
Abstract
Objective:
Establish median nerve cross-sectional area (CSA) reference values and identify patient-level factors impacting diagnostic thresholds.
Materials and Methods:
Studies were identified through a robust search of multiple databases, and quality assessment was conducted using a modified version of the National Institute of Health Study Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies. A meta-analysis was performed to identify normative values stratified by anatomic location. A meta-regression was conducted to examine heterogeneity effects of age, sex, and laterality.
Results:
The meta-analysis included 73 studies; 41 (56.2%) were high quality. The median nerve CSA [95% confidence interval, CI] was 6.46 mm2 [6.09–6.84], 8.68 mm2 [8.22–9.13], and 8.60 mm2 [8.23–8.97] at the proximal forearm, the carpal tunnel inlet, and the proximal carpal tunnel, respectively. Age was positively associated with CSA at the level of proximal carpal tunnel (β = 0.03 mm2, P = .047). Men (9.42 mm2 [8.06–10.78]) had statistically larger proximal tunnel CSA (P = .03) as compared with women (7.71 mm2 [7.01–8.42]). No difference was noted in laterality.
Conclusion:
A reference value for median nerve CSA in the carpal tunnel is 8.60 mm2. Adjustments may be required in pediatrics or older adults. The diagnostic threshold of 10.0 mm2 for male patients should be cautiously applied as the upper limit of normative averages surpasses this threshold.
Sonographic imaging is becoming widely used for the examination of peripheral nerves, particularly in the diagnosis of carpal tunnel syndrome (CTS), where a growing body of literature is examining the diagnostic accuracy of sonography for CTS.1–3 Research and clinical approaches primarily compare median nerve cross-sectional area (CSA) to a diagnostic threshold (e.g., 10 mm2) or use a within-arm comparison of the CSA in the carpal tunnel to the CSA in the forearm.4–6 Sonography has been shown to demonstrate a better false-positive rate at 23% compared with the “gold standard” of nerve conduction at 43%. 1 Recent expert consensus suggests that combining sonography with other clinical measures 7 can increase diagnostic accuracy 8 and may be able to differentiate severity of CTS. 9
Most researchers examining diagnostic accuracy or developing diagnostic thresholds for sonographic measurements enroll a unique sample of healthy individuals to serve as reference values, in their individual studies. These comparative samples are often substantially small and purposefully recruited to match the patient population of the primary study. Although a few studies have been conducted to report normative values within specific populations10–12 and across different demographic factors,13,14 these studies do not provide the substantially large, heterogeneous samples necessary to serve as stand-alone reference values, for all clinical patients or research protocols.
With the proliferation of sonographic measurement of the median nerve in diagnostic studies and clinical trials, along with the increasing clinical use of sonography for screening and prevention of CTS, there is a need to establish a robust set of normative reference values for these measures across various populations, ages, and sexes. Thus, the purpose of this meta-analysis was to locate all published data on median nerve CSA measurements in healthy participants, statistically combine the data to establish references values, and identify patient-level factors that may impact how diagnostic thresholds are considered within clinical practice and research.
Materials and Methods
Search Strategy
This review was designed to meet the criteria of the Preferred Reporting of Items for Systematic Reviews and Meta-Analyses. 15 The study protocol was registered with the International Prospective Register of Systematic Reviews (CRD42016037286) and the detailed search and selection methodology has been previously published. 16 An initial bibliographic search was completed by a clinical and research librarian on March 20, 2017, and an updated search was conducted on May 31, 2019. Searches were conducted in Ovid MEDLINE, Embase, Cochrane Library, CINAHL, and SPORTDiscus using a combination of subject headings (when available) and keywords for concepts of peripheral nerves, reference values, or carpal tunnel and ultrasonography to capture articles published since the year 2000. The detailed search strategies for each database are included (see Supplemental Table 1). Additional searches were conducted in ClinicalTrials.gov, the tables of contents of journals within related medical (e.g., imaging, neurology) and injury prevention fields (e.g., human factors and industrial engineering), and the reference lists of relevant review articles identified in the search process.
Study Selection
A review team with varied training in sonographic imaging, rehabilitation, and medicine followed a standardized protocol to complete the study selection process. 16 Following removal of duplicates, all abstracts were imported into Covidence (Veritas Health Innovation Ltd; Melbourne, Australia) and independently screened by two reviewers. Full texts were obtained for any article that at least one reviewer indicated used sonography to examine the peripheral nerves of the upper extremity in healthy individuals. All full texts were independently reviewed for eligibility by two reviewers to identify studies that measured median nerve CSA in healthy participants using sonography. A registered musculoskeletal sonographer with more than 10 years of experience examined articles with discrepancies between the primary reviewers, and final inclusion was determined by consensus among the reviewers. Studies that used a transducer <10 MHz, a measurement technique other than direct trace around the internal hyperechoic border of the nerve, or a primary measurement of CSA in cm2 rather than mm2 were excluded. When units of measurement were not reported in the methods, studies were excluded if cm2 appeared in figures or whole numbers were used to report CSA. Studies that lacked a clear anatomical description or combined measures from different locations across participants (e.g., largest CSA measured across the carpal tunnel region) were also excluded.
Data Extraction and Quality Assessment
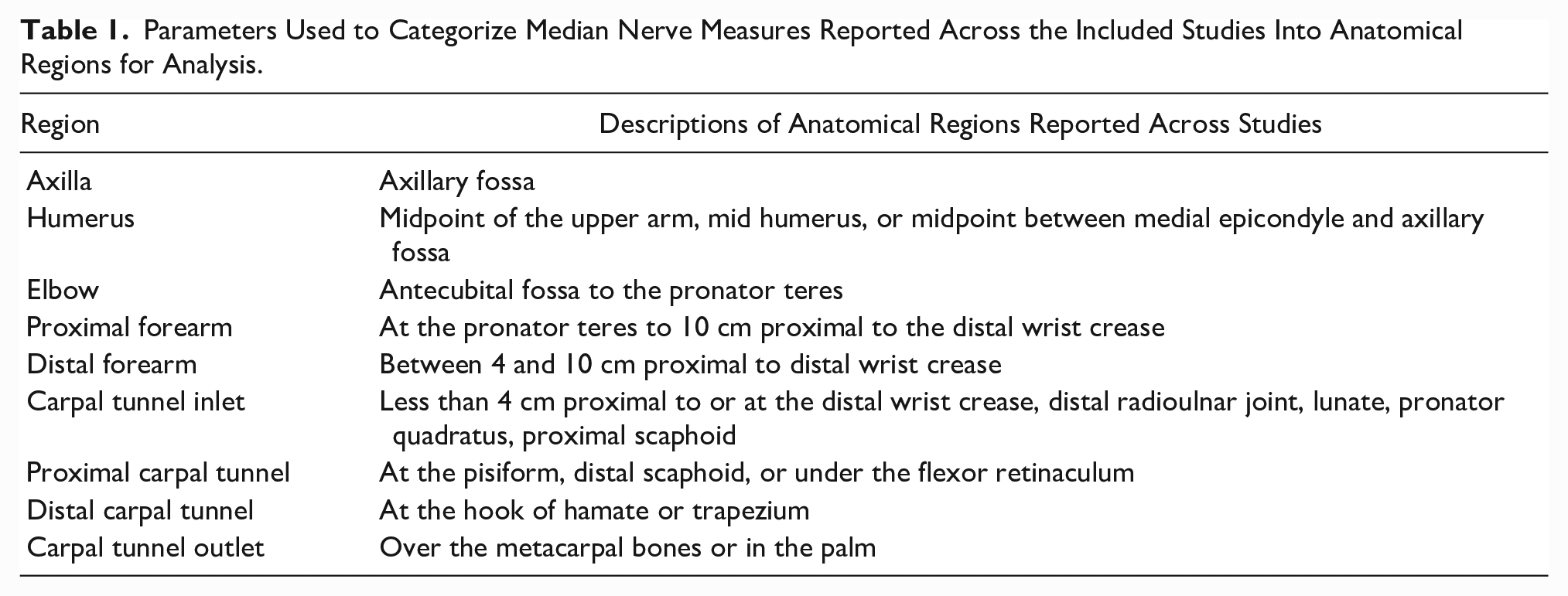
For each study, the number, average age, and distributions of sex and handedness of participants were extracted. Central tendency and variance for each sonographic CSA measurement of the median nerve were entered into the data set across nine anatomic locations from the axilla to the distal carpal tunnel (see Table 1). To obtain missing data, the corresponding authors were contacted when articles did not report both centrality and variance of CSA for healthy participants. Because the purpose of this review was limited to measures of the median nerve in healthy participants, additional information related to overall study (e.g., design, diagnosis, intervention) were not extracted or reported.
Parameters Used to Categorize Median Nerve Measures Reported Across the Included Studies Into Anatomical Regions for Analysis.
Quality assessment was conducted using a modified version of the National Institute of Health Study Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies. 17 Studies were scored as having fully met (1 point), partially met (0.5 points), or not met (0 points) eight quality criteria related to the imaging of healthy participants in the study. 16 Studies that did not report enough detail to determine whether a criterion was met received no points, and studies that included only healthy participants received full points for criteria that required differentiation between groups (e.g., blinding of raters to participant status). Two reviewers individually scored each article, and a third reviewer resolved any differences. Average quality across the included studies was calculated, and individual articles were categorized into three quality levels: (1) high quality: > 6.0 points; (2) fair quality: 4.5–6.0 points; and (3) poor quality: < 4.5 points.
Statistical Analysis
A meta-analysis was performed to identify normative values for sonographic measurement of median nerve CSA stratified by anatomic location. Weighted averages were calculated for each anatomic location using random-effects models specifying the mean value of each study-specific median nerve CSA as an effect size. Standard errors for each study mean were obtained (in order of preference): (1) using directly reported standard errors, (2) calculated from standard deviation (SD) and sample size, or (3) using the sample range to compute an SD. Overall measures, study-specific effect sizes, and 95% confidence intervals (CIs) were displayed in forest plots by anatomic location, and the I2 test statistic was used to evaluate heterogeneity of CSA means across studies. A meta-regression was conducted to examine heterogeneity effects of age (i.e., mean study age) and sex (i.e., % male in study) at the two most clinically used anatomical locations (i.e., proximal forearm, proximal carpal tunnel). Finally, means were reported by subgroups of sex and hand dominance using studies that reported CSA values in these two locations by these subgroups or that had a homogeneous sample (e.g., all females, all dominant hands); differences in CSA means by sex and hand dominance were tested. Meta-analyses were conducted using Stata V17 (College Station, TX).
Results
Study Selection
The flow of records through the study selection process is presented in Figure 1. Screening was conducted for 18 592 unique records. A total of 418 full-text articles were reviewed for eligibility due to abstracts indicating that sonographic measurement of the median nerve was conducted in the study. Articles were excluded that did not evaluate median nerve CSA (n = 75), did not include healthy participants (n = 34), or did not use an appropriate measurement technique (n = 166). In addition, 69 articles were excluded due to missing data or re-reporting of healthy participant data that had been used in previous studies already included in the review. One study was identified as an outlier and excluded; this study reported an average CSA of approximately twice the size reported by the 20 other studies within the same anatomical region. 18 Data from the remaining 73 articles were included in the meta-analysis.
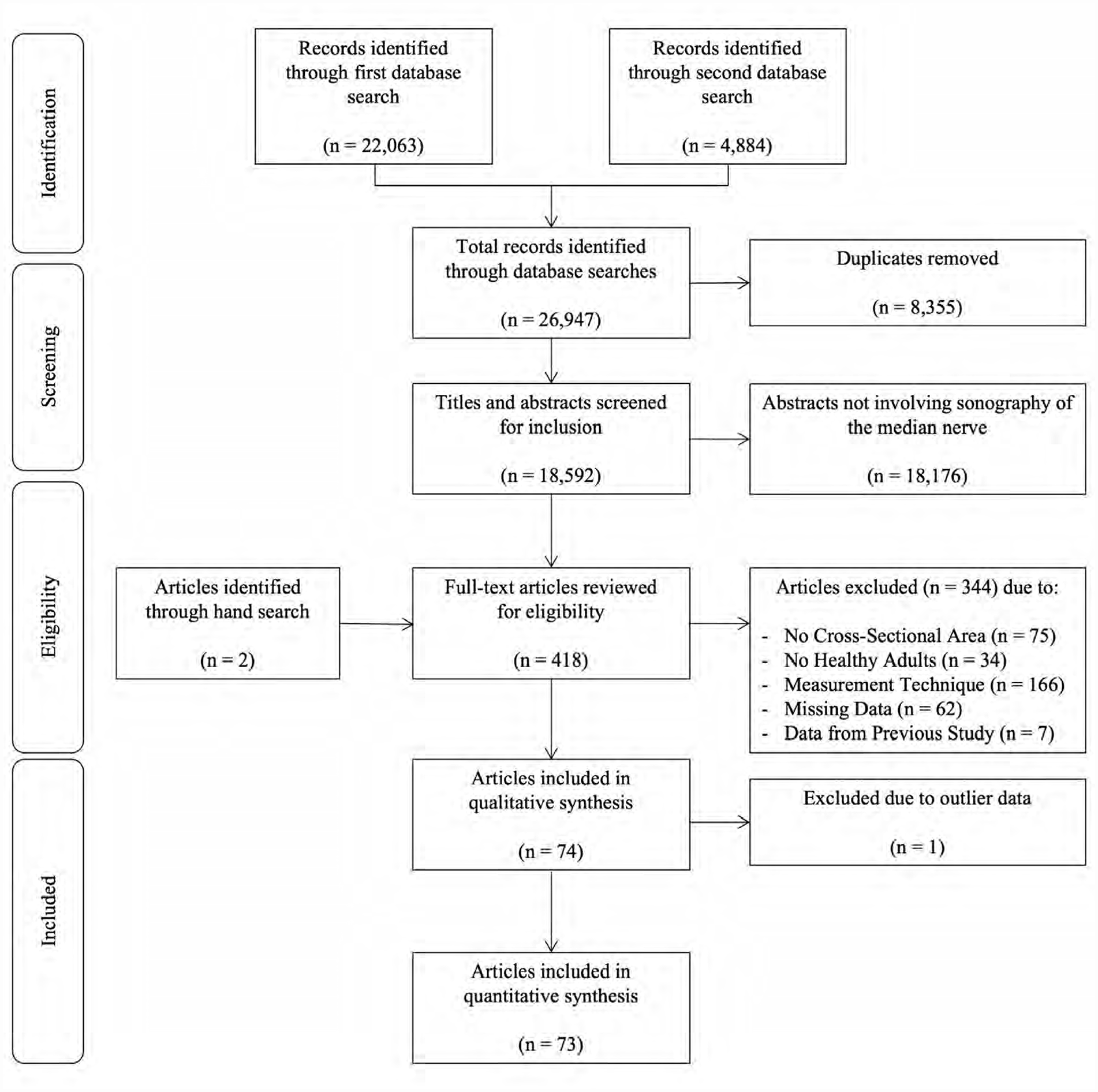
Flow chart of studies through the search, screening, eligibility, and inclusion process.
Study Characteristics and Quality
The proximal carpal tunnel (47/73, 64.4%), carpal tunnel inlet (35/73, 47.9%), and proximal forearm (20/73, 27.4%) were the most common anatomical locations of CSA measurement among the included studies. The meta-analytic average age of healthy participants across all articles in the sample was 43.6 years. The average quality rating across the included studies was 6.1 of 8.0, with 41 of 73 (56.2%) studies identified as high quality, 28 of 73 (38.4%) fair quality, and 5 of 73 (6.8%) poor quality (see Table 2). Quality of the image acquisition process was the criterion most often partially or not met based on the description in the articles (i.e., only 37.8% fully met this criterion). Only half of the studies indicated the qualifications of the individuals obtaining or measuring the sonographic data.
A Quality Assessment of Included Published Studies, Sorted By Their Quality Score.

Green plus = satisfactorily met the criterion; yellow plus = partially met the criterion; red minus = did not meet criterion; gray question mark = did not report on the criterion. Quality assessment was conducted using a modified version of the National Institute of Health Study Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies 17 using the eight criteria as previously described. 16
Meta-analysis of Healthy Median Nerve CSA
The weighted averages and CIs for median nerve CSA across the nine anatomic regions are presented in Table 3. The median nerve CSA was approximately 8–9 mm2 in the upper arm, elbow, and wrist, with a smaller CSA noted in forearm. In the most frequently measured regions, CSA was 6.46 mm2 (95% CI: 6.09–6.84) in the proximal forearm, 8.60 mm2 (95% CI: 8.23–8.97) at the level of the pisiform in the proximal carpal tunnel, and 8.68 mm2 (95% CI: 8.22–9.13) at inlet to the carpal tunnel (see Figures 2 and 3). Most CIs for the weighted means were approximately ±0.5 mm2; however, these intervals were larger for measurements in the upper arm, the distal carpal tunnel, and the carpal tunnel outlet indicating either wider variability in nerve size or increased measurement error in these locations. The I2 values indicated heterogeneity across the included studies suggesting potential moderating effects within the individual study designs or samples and confirming the need for further meta-regression and moderator analyses. Forest plots for the additional anatomical regions are provided and these give a quick graphic summary and direction of the data (see Supplemental Figures 1–6).
Meta-Analytic Averages for Cross-Sectional Area (CSA) of the Median Nerve Within Healthy Individuals Across Anatomical Regions of the Upper Extremity.
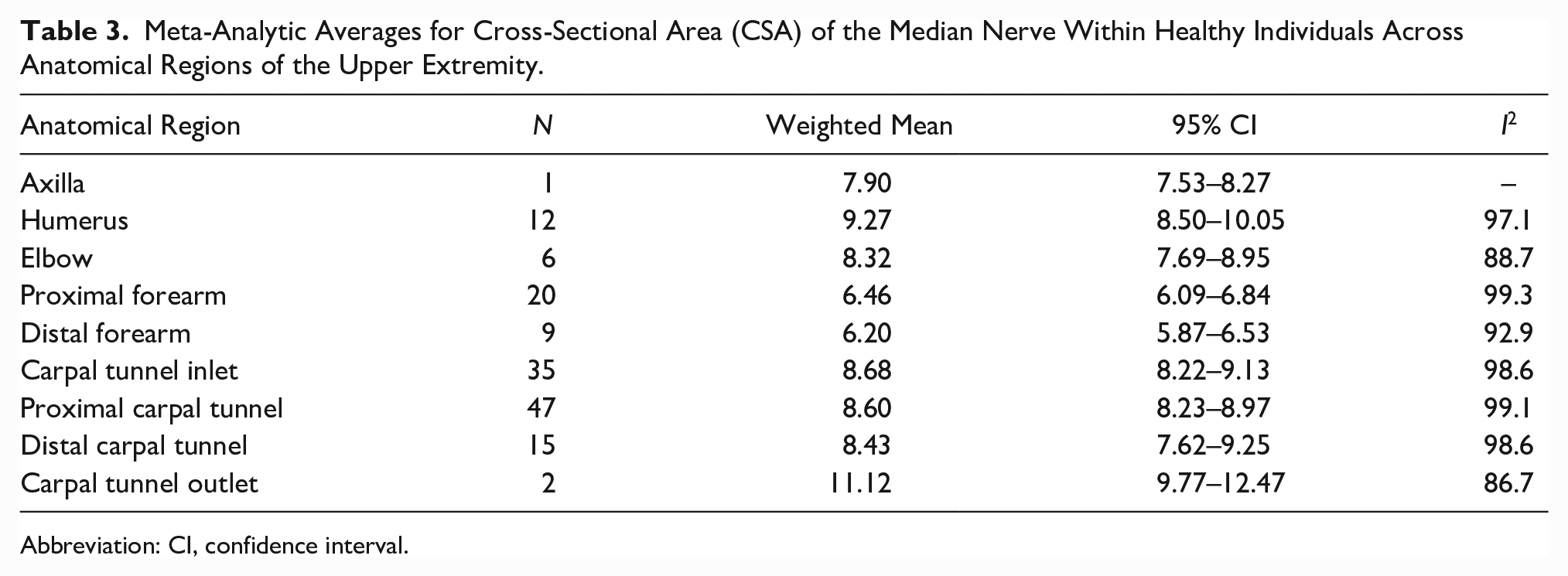
Abbreviation: CI, confidence interval.
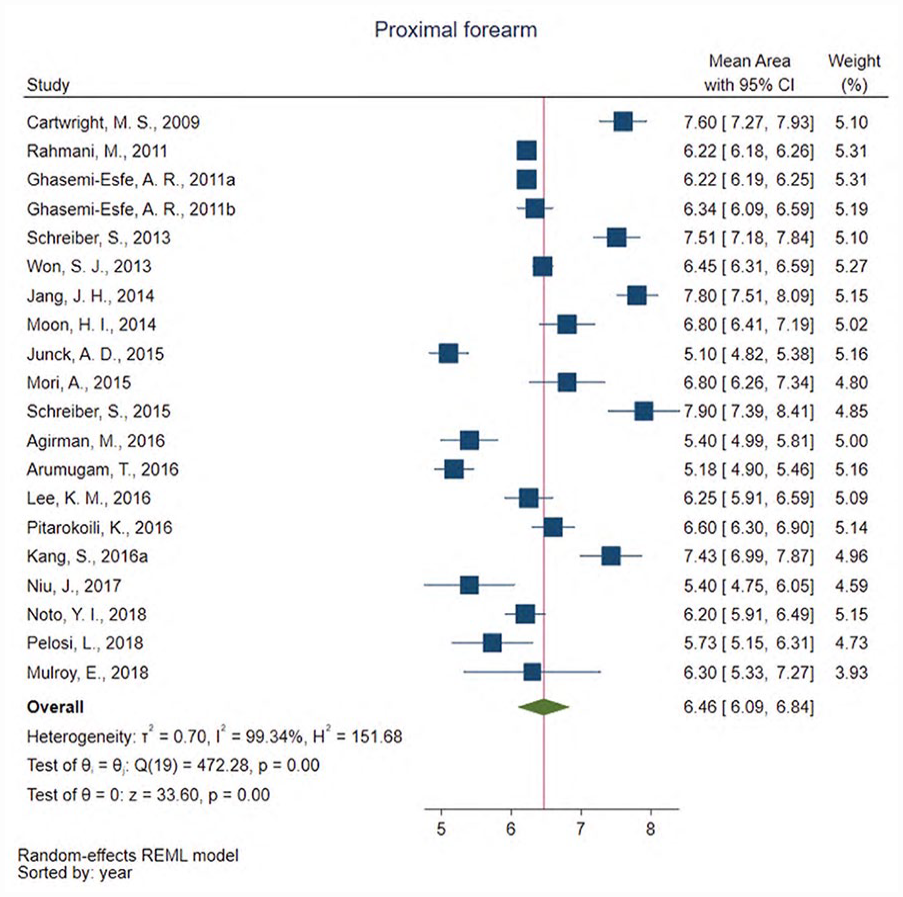
Forest plot of meta-analysis results showing the direction and magnitude of the weighted averages of median nerve cross-sectional area (CSA) in the proximal forearm 10 cm or greater from the wrist across individual studies. CI, confidence interval.
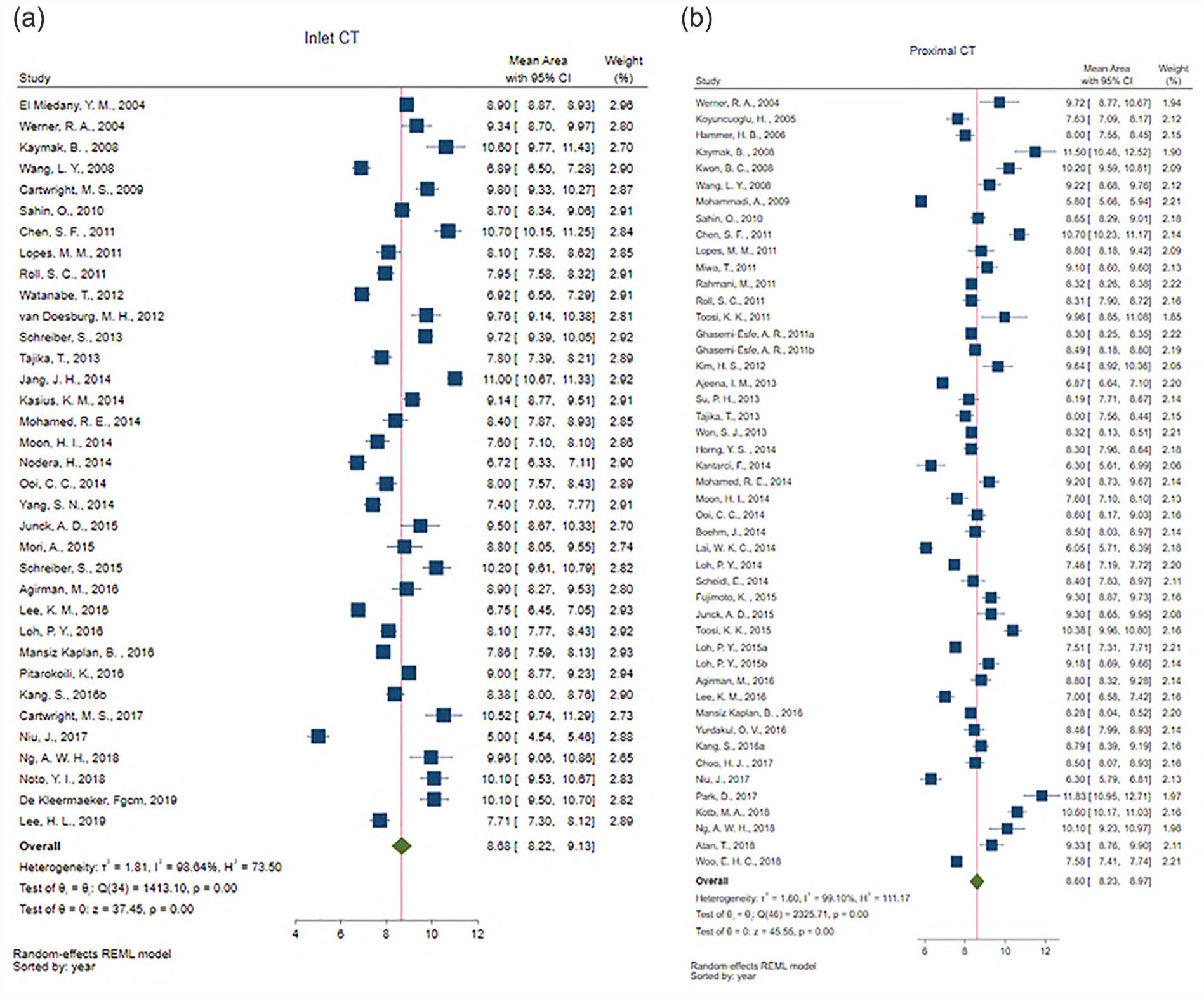
Forest plot of meta-analysis results showing the direction and magnitude of the weighted averages of median nerve cross-sectional area (CSA) at the inlet to the carpal tunnel (CT) up to 4cm proximal to the radial carpal joint (i.e., distal wrist crease; (a)) and proximal CT at the level of the pisiform (b) across individual studies. CI, confidence interval.
Meta-regression and Moderator Analysis of Study Factors Related to CSA
Five studies were excluded from the meta-regression due to missing data for average age or sex distribution (i.e., % male). Among the remaining studies, there was no significant effect of sex distribution or age in proximal forearm CSA (sex, P = .809; age, P = .418) and no effect of sex distribution on proximal carpal tunnel CSA (sex, P = .112). There was a statically significant effect of age on proximal carpal tunnel CSA (P = .047), such that, assuming a linear trend, each year of increase or decrease from the average age of the sample (i.e., 43.6 years) would result in a subsequent increase or decrease in CSA by 0.03 mm2 [95% CI: 0.00–0.07]. Thus, assuming a linear trend, the estimated range of normal CSA at the pisiform for adults aged 18–65 years would be 7.83–9.24 mm2.
Only three studies reported stratified data by either sex or hand dominance at the proximal forearm, so that, further evaluation of these factors at this location was not completed. Ten studies provided proximal carpal tunnel CSA values stratified by sex (see Figure 4). The weighted average CSA of these 10 studies was equal to the overall weighted average of the 47 studies measuring CSA at this location (i.e., approximately 8.60 mm2); however, men (9.42 mm2 [8.06–10.78]) had statistically larger weighted average CSA (P = .03) as compared with women (7.71 mm2 [7.01–8.42]). Eighteen studies reported CSA values at the proximal carpal tunnel stratified by hand dominance and 16 studies reported values based on laterality of right versus left wrist (see Figure 5). The weighted averages were nearly identical with no significant differences between nerves measured in a dominant wrist (8.51 mm2 [7.72–9.29]) and a non-dominant wrist (8.57 mm2 [7.62–9.52]), and in nerves measured in the right (7.71 mm2 [7.03–8.40]) versus left wrist (7.93 mm2 [7.46–8.76]). Similarly, there was no significant difference (P = .81) among eleven studies that reported laterality for CSA of the median nerve in the proximal formal between the right (6.92 mm2 [6.30–7.54]) and left (6.87 mm2 [6.49–7.26]).
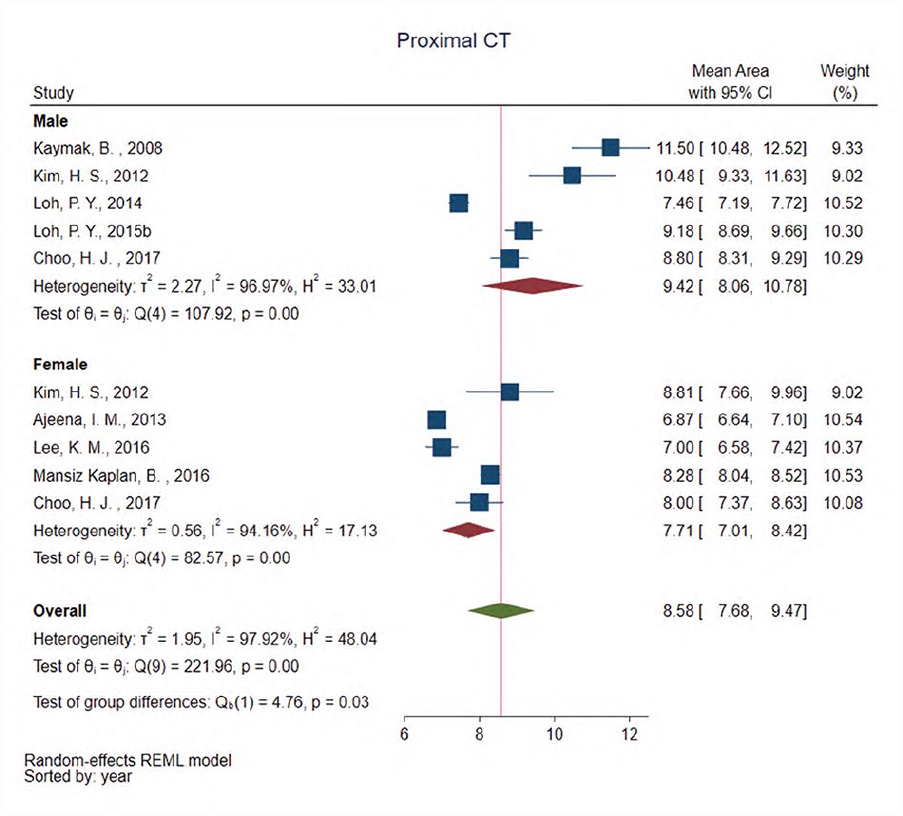
Forest plots showing group differences for weighted averages of median nerve cross-sectional area (CSA) in the proximal carpal tunnel (CT) among studies that provided data stratified by sex demonstrating significantly larger CSA (P = .03) in men (9.42 mm2) than in women (8.58 mm2). CI, confidence interval.
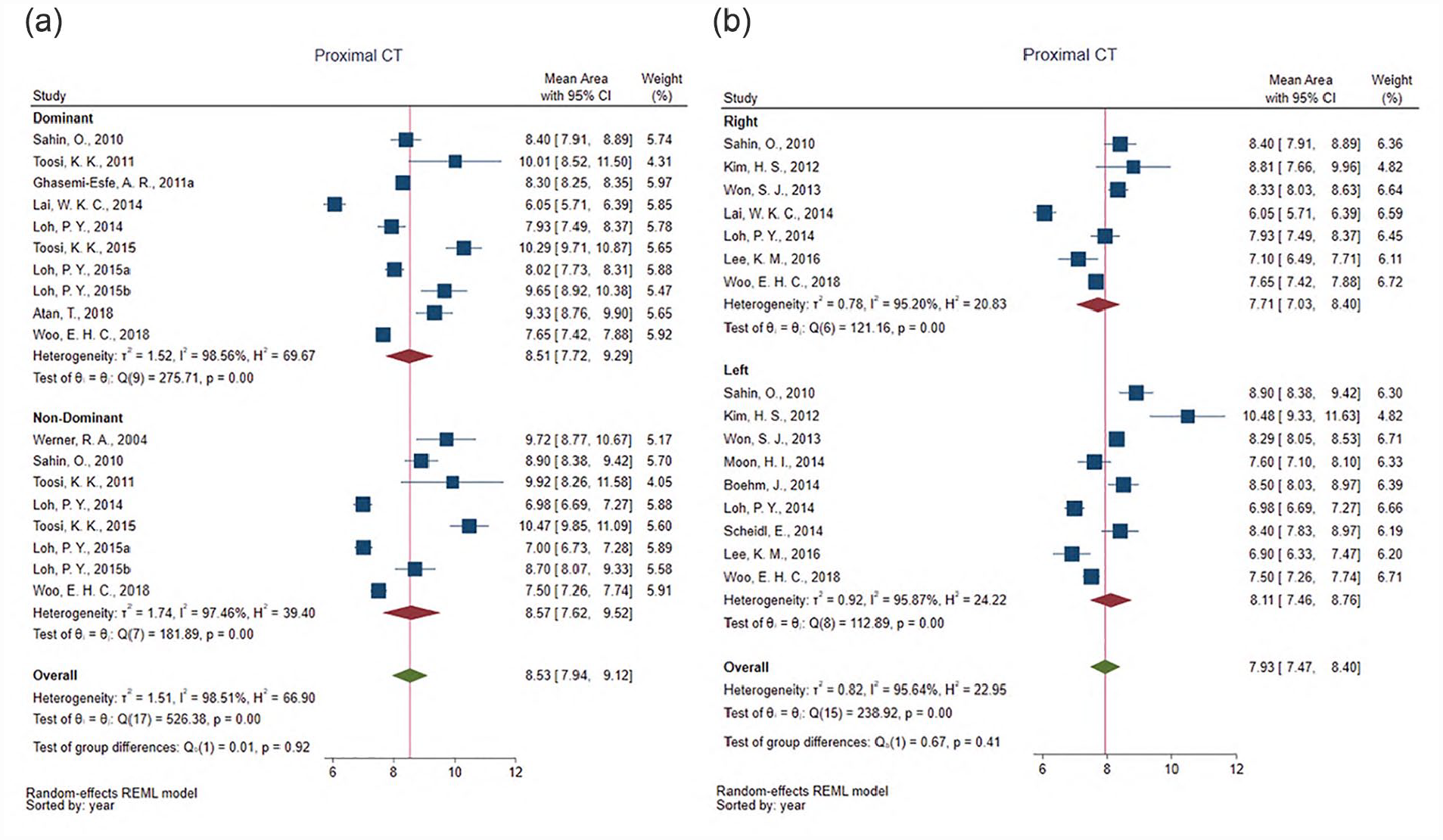
Forest plots showing group differences for weighted averages of median nerve cross-sectional area (CSA) in the proximal carpal tunnel (CT) among studies that provided data stratified by hand dominance (a) or side (b) demonstrating no differences based on laterality (P = .92, P = .41). CI, confidence interval.
Discussion
Without accounting for age, sex, or laterality, healthy median nerve CSA values measured at the inlet to or in the proximal carpal tunnel all fall below the commonly used diagnostic threshold of 10 mm2 and are well below meta-analytic values reported for patients with various severities of CTS.5,92 Reference values for median nerve CSA in healthy individuals change slightly as the nerve travels from proximal to distal, being of similar size in the wrist and upper arm regions and slightly smaller in the forearm. Specifically, healthy median nerve CSA should be about 8.60 mm2 in the proximal carpal tunnel, approximately 2.0 mm2 larger than in the forearm with a wrist-to-forearm ratio of approximately 1.3. Although using either a difference of 2.0 mm2 or a wrist-to-forearm ratio of greater than 1.4 as suggested by commonly cited literature,93,94 these measures may lead to false positives and might be best considered as general “rules of thumb” rather than singular diagnostic threshold. That is, when considering CIs of healthy measures of the nerve between the proximal forearm and carpal tunnel, the potential difference in a healthy individual could be as large as 2.88 mm2 (i.e., 8.97–6.09 mm2) with a corresponding wrist-to-forearm ratio of 1.5. Definitive diagnosis of CTS may require adoption of these more conservative thresholds or a combination of multiple clinical measures.9,95
When accounting for linear changes by age, the estimated range of CSA within the carpal tunnel in healthy adults (18–65) is 7.83–9.24 mm2, falling well below a diagnostic threshold of 10 mm2. Given a small effect of age on CSA measures, adjusting normative values is only necessary when evaluating pediatric or older adults; however, sex and laterality may require attention in clinical practice and research. Although there were no differences in median nerve CSA when considering percent male versus female across 47 studies, among 10 studies that exclusively stratified data by sex, men had significantly larger CSA than women. Given that these studies had the same weighted average as the full sample when compiling men and women together, research with mixed-sex samples could confidently use 8.60 mm2 as a valid reference for median nerve CSA at the level of the pisiform. Alternatively, for studies with higher representation of men or women and for individual patients, researchers or clinicians should consider using the sex-normed reference values of 7.71 mm2 for women and 9.42 mm2 for men. Importantly, caution should be used when applying the diagnostic threshold of 10.0 mm2 in men as the upper limit of the 95% CI for male CSA surpasses this threshold in the aggregate data within this meta-analysis.
In healthy individuals, median nerve CSA in the proximal carpal tunnel is likely highly similar between dominant and non-dominant sides. Thus, studies that consider bilateral CSA as independent data points could have increased risk of erroneous statistical findings. Alternatively, accounting for within-subject differences between wrists as a diagnostic assessment may have significant validity. Current primary sonographic diagnostic criteria for CTS rely on an absolute threshold (i.e., 10.0 mm2) or a within-arm comparison (e.g., wrist-to-forearm ratio). Adding a bilateral comparison criterion would mirror electrodiagnostic approaches that consider bilateral differences in conduction velocities along with an absolute threshold and a within-arm comparison with the ulnar nerve.
Methodological concerns require attention to improve rigor in the clinical or research use of median nerve CSA measurements. One previously identified issue that remains pervasive is the wide variability how anatomical locations of CSA measurements are identified and described. 6 Two issues arose in attempting to categorize study findings using the heterogeneous descriptions across the studies. First, the same term was often used to represent different anatomical regions, such as the word “inlet” used to indicate a location immediately proximal to the carpal ligament in some studies and a location under the most proximal portion of the carpal ligament in other studies. Second, there was variability in how much detail was used to describe where a measure was taken and disparate use of surface landmarks versus sonographically identified anatomical landmarks to identify the measurement location. For example, the “carpal tunnel inlet” was sometimes mentioned as generally being measured from an image taken at the wrist crease, while measurements in the proximal forearm were sometimes completed at a specific distance from the elbow or wrist and other times completed at the location where the nerve emerged between the heads of the pronator teres muscle. The only consistent description noted across the studies was using the pisiform as a landmark for measuring the median nerve in the proximal carpal tunnel. Developing additional standardized nomenclature that avoids gross, external landmarks and uses clear sonographic anatomical landmarks for the acquisition and analysis of median nerve CSA will improve clarity across research studies and consistency in clinical diagnostics.
In addition to adopting standardized nomenclature, there is a significant need for studies to clearly describe how individual patients versus individual wrists are included or excluded from final data samples. It was often challenging to determine whether one or both wrists were included among individual participants and even more challenging to know when or why data from some wrists were either not collected or were excluded when the number of wrists was not equal between sides or did not match the total number of participants in the sample. Importantly, if both wrists of an individual participant are included, data from this meta-analysis suggest a need to account for the dependent nature of nerves when conducting within-subject analyses. Finally, although most studies now measure CSA using a direct trace within the hyperechoic epineurium, multiple studies were eliminated due to measurement using less sensitivity or accurate techniques (e.g., ellipse).
Limitations
The reliance on reported summary data rather than using primary data, combined with inconsistencies in reporting of methodological details across studies introduces some error in the meta-analytic means. First, individual studies obtained and reported data either by individual or by wrist, and it was often unclear when data were from left or right wrists, from dominant or non-dominant sides, or averaged across a mixture of both upper extremities. Furthermore, some studies reported inconsistencies between the number of included wrists or individuals and the final sample size used in the analysis. Second, despite efforts to obtain missing data, many studies were excluded, and inconsistent reporting of race and ethnicity resulted in the inability to examine CSA based on these factors. Finally, definitions of “healthy” varied greatly across studies or were generally undefined, which potentially resulted in inclusion of some data from individuals with pathologies. Despite these limitations, consistency of CSA means within similar ranges across the included studies increases confidence in reporting the meta-analytic averages as normative reference values within the general population.
Conclusion
Using data from 73 studies, normative reference values for the CSA of the median nerve in healthy individuals were identified. The reference value for the most common measurement site within the carpal tunnel at the level of the pisiform is 8.60 mm2. Adjustment for age in a clinical setting or age-matching in research samples may only be necessary when examining pediatric or older adult patients. Men generally have larger CSA in the proximal carpal tunnel than women, and caution is required when applying a diagnostic threshold of 10.0 mm2 for male patients as the upper limit of normative averages surpasses this threshold. Finally, evidence of no difference between dominant and non-dominant wrists is important. Researchers should avoid considering bilateral CSA measures from one individual as independent data points, while within-patient differences between wrists may be useful as a clinical diagnostic assessment. In addition to normative values, this meta-analysis illuminated numerous issues in the quality of study reporting, variations in the use of anatomical landmarks, and a lack of standard nomenclature.
Supplemental Material
sj-docx-2-jdm-10.1177_87564793231176009 – Supplemental material for Sonographic Reference Values for Median Nerve Cross-sectional Area: A Meta-analysis of Data From Healthy Individuals
Supplemental material, sj-docx-2-jdm-10.1177_87564793231176009 for Sonographic Reference Values for Median Nerve Cross-sectional Area: A Meta-analysis of Data From Healthy Individuals by Shawn C. Roll, Sandy C. Takata, Buwen Yao, Lynn Kysh and Wendy J. Mack in Journal of Diagnostic Medical Sonography
Supplemental Material
sj-docx-3-jdm-10.1177_87564793231176009 – Supplemental material for Sonographic Reference Values for Median Nerve Cross-sectional Area: A Meta-analysis of Data From Healthy Individuals
Supplemental material, sj-docx-3-jdm-10.1177_87564793231176009 for Sonographic Reference Values for Median Nerve Cross-sectional Area: A Meta-analysis of Data From Healthy Individuals by Shawn C. Roll, Sandy C. Takata, Buwen Yao, Lynn Kysh and Wendy J. Mack in Journal of Diagnostic Medical Sonography
Supplemental Material
sj-pdf-1-jdm-10.1177_87564793231176009 – Supplemental material for Sonographic Reference Values for Median Nerve Cross-sectional Area: A Meta-analysis of Data From Healthy Individuals
Supplemental material, sj-pdf-1-jdm-10.1177_87564793231176009 for Sonographic Reference Values for Median Nerve Cross-sectional Area: A Meta-analysis of Data From Healthy Individuals by Shawn C. Roll, Sandy C. Takata, Buwen Yao, Lynn Kysh and Wendy J. Mack in Journal of Diagnostic Medical Sonography
Footnotes
Acknowledgements
The authors would like to acknowledge the assistance in reviewing abstracts and studies provided by Joyce Ho and Nina Wakayama.
Key Takeaways
A healthy median nerve cross-sectional area reference at the pisiform is 8.60 mm2. Age adjustments for median nerve reference values are not indicated in adults. Healthy men have larger nerves that may exceed common diagnostic thresholds. Healthy nerves do not differ in size between wrists. Differences in nerve area between wrists may be a viable diagnostic indicator.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by grant number R01 OH010665 from the Centers for Disease Control and Prevention (CDC), National Institute for Occupational Safety and Health, and by grant number F31 AR074894 from the National Institutes of Health (NIH), National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS). The content is solely the responsibility of the authors and does not necessarily represent the official views of the CDC or the NIH.
Peer Reviewer Guarantee Statement
The Editor/Associate Editor of JDMS is an author of this article; therefore, the peer review process was managed by alternative members of the Board and the submitting Editor/Associate Editor had no involvement in the decision-making process.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.