
Abstract
The prevalence of segmental testicular infarction is extremely uncommon and very few cases have been reported in literature. Clinical and sonographic presentation of this condition can mimic testicular neoplasms or testicular torsion. Therefore, accurate diagnosis of segmental testicular infarction is imperative in the treatment process. This case study presents the sonographic diagnosis of testicular infarction in a 49-year-old man who reported mild testicular tenderness. A conservative treatment approach was used, saving the patient unnecessary surgical intervention.
Global testicular torsion is a common finding in acute scrotal pain and is considered a urologic emergency. 1 Segmental testicular infarction is a localized area of ischemia. It has a rare incidence that usually occurs in patients in the second and fourth decade of life and is idiopathic in most cases. 1 There have been less than 70 cases of segmental testicular infarction reported since 1909. Acute scrotal pain and swelling are the most common clinical symptoms, and sonography is the primary imaging modality used to evaluate for testicular pathology. Differential diagnoses for segmental testicular infarction include testicular seminomas and testicular torsion. Sonography can aid in correctly diagnosing segmental infarction and can prevent unnecessary treatment such as surgical intervention.
Case Report
A 49-year-old man presented to an outpatient clinic with complaints of a “high riding” right testicle and mild testicular tenderness. He had a history of a cadaveric renal transplant 2 weeks prior and a remote history of a vasectomy. The testicle was nontender without evidence of masses or ecchymosis on physical examination. The patient denied signs of fever, chills, hematuria, dysuria, or abdominal pain. He was then referred for a sonogram where a Philips iU-22 ultrasound equipment system (Philips Medical, Bothell, WA) was used with a L12-5 MHz linear-array transducer.
An initial sonogram showed a hypoechoic, avascular area in the right upper pole suggesting concerns for segmental testicular infarction in the setting of acute pain (Figure 1A and 1B). The lower pole of the right testicle demonstrated normal arterial and venous flow. The left testicle demonstrated normal homogenous echogenicity and was unremarkable (Figure 2). The radiologist recommended a follow-up testicular sonogram in 4 to 6 weeks to ensure resolution.
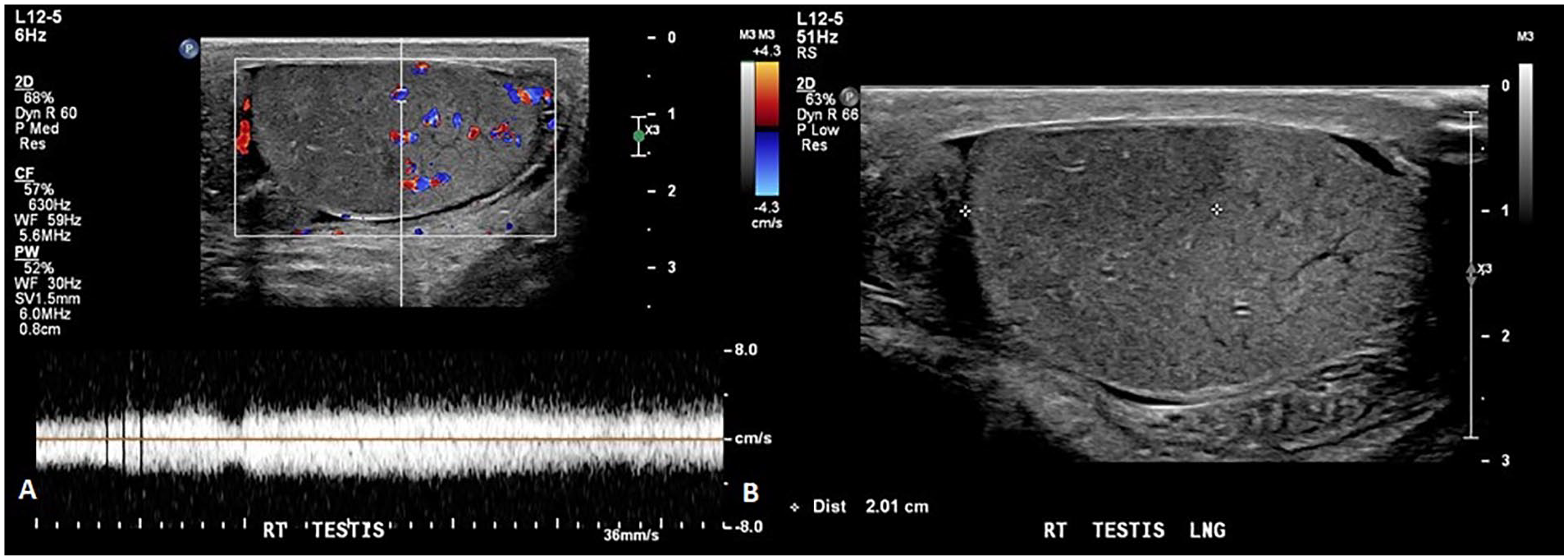
(A) Longitudinal sonographic image of the right testis with color and pulsed wave Doppler demonstrated peripheral flow to the avascular region. (B) Longitudinal gray-scale sonographic image of the right testis which shows a measurement of the hypoechoic region.
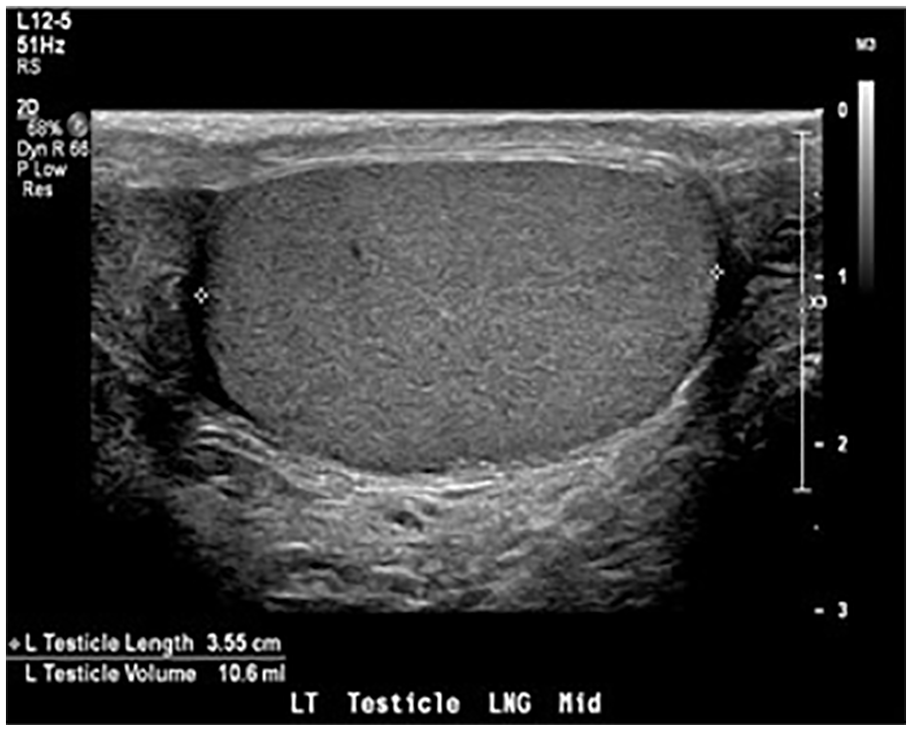
Longitudinal sonographic image of the left testis demonstrated a normal homogenous echogenicity.
The patient returned 2 weeks later for a clinic visit with complaints of tightness in his right groin and still denied clinical signs of infection. The follow-up sonogram re-demonstrated the avascular hypoechogenicity in the upper pole of the right testicle with a decrease in the right testicular length, suggesting a maturing segmental infarct (Figure 3). Once again, the lower pole of the right testicle demonstrated normal arterial and venous flow. An infiltrative testicular neoplasm was considered, although unlikely due to the clinical history, but not entirely excluded. Therefore, another follow-up sonogram in 3 months was recommended to again assess for the expected evolution of the suspected testicular infarct.
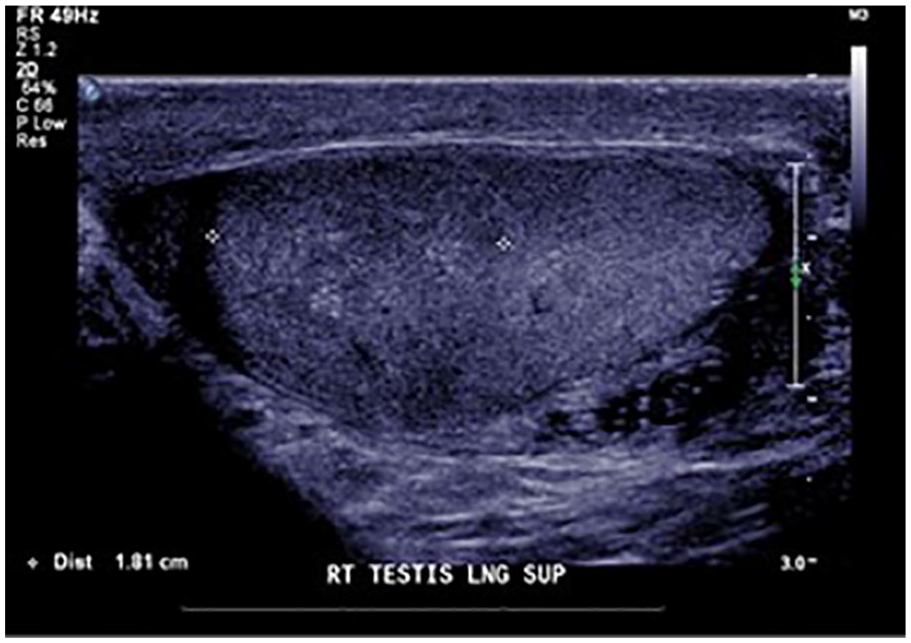
Follow-up gray-scale sonographic image indicated a decreased size in the avascular, hypoechoic region.
The patient returned for a 3-month follow-up clinic visit and stated the testicular pain had resolved. A final sonogram once again re-demonstrated the avascular hypoechogenicity in the upper pole of the right testicle and a decrease in size compared with the prior examination (Figure 4). The right testicle demonstrated normal arterial and venous flow in the lower pole. The findings were consistent with a maturing segmental infarct of the testicle.
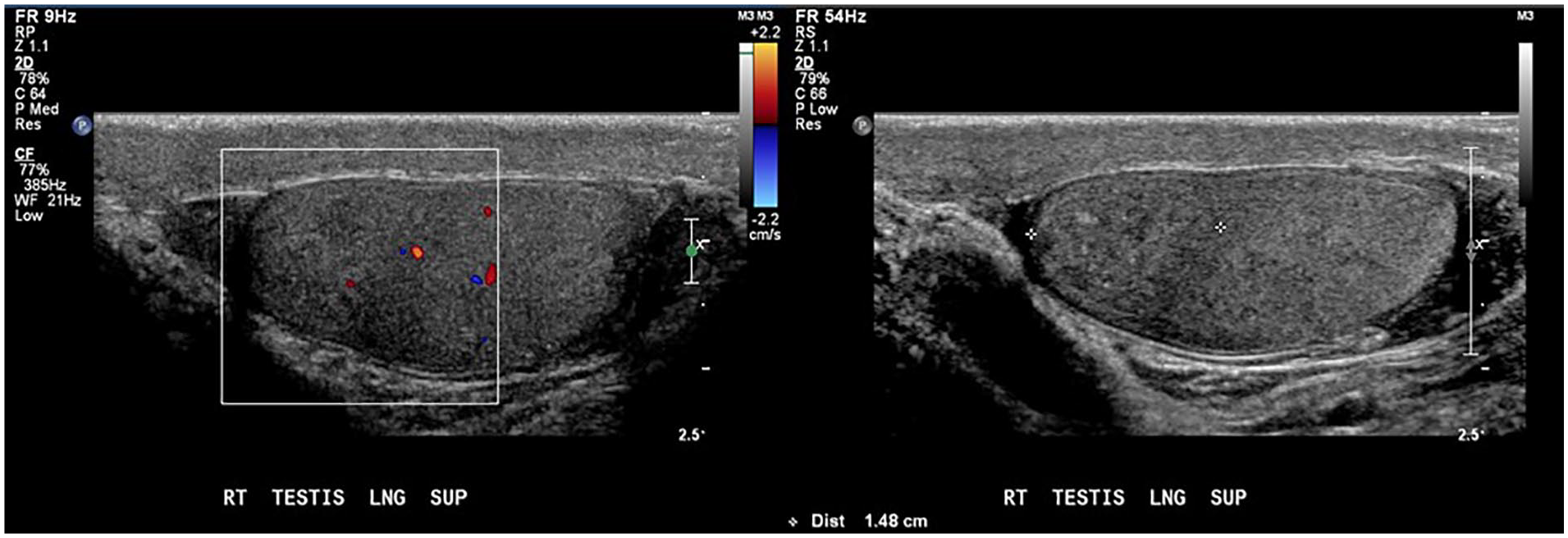
Final sonogram showed a decreased size of the avascular, hypoechoic mass in the superior pole of the right testis compared with the prior examination.
Discussion
Diagnostic sonography is the best modality to evaluate acute scrotal pain. 2 It is considered a safe imaging modality due to the low risk of biological effects compared with other imaging choices. Gray-scale sonographic images of the testicles evaluate the parenchyma, echogenicity, size, and symmetry. A normal testicle appears as a homogenous ovoid structure that approximately measures 5 cm × 3 cm × 2 cm (length × height × width). 3 Doppler sonography can accurately evaluate blood flow within the testicle that can be useful in differentiating testicular pathologies. The testicle has a triple blood supply consisting of the abdominal aorta (through the internal spermatic artery), the cremasteric artery, and the artery of the ductus deferens. 4 A normal testicular artery has a low-resistance waveform with resistive indices (RIs) from 0.48 to 0.75. 2 Venous flow has a continuous spectral Doppler waveform with a low velocity. 3
Segmental testicular infarction is a localized area of infarction in the testis. The prevalence of segmental testicular infarction is particularly rare. 1 In 70% of cases, the condition is usually idiopathic and affects patients between the second and fourth decades of life. The pathophysiology of segmental testicular infarction has not been fully understood; however, it has been hypothesized that the segmental portion of the testicle can functionally act as an end-organ. 4 An infarction may occur if the blood flow through the segmental artery is interrupted, and there is inadequate collateral blood supply. Segmental infarction can occur after testicular torsion, trauma, bacterial endocarditis, epididymo-orchitis, vasculitis, leukemia, or hypercoagulable states. Patients usually clinically present with acute scrotal pain and swelling; however, some studies have found that these symptoms may be variable or absent. 5 Physical examinations of the testis are typically normal without a palpable mass. Sonography of the testicles using color and pulsed wave Doppler is important for making a diagnosis of segmental infarctions. Depending on the age of infarction, a focal, wedge-shaped, or round hypoechoic mass is most commonly visualized. A case study completed by Madaan et al showed an avascular, hypoechoic lesion in 74% of cases with segmental testicular infarction. 6 Over time, the area of infarction decreases in size and may become hyperechoic. Color Doppler will show reduced or absent flow within the area of infarction. 5 There is a broad spectrum of testicular pathologies that share similar clinical symptoms making segmental testicular infarction difficult to distinguish from other findings. Because the sonographic presentation of testicular masses or testicular torsion are similar, these are the two most common differential diagnoses. Due to the inability to definitively diagnose segmental testicular infarction, surgical exploration is often used and results in a partial or complete orchiectomy. Thus, it is important to differentiate between the different pathologies to prevent unnecessary treatment options.
Testicular seminomas are the most common type of malignant testicular tumors and account for 55% of cases. Seminomas typically affect men between the third and fifth decade of life. 7 As the primary treatment method for testicular seminomas is a radical inguinal orchiectomy, it is important that an accurate diagnosis is made. Patients with a seminoma clinically present with a unilateral, slow-growing, painless, palpable mass while segmental infarctions present with pain. Therefore, the clinical presentation can also differentiate these two pathologies. Sonographically, seminomas are solid, homogenous, and hypoechoic, similar to the appearance of a segmental testicular infarction. Color Doppler is a useful tool to differentiate between these two pathologies. With color Doppler, seminomas will show an increase in internal vascularity compared with the rest of the testicle. 7 Serial follow-up sonograms may be useful in distinguishing between the two lesions. In addition, unlike a segmental infarction, a seminoma will gradually increase in size.
The incidence of testicular torsion is 1 in 4000 male patients under 25 years of age. It occurs when the spermatic cord twists and obstructs the blood supply to the entire testicle requiring imperative intervention to prevent radical orchiectomy and infertility. Manual detorsion can treat testicular torsion if detected within 6 hours of onset symptoms; however, evaluation of blood flow must be evaluated to confirm the restoration of blood flow. 2 An orchiopexy is the most common treatment for testicular torsion. 3 Patients clinically present with sharp and acute scrotal pain. Evaluating testicular torsion sonographically varies depending on the time frame of the incident. In the early phase, the testis will be normal in echogenicity and become hypoechoic after 4 to 6 hours. 2 Secondary to infarction, the testicles become heterogenous. It is crucial to evaluate venous flow since venous flow is obstructed first in torsion. 2 Color Doppler will show decreased or absent flow within the entire testicle. The diastolic component of arterial flow may also be reversed. Furthermore, identification of a sonographic “whirlpool sign” can add to a more definite diagnosis. The whirlpool sign is reported to be the most specific and sensitive sign of torsion. 2 This is seen as an enlarged twisted spermatic cord superior to the symptomatic testis. The sensitivity of color Doppler to testicular torsion in the adult population is 80% to 98% with a specificity of 97% to 100%. 2 Carefully investigating the color Doppler and spectral waveforms of the testicle can aid in diagnosis along with the presenting symptoms. If the entire testicle is affected, segmental infarction can be ruled out.
There is a large controversy regarding the course of management for segmental testicular infarction. Radical orchiectomy is performed in most cases where segmental testicular infarction is suspected. However, there have been many proposals recommending a more conservative management strategy. 1 In a case study performed by Madaan et al, 16 out of 19 patients with segmental testicular infarction were successfully managed by careful observation for 6 to 12 weeks. 6 After the follow-up period, the patients had no symptoms and sonographically showed maturing of the infarct. If a conservative approach is used, clinical and sonographic follow-up are necessary to rule out other pathologies and to ensure resolution of symptoms.
Conclusion
Accurately identifying the clinical and sonographic differences of segmental testicular infarction, testicular torsion, and a testicular seminoma is crucial due to the different treatment options. Patients with segmental testicular infarction commonly present with acute scrotal pain and swelling. Sonographically, segmental testicular infarctions are focal, wedge-shaped or round hypoechoic, avascular masses. Surgical intervention can be avoided if segmental testicular infarction is diagnosed. In the present case, a conservative approach was used after sonography confirmed segmental testicular infarction and prevented unnecessary surgical intervention. Sonography is an important tool for identifying and aiding in an appropriate course of treatment options.