
Abstract
Objective:
The upper limb tension test 1 (ULTT1) is commonly used by physical therapists for patients with complaints of radiating symptoms in their upper extremity following the path of the median nerve. Clinicians typically perform similar testing positions for patients, except for scapular position, which may vary between scapular blocking and scapular depression. This may alter the test results based on this positioning. The purpose of this study was to determine if there is a significant difference in median nerve morphology during the ULTT1 between resting and two scapular testing positions.
Materials and Methods:
Thirty healthy participants, 18 to 65 years of age, were tested using the ULTT1 in both blocked and depressed scapular positions. The height and width of the median nerve were measured by diagnostic sonography. Paired t tests were utilized to compare baseline, blocked, and depressed scapular positions with the ULTT1.
Results:
No statistically significant difference in height or width was found between resting, blocked, or depressed scapular positioning.
Conclusion:
There were inconclusive results regarding the morphology of the median nerve in this study.
Key Takeaways
Inconclusive results on nerve morphology comparing two scapular positions during the ULTT1. Research may be conducted on symptomatic patients to assist with more reliable test findings related to ULTT1.
A common reason for seeking neurologic care is peripheral neuropathy. 1 Because of its superficial positions running through narrowed regions and in areas of high risk of trauma, peripheral nerves are at an increased risk of injury. 2 Neuropraxia is the most common type of nerve injury which causes a transient physiologic block of the nerve. Sources of this block can come from pressure or stretch of the nerve and usually resolves in minutes or days. With continued pressure or stretch on the nerve, chronicity or progression of nerve injury can occur with subsequent motor and/or sensory changes in the dermatome/myotome of the nerve. Common nerves in the upper extremity that are affected from neuropraxia include the radial, ulnar, and median nerves. Physiologic and mechanical adaption resulting from injury of the median nerve often alters the ability for the nerve to conduct impulses into the distal extremity due to morphing or compression of the nerve, thus leading to a lack of afferent sensory information to the brain and efferent motor output to the forearm and hand.3,4 The median nerve follows a distinct pathway within the body from the medial and lateral cords of the brachial plexus, descending down the upper arm, continuing at the level of the elbow under the bicipital aponeurosis, and traveling distally to innervate the flexor muscle bellies of the forearm. The nerve then subsequently passes through a sheath of connective tissue known as the carpal tunnel, where it supplies motor function to the first three digits of the hand. 5 To determine where peripheral nerve dysfunction may be occurring, clinicians may utilize upper limb tension tests (ULTTs) to assist with diagnosing this condition. ULTTs continues to be investigated to provide more information on identifying peripheral nerve conditions, such as cervical radiculopathy (CR), carpal tunnel syndrome, and cubital tunnel syndrome.6,7 The median nerve ULTT (upper limb tension test 1 [ULTT1]) is of interest to researchers and clinicians due to the median nerve being a main contributor to the functionality of the hand. 8
The ULTT1 is most often used to identify median nerve pathologies related to radicular or neuropathic symptoms within the upper extremity.6,9 The ULTT1 is performed by an examiner or clinician as a multistep test, starting with the patient relaxed in supine. The examiner or clinician depresses the patient’s scapula, then performs 90° of shoulder abduction and external rotation, forearm supination, and elbow and wrist extension.6,9 The examiner or clinician may then have the patient perform a cervical side bend away from the side being tested to assist with determining nerve tension, with increased symptoms into the upper extremity being tested. Clinicians can utilize segmental positioning of distal to proximal segments to get a better idea of where, in the course of the nerve, the pathology is occurring. Segmental testing occurs at the cervical spine, glenohumeral joint, elbow, wrist, and hand, with scapular depression or blocking, which is used to mimic the resting position of the scapula. A positive test is patient-reported tension or dull pain within the forearm, wrist, or first three digits at any point in the test, indicating strain on the median nerve. 6 When using ULTT1 as a diagnostic tool, it is essential to determine the sensitivity and specificity of the test. Kleinrensink et al. 10 used buckle force transducers on cadavers to conclude that the ULTT1 with and without cervical side bending away from symptomatic side has both high specificity and sensitivity in determining median nerve lesions. Ghasemi et al. 11 concluded that the ULTT1 has high sensitivity in determining acute CR and recommended using the ULTT1 as a screening tool to diagnose CR. Talebi et al. 6 demonstrated high reliability and limited variability of the ULTT1 to identify carpal tunnel syndrome, with intratester reliability of the ULTT1 reported at 0.98 in healthy participants. Conversely, Davis et al. 12 reported that the false-positive rate was 88% during the ULTT1 procedure, concluding that most healthy participants were classified incorrectly. Using the ULTT1 for diagnosis and management can be advantageous when performed correctly because it can save time and cost, minimizing further workups and referrals. 11 However, as outlined above, some questions remain regarding its execution, which may be related to the way in which the test is conducted, including blocking or depressing the scapula. Standardization of testing positions may help with increasing the reliability and improve diagnosing peripheral nerve pathology. Since the scapular position is the structure that is most variable in the literature, it may be useful to visualize any changes that may occur in the nerve that would affect the outcome of the testing.
Identifying symptoms of peripheral neuropathy is a common characteristic of ULTTs; however, the test itself cannot visualize the characteristics of the nerve. Sonographic techniques used in diagnostic imaging have been used to visualize peripheral nerve morphologic features for diagnostic information and therapeutic decision-making. 4 Superficial structures, such as the median nerve, can be identified in adequate detail using ultrasonography (US).1,13 The nerve is depicted as a round hypoechoic structure with a honeycomb-like appearance and a hyperechoic border. This, in turn, contrasts well with more surrounding hypoechoic structures such as healthy muscle, making it easier to visualize on US in these areas. 14 Most research that involves US measurements of the median nerve utilizes cross-sectional area (CSA) in subjects with nerve pathology. Pathology commonly occurs in the form of edema or inflammation of the nerve from compression, disease, or trauma. Hersh et al. 15 determined a near-perfect correlation when comparing CSA measurements with a magnetic resonance imaging (MRI), to those with US. This suggests US has a high reliability in measuring CSA. 15 An increase in the CSA of the median nerve is a common finding in peripheral neuropathies such as carpal or cubital tunnel syndrome. 1 Compression results in thinning in the area of compression and can result in adjacent proximal thickening. This can be a sign of nerve compression and an increased CSA. It is also possible to calculate a flattening ratio (FR) between these areas by utilizing the major and minor axes of the nerve. 16 In a systematic review by Gonzalez-Suarez et al., 17 they analyzed several studies that utilized CSA and FR to determine reliability of measurements comparing external landmarks versus sonographic landmarks, with external landmarks having excellent inter-rater and intrarater reliability. Intrarater reliability has been found to be good when measuring CSA, FR, swelling ratio, and mean gray scale when measuring the median nerve using ultrasonographic imaging. 16 Overall, US is a noninvasive technique that continues to become more advanced in diagnosing peripheral neuropathies, including those of the median nerve, and can be a useful tool in making medical decisions, relative to a plan of care. 3
There is extensive literature regarding median nerve sonography, but most are in relation to its CSA and the change in size with pathology, most commonly carpal tunnel syndrome which limits the information to a specialized population. In general, there is limited literature on identifying median nerve morphology changes other than CSA along with minimal studies with reference values of healthy median nerves. 18 In this literature review, there was limited research found on transverse or axial US images of the median nerve during specialized testing, such as the ULTT. There are conflicting opinions among physical therapists (PTs) when performing the ULTT1 in different testing positions, such as whether to use scapular blocking or scapular depression during performance of the test in symptomatic individuals. Investigating in this research using ultrasound may help construct an understanding of how different testing positions influence median nerve morphology. This study hypothesis was that there would be a change in the median nerve morphology in the distal forearm, as visualized by diagnostic imaging, when comparing scapular blocking and scapular depression positions during the ULTT1. The outcome of this study was designed to help both clinicians and researchers understand if there is a change in the median nerve morphology with different scapular positions, as well as if this would affect test results.
Materials and Methods
Design
This study was a cross-sectional study conducted between September 15, 2020 and September 25, 2020. The host institution’s Institutional Review Board approved the study.
Subjects/Participants
Investigators marketed participation in the study to all faculty, staff, and students at the host institution, a regional Midwest private university. An e-mail was distributed through the university e-mail database to gather healthy male and female subjects between the ages of 18 and 65 years old, which included exclusion criteria to participate in the study. Subjects were excluded from the study if they had neck, shoulder, elbow, wrist, or back pain; range of motion deficits that would prevent them from doing the testing positions; or neurologic symptoms of the upper quarter. If subjects volunteered to be in the study with no exclusion criteria, investigators educated subjects on what to expect during testing. Subjects that continued to agree to participate in the study signed the provided informed consent prior to testing.
COVID-19
Investigators required a check-in procedure for subjects due to the COVID-19 pandemic. Subjects underwent a temperature check, pulse oximetry reading, and the university-specific public health screen when they arrived at the facility. Subjects and the examiners were required to always wear a face mask during testing. Along with the check-in procedure, investigators also implemented a strict cleaning procedure, which included disinfecting all equipment and tables before and after all procedures as well as miscellaneous items wiped down and cleaned between subjects, and hand washing or hand sanitizing between subjects.
Tools/Instruments
A GE Logiq E ultrasound unit was used to capture images and measurements using a L4-12t linear transducer. Investigators used the musculoskeletal presets for the wrist which included a frequency of 13 MHz to appropriately identify the median nerve at the distal forearm and were held constant for each subject. Any changes to the image brightness, if needed, were made by adjusting the gain on the unit. An acoustic gel was used as the medium for ultrasound transmission. One student investigator measured passive range of motion of the dominant extremity shoulder and elbow with a standard manual goniometer. A digital timer set at 30 seconds measured rest breaks between each trial. Additional equipment to aid in data collection included a computer with Microsoft Excel, statistical program SPSS, and a high-low adjustable therapy plinth.
Examiners
One licensed PT with 10 years of clinical experience and musculoskeletal sonography certification performed sonography and corresponding measurements. Three second-year physical therapy student investigators assisted the licensed PT with testing, range of motion measurements, and data collection. The students had previous education, training, and assessment of range of motion skills through their accredited physical therapy program. One student PT performed the ULTT1, whereas another measured range of motion on each subject. The third PT entered data and timed the rest period between trials. Roles remained constant for each investigator during the study. Prior to testing, the physical therapy students were educated and instructed on administering the ULTT1 by the licensed PT and trial runs were performed on a pilot test subject.
Procedure
Subjects were instructed to wear nonrestrictive clothing that allowed for full motion of the upper extremity with their distal arm exposed. The subject’s self-reported dominant arm was used for testing. Subjects were positioned in supine with legs extended on an adjustable therapy plinth. To complete baseline measurements, subjects were supine with their arm supinated and at their side and wrist and fingers resting in neutral. A mark was then placed 4 inches (10.16 cm) proximal from the distal wrist crease which was determined to be an area that shows best visualization and excellent inter-rater and intrarater reliability of the median nerve, according to a study by Gonzalez-Suarez et al. 17 The US transducer was placed on the anterior surface of the forearm to produce an axial image of the median nerve with the probe marker positioned medially for correct and consistent identification of the nerve on the ultrasound equipment monitor. When the licensed PT determined the clearest image, the image was captured, frozen, and saved on the equipment system’s hard drive. This was followed by using the ultrasound equipment system’s calipers to measure the height and width of the nerve, in centimeters. The caliper markers were again saved with a numerical identifier for the subject (see Figure 1). Investigators determined width to be the longest area of the nerve, and height measured perpendicular to width at highest area of nerve. Height and width were used in this study due to investigator hypothesis that CSA of the median nerve would remain consistent in a healthy population and height and width may change due to a flattening of the nerve due to strain. To maintain consistency of the scapular position, the same student PT performed each ULTT1 throughout the data collection process. Subjects were instructed to inform the investigators when they start to feel symptoms of stretching, aching, or tingling in their first, second, and third fingers during the elbow extension portion of the ULTT1 to determine their end range of median nerve tension.

This sonogram demonstrates the participant’s median nerve. The yellow dotted lines at 1 and 2 indicate the margins of the median nerve. Dotted line at 1 indicates nerve height, and dotted line at 2 indicates nerve width and were measured in centimeters.
The first resting measurement was taken with the patient supine with legs extended and arms at their side with palms up. The transducer was placed at the 4-inch mark and identified the median nerve, on the ultrasound equipment monitor. Height and width of the nerve were taken with the calipers and recorded. Next, the subject was positioned to prepare for the ULTT1 measurements. The ULLT1 technique used in the study was the sequence described by Talebi et al. and Riley et al.6,9 which was “patient supine with legs extended and cervical spine in neutral, scapular positioning, shoulder abduction to 90 degrees, elbow flexion to 90 degrees, and shoulder external rotation to end range.” For scapular depression, the student investigator placed their forearm closest to the subject’s body over the superior aspect of the subject’s shoulder over the superior border of the scapula in a perpendicular position and pulled their forearm in an inferior direction to the subject’s shoulder (see Figure 2). For scapular blocking, the student investigator placed their forearm just above the subject’s superior aspect of their shoulder similar to scapular depression with the exception of “blocking” the scapula from moving superiorly during the testing. The distal hand placement the student investigator utilized was a “pistol grip,” where the student investigator’s index finger abducted the subject’s thumb and the student investigator’s palm extended the subject’s digits and wrist (see Figure 3). The student investigator then placed the subject’s forearm in supination to end range and passively moved into elbow extension until the subject verbalized dull tingling or aching in their first, second, and/or third digits of the extremity tested.6,9 The student investigator held elbow extension, and another student measured elbow extension with a goniometer, while the lead investigator captured the image, followed by measurement of the nerve height and width with the GE Logiq E calipers. The angle of the elbow was recorded and used for all subsequent trials with the same subject for both scapular depression and blocking to keep distal segments consistent while changing scapular positions. Three trials were performed and measured for scapular blocking and scapular depression. The subject’s arm was positioned to baseline with a 30-second rest period before completing the next scapular position. The average measurements for nerve height and width of the scapular positions were used for statistical analysis. Resting position nerve measurements were used for a baseline measurement.
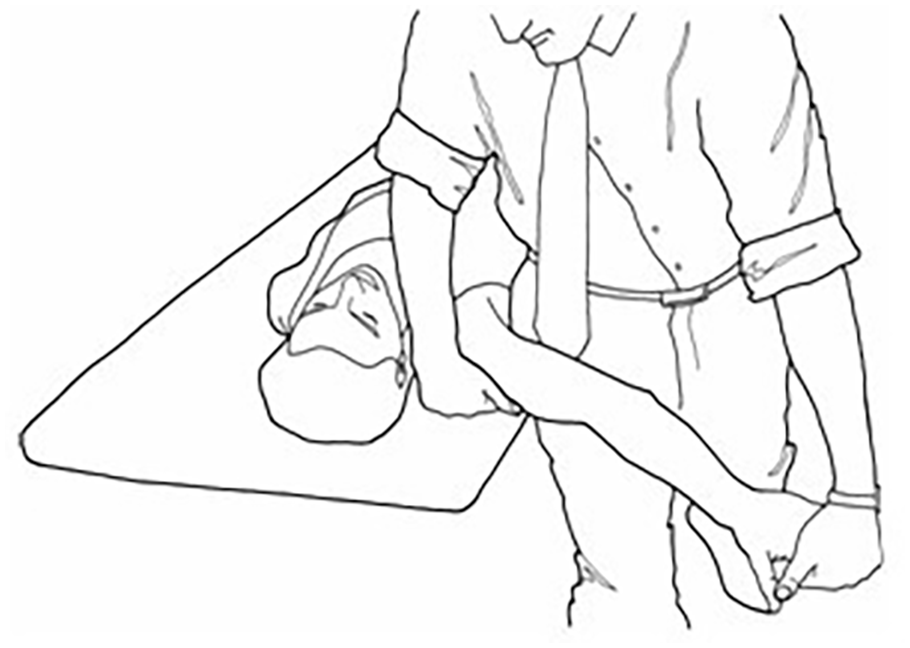
Diagram of how the ULTT1 is conducted. ULTT1, upper limb tension test 1.
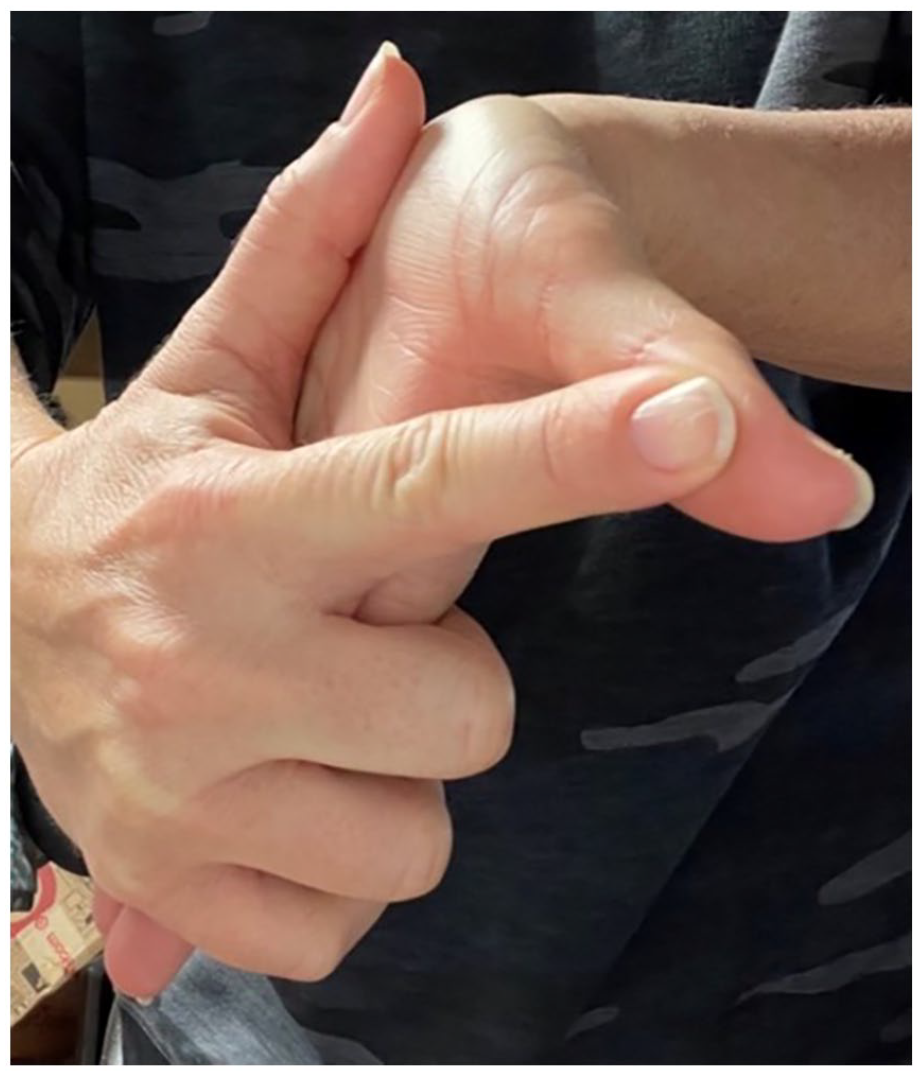
Illustration of a pistol grip.
Statistical/Data Analysis
Investigators used IBM Statistics SPSS version 27 software with a paired t test with a P value of .05 to test our hypothesis of a possible change in the median nerve morphology in the distal forearm, as visualized by diagnostic imaging, when comparing scapular blocking and scapular depression positions during the ULTT1. Comparisons were made to the following items: condition 1: nerve height with arm at side, condition 2: nerve height with scapula blocked, and condition 3: nerve height with scapula depressed. This was followed by condition 1: nerve width with arm at side, condition 2: nerve width with scapula blocked, and condition 3: nerve width with scapula depressed. Comparisons were made between baseline and blocked, baseline and depressed, and blocked and depressed. All data were entered into a Microsoft Excel spreadsheet by a student investigator, and statistical analysis was entered and analyzed by the primary investigator.
Results
This study included a total of 30 participants with 18 females and 12 males with an average age of 27.7 ± 8.80 years and a range of 22 to 55 years. Of the 30 participants, 27 were right arm dominant, and three were left arm dominant. Table 1 refers to the mean height and width (cm) of the median nerve in resting, blocked, and depressed positions. Table 2 refers to the mean difference in height (cm) between each position of the median nerve, a complete standard deviation (SD) of all participating subjects, and P values indicating significance during resting, blocked, and depressed positions. Table 3 refers to the mean difference in width (cm) between each position of the median nerve, a complete SD of all participating subjects, and P values indicating significance during resting, blocked, and depressed positions. Comparisons between resting and blocked, resting and depressed, and blocked and depressed were made using a paired t-test to identify if there was a significant difference for height and/or width in each position (see Tables 2 and 3). The complete data presented in Tables 2 and 3 indicate no significant difference (P value) in height and width of the median nerve using a P interval >.05 for all compared scapular positions.
Mean Height and Width of the Median Nerve in Each Subject Position.

Paired t Test Comparison of the Median Nerve Height in Different Scapular Positions.

Paired t Test Comparison of the Median Nerve Width in Different Scapular Positions.

Discussion
Although clinicians have differing opinions over scapular positioning during the ULTT1, the current weight of evidence suggests that the scapula should be in a neutrally blocked position compared with the scapula being depressed. The scapula is not considered part of the nerve “sensitization” position within the ULTT and the importance of standardization of this position should be considered within clinical practice. Riley et al. 9 found that having the scapula in a depressed position induced considerable changes in the test results and determined that it was less reliable than having the scapula blocked. Legakis and Boyd 19 found that with the scapula depressed, sensory responses were both heightened and occurred earlier during the testing phase when investigators performed ULTT1. This minor change with the testing position at the scapula could decrease validity of that testing position. When investigators placed the scapula in a blocked position, it allowed individuals to have a greater degree of elbow extension and an increase in median nerve tension during the testing procedure. Therefore, they concluded that scapular blocking should be considered the standard positioning for the ULTT1. 19 Thus, there remains some controversy over the most appropriate scapular positioning to maximize the effectiveness of the ULTT1. The ULTT1 is used often in combination within a clinical prediction rule for CR. Standardization of the testing position for the ULTT1 would also be helpful in improving likelihood ratios for diagnosing pathology such as CR and decrease the need for expensive testing such as MRI or nerve conduction studies.
The data from this study determined no significant difference in the height or width of the median nerve between baseline, blocked, and depressed positions with elbow extension held constant and cervical spine in neutral. Although subjects reported symptoms with the testing positions that could indicate nerve tension, the quantification of nerve height and width did not provide strong evidence to support any changes in nerve morphology.
Limitations
There were some inherent limitations due to the study design and the convenient sample of participants. The study contained a small sample size of healthy individuals due to limiting the sample to individuals within the university. This small sample size cannot be generalized to the symptomatic population. Another limitation was the variability in the angle measurements of elbow extension between participants. Elbow extension measurements ranged from 15° to 55°, with an average of 34.8° ± 9.78°, with no participants being able to reach full elbow extension without symptoms into the first, second, and third digits of the hand.
Future studies can incorporate cervical side-bending away or toward the test side before taking the median nerve measurements. Cervical side-bending is commonly applied to the ULTT1 but was omitted from our technique due to the primary investigator’s decision. Another subsequent study can focus on comparing symptomatic and asymptomatic populations. It is clinically relevant to explore differences in the median nerve between participants who have median nerve pathology and those who do not.
Conclusion
The purpose of this study was to determine whether there was a difference in the morphology of the median nerve between blocked and depressed positions of the ULTT1 in a sample of healthy subjects. The results of this study would suggest that there was no statistical difference between resting, blocked, and depressed scapular positions during the ULTT1, but this does not indicate differences in tension on the median nerve in either scapular position, even with subject reported symptoms. Continued research may be done to determine a standard scapular position with quantitative anatomical findings of nerve morphology to support validity of test findings and determine how to best optimize the ULTT1.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this research was provided by Briar Cliff University.