
Abstract
Appendicitis is a common pathology most often caused by an appendicolith. Laparoscopic appendectomy has become the standard operative approach, but it has a higher risk of retained appendicoliths than open laparotomies. This report describes a case of a perihepatic abscess due to a retained appendicolith following laparoscopic intervention. The abscess was successfully drained and the appendicolith retrieved percutaneously under fluoroscopic guidance. A literature review and discussion about retained appendicoliths are provided as points for diagnostic consideration.
Acute appendicitis occurs in up to 7% of the US population during their lifetime and presents most commonly in 10- to 20-year-old males. 1 It is usually caused by obstruction secondary to an appendicolith but may also be due to lymphoid hyperplasia or adhesional bands. Obstruction causes high intraluminal and intramural pressures, which impair venous and lymphatic drainage. This leads to edematous ulcerated mucosa that becomes infected, ischemic, and ultimately necrotic.2,3
Laparoscopic appendectomy has become the standard approach to treat acute appendicitis, as it results in faster recovery, less pain, and fewer wound complications than open laparotomies. However, it carries an increased risk of stump appendicitis and retained appendicoliths when compared with open approaches. 2 The present case describes a patient who developed a perihepatic abscess secondary to a retained appendicolith. The abscess was successfully drained and the appendicolith retrieved percutaneously under fluoroscopic guidance with a basket.
Case Report
A previously healthy 24-year-old man was admitted with pain rated eight out of ten in the right lower quadrant and epigastric pain that suddenly occurred 2 days prior. He was diffusely tender to palpation, particularly in the right lower quadrant; he was also febrile and had a white blood cell count of 16 600 per mm3. A computed tomography (CT) scan of the abdomen and pelvis showed an enlarged and inflamed appendix with two fecaliths at the orifice and small foci of free air in the upper abdomen, consistent with a perforated appendix.
Antibiotics were started, and a laparoscopic appendectomy was performed. Over the next few days, his white blood cell count normalized, but he continued to remain febrile. A repeat CT scan on postoperative day 5 demonstrated four abscesses, all too small to drain, and a retained 8-mm calcific body between segment 8 of the liver and the abdominal wall, most suggestive of a retained appendicolith. Given the small size of the intra-abdominal abscesses, commonly associated with surgical intervention for perforated appendicitis, the patient was discharged on a 14-day course of antibiotics.
Three months later, he returned with sharp pain, rating five out of ten in the right upper quadrant, and with high-grade fever and a positive Murphy sign. A sonogram revealed a complex perihepatic fluid collection with no internal vascularity, as well as a 10-mm calcification consistent with an appendicolith adjacent to segment 5 of the right hepatic lobe (Figure 1). Power Doppler displayed enhanced hepatic flow around the collection, no internal vascularity, and multiple high-amplitude linear echoes within the fluid (Figure 2). The sonographic artifacts are most consistent with gas bubbles within an abscess. Given his history and prior CT scan, this was concerning for a perihepatic abscess containing an appendicolith. A contrast-enhanced CT scan of the abdomen and pelvis confirmed the abscess containing an appendicolith (Figure 3) and internal gas bubbles (Figure 4).
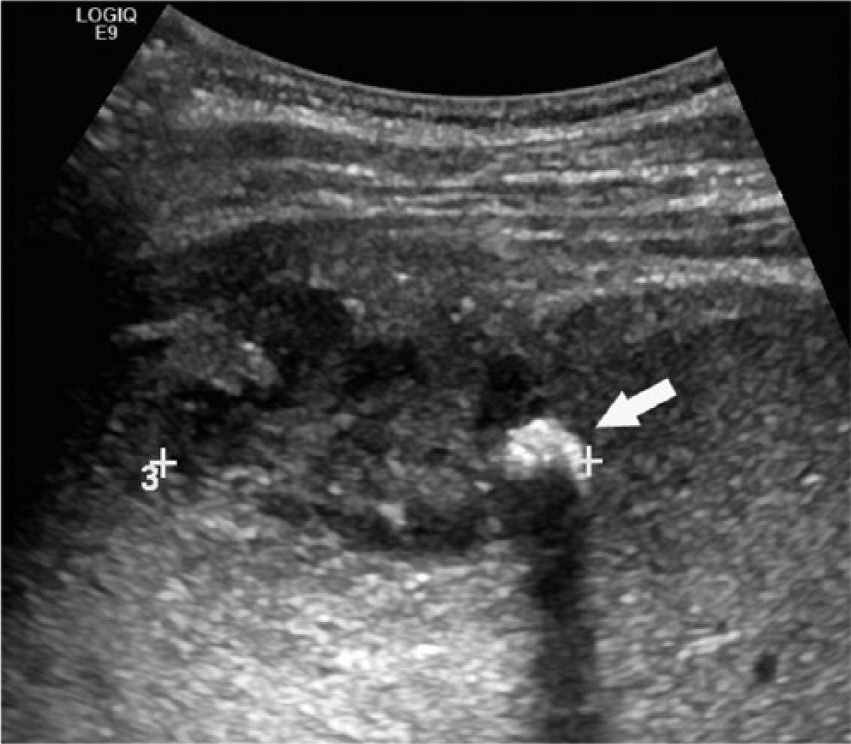
Transverse gray-scale ultrasound demonstrating complex perihepatic fluid collection containing a shadowing calcification (arrow) consistent with a retained appendicolith within an abscess.
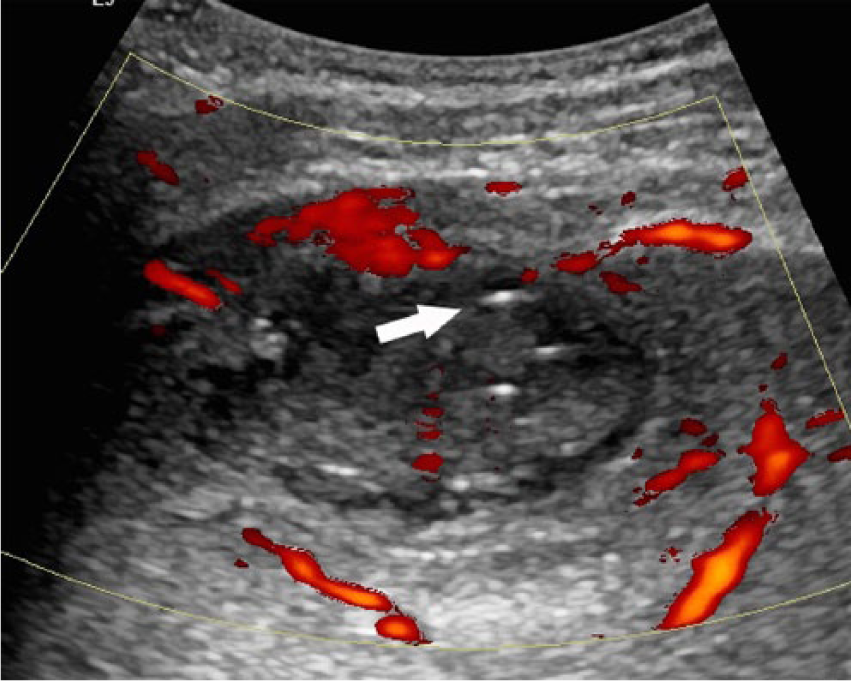
Transverse power Doppler image showing increased hepatic flow around the collection, no internal vascularity within the fluid, and linear high-amplitude echoes (arrow) consistent with gas bubbles within the abscess.
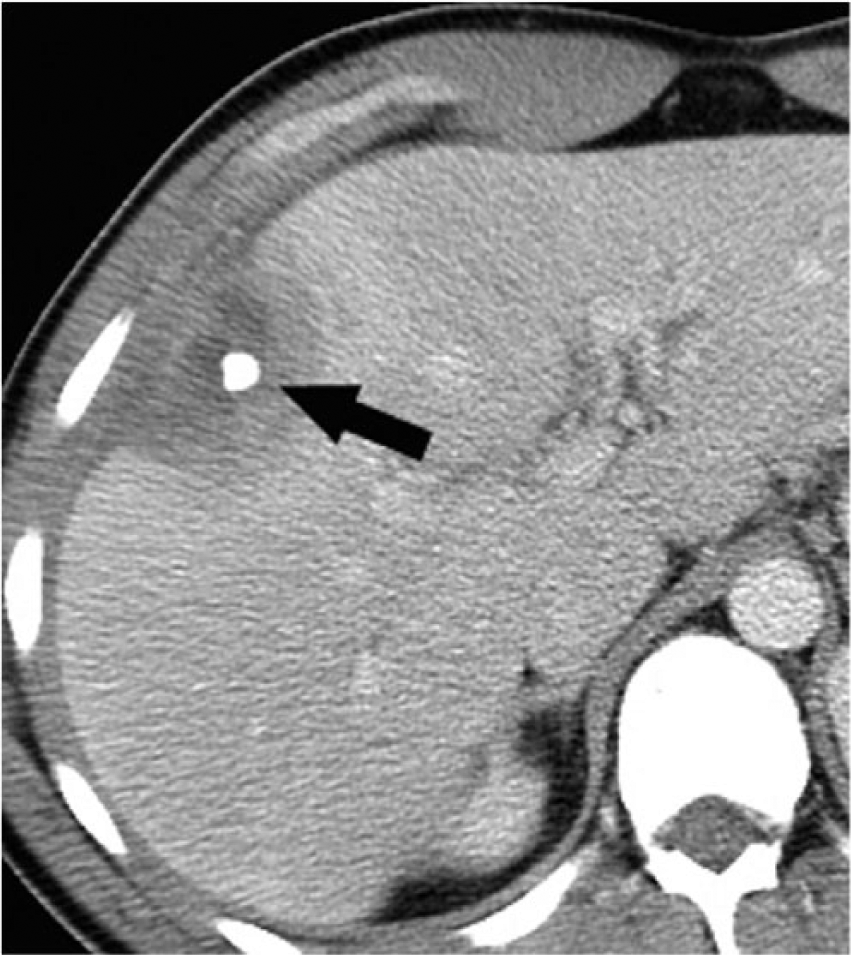
Contrast-enhanced CT scan demonstrating the appendicolith (arrow).

Contrast-enhanced CT scan showing the gas bubbles (arrow) within the perihepatic abscess.
The patient was started on antibiotics, and an interventional radiologist placed a pigtail catheter. A week later, the interventional radiologist removed the appendicolith percutaneously. Initially, an abscessogram was performed by injecting dilute contrast into the existing abscess drain. Under fluoroscopic guidance, a micropuncture set was advanced toward the appendicolith, and a short guidewire was coiled in the abscess cavity. Serial dilation was performed over the wire until a 24F sheath could be accommodated. A basket was then advanced through a 12F sheath coaxially through the 24F sheath (Figure 5), and the appendicolith was successfully retrieved. Contrast was gently injected through the existing drain to confirm that no other stones were present; the drain was left in place.
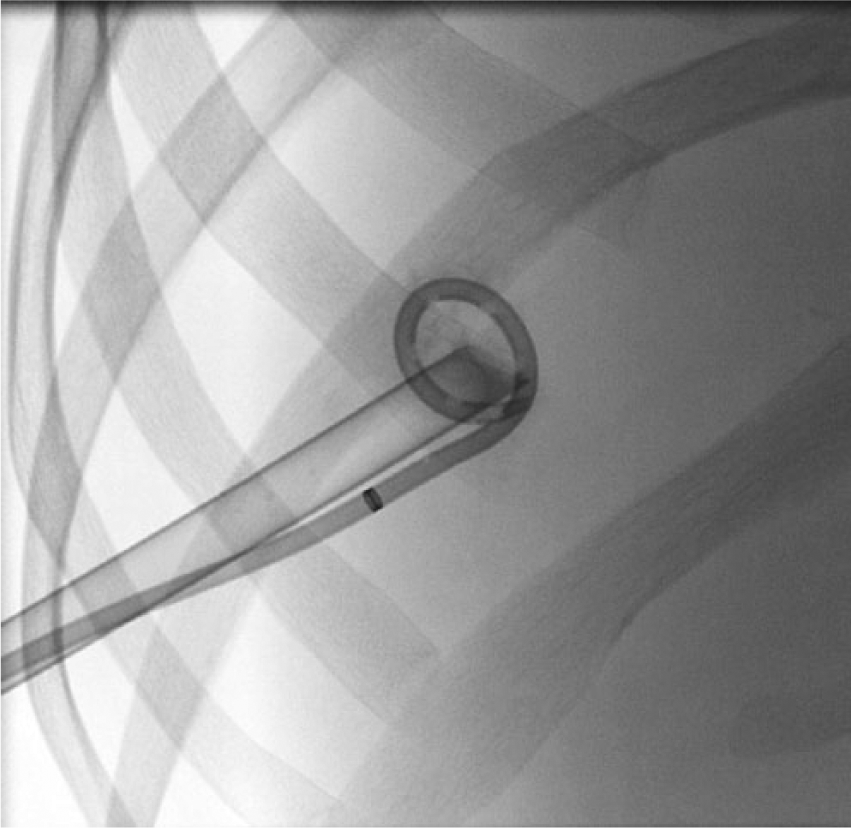
Fluoroscopic image showing a percutaneous pigtail catheter in the abscess cavity, as well as the Wittich tube for the appendicolith removal.
The same day, a chest radiograph revealed large right pleural effusion tracking up to the apex, and an interventional radiologist placed a pigtail pleural catheter. The following day, a CT scan of the chest showed right multiloculated exudative pleural effusion causing significant collapse of the right lower lobe and thickening and enhancement of the pleura. The collection was determined to be undrainable via percutaneous drainage. The patient was subsequently taken to the operating room for right-sided video-assisted thoracoscopic surgery that converted to a thoracotomy with decortication after the thick gelatinous material could not be evacuated. Chest tubes were placed, which were subsequently removed over the next few days, along with the perihepatic drain. A contrast-enhanced CT displayed resolution of the abscess cavity.
Discussion
Extraluminal appendicoliths may result from appendiceal perforation or may spill intraoperatively. In either case, they are more easily missed during laparoscopic techniques. Appendicoliths are pathologically evident in up to a third of cases in adults, but they are radiologically evident in only about 10% of cases. 2 Rates of detection preoperatively have increased as CT and sonography have gained popularity. Fecaliths are composed of fecal material and calcium, and they serve as a focal site for infection. 4 In contrast, gallstones dropped during laparoscopic cholecystectomy are less commonly associated with intra-abdominal abscess formation, as they tend to be sterile. 3
Abscesses secondary to retained appendicoliths are most commonly found in the paracecal region, but they have also been reported in the pouch of Douglas, rectovesical pouch, fallopian tube, iliopsoas, and gluteal region, as well as perihepatically. 5 No other cases of a perihepatic abscess caused by fecalith erosion into the liver appear to have been reported. The time from appendectomy to abscess formation ranges from 2 months to 4 years. 2 Thus, an abscess secondary to a dropped appendicolith could be considered even in individuals with a remote history of an appendectomy if the clinical presentation and imaging are consistent with such a scenario.
On sonography, an intra-abdominal abscess is visualized as complex fluid collection with internal echoes. Gas bubbles, if present, appear as high-amplitude linear echoes with reverberation artifacts, and an appendicolith appears as a shadowing calcification within the fluid collection. 6 On power Doppler, the periphery is hypervascular, whereas the center is avascular. On CT, an abscess is seen as a hypodense complex fluid collection that may also have internal gas bubbles, exert a mass effect, and display rim enhancement with contrast. 6 A calcification within the fluid collection in the setting of a prior appendectomy should suggest an associated appendicolith. The sensitivities and specificities of detecting an intra-abdominal abscess with sonography are 71% to 93% and 87% to 99%, respectively, and with CT are 95% to 97% and 95%, respectively. 7 The differential diagnosis of an abscess is based on the location in the abdomen. In terms of perihepatic abscesses, the differential includes other causes of abscess, such as rupture of an infected biliary tree or liver abscess, a hematoma, a biloma, or metastasis on the hepatic surface.
If retained during surgery, appendicoliths are known to cause recurrent postoperative abscesses in virtually all cases if not removed. Thus, antibiotics and, generally, abscess drainage, along with appendicolith extraction, are the definitive treatment. Extraction has been performed via open, laparoscopic, and percutaneous approaches.1,4,8-12 Appendicoliths are often difficult to locate during surgery because they are small, often migrate to inaccessible recesses, and can form necrotic tissue with associated adhesions. 9 Various techniques have been used to locate appendicoliths intraoperatively, including fluoroscopy with or without endoscopic techniques, 10 laparoscopic ultrasound probes inserted into a port, 9 and preoperative CT-guided hookwire placement. 11
There have been only 2 other case reports demonstrating the feasibility and effectiveness of percutaneous removal of retained appendicoliths.4,10 In the case described, the interventional radiologists successfully retrieved the appendicolith under fluoroscopic guidance with a basket. Rasuli et al. extracted a pelvic fecalith using a similar technique, but they required a flexible cystoscope in addition to fluoroscopy because the appendicolith was not radiopaque enough to visualize with fluoroscopy alone. 10 Given the less invasive nature and lower cost of percutaneous removal, it is the optimal approach for appendicolith removal. However, the appropriate strategy must be planned with consideration of the appendicolith location, the ability to visualize it with the various imaging modalities, the available equipment, and the skill of the interventional radiologists and surgeons. Full resolution of the abscess without recurrence occurs in all cases, provided that appendicoliths are removed and the abscess is drained.
Conclusion
Retained appendicoliths, although rare, can cause recurrent abscesses if not removed. As the prevention of retained appendicoliths is preferable, every effort should be made to avoid this complication. Therefore, it is important that radiologists communicate the presence of any appendicoliths on preoperative imaging so that the surgeon may verify their removal intraoperatively prior to closure. Likewise, the presence of fecaliths on postoperative imaging should prompt communication with the surgeons so that extraction may be planned prior to discharge. Percutaneous removal of appendicoliths is the least invasive method of retrieval and has been performed successfully, but the appropriate strategy must be made on a case-by-case basis.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.