resected gallbladder to avoid extensive surgery. The significance of this finding needs further studies by accumulating additional similar cases.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Compliance With Ethical Standards
All procedures followed were by the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964 and later versions. Written informed consent was obtained from the patient for being included in the study