
Abstract
The objective of this study was to determine the sonographic patterns of the testes in patients with testicular torsion. Clinical data of 46 patients with testicular torsion confirmed by surgical exploration or manual detorsion were reviewed, and sonographic patterns of testicular torsion were categorized according to the sonographic characteristics of the testes, and their relation to the pathologic changes were analyzed. The sonographic appearances of testicular torsion were categorized into six patterns, reflecting pathologic changes of testicular torsion. Sonography of testicular torsion has different patterns, and recognition of these patterns may help the examiner establish a diagnosis and subsequently manage the patient.
Testicular torsion is an acute process within the scrotum requiring urgent management. Color Doppler sonography is the initial imaging study required because of its high sensitivity and specificity in the diagnosis.1–5 Color Doppler imaging demonstrating abnormal testicular perfusion aids in reaching a specific diagnosis of torsion.1–5 Grayscale sonography delineating the structural features of testicular torsion, including shape, size, echogenicity, and texture, allows meticulous interrogation of the testicular parenchyma.5–7 The aim of this study was to add to grayscale feature recognition of testicular torsion through lesion characterization.
Patients and Methods
Clinical data of 46 consecutive patients with acute-phase or late-phase testicular torsion from April 2005 to July 2010 were reviewed retrospectively; all cases were confirmed by surgical exploration or manual detorsion. Two experienced sonologists examined sonographic characteristics of the testes, including shape, echogenicity, texture, and distribution of echogenicities. The age of the patients ranged from 13 to 49 years, with a mean of 21 years. Acute-phase torsion was defined as <24 hours of pain and late-phase torsion as ≥24 hours of pain. 8 Sonologists with 7 to 23 years of experience performed the sonographic studies with Logiq 9 (GE Healthcare, Piscataway, New Jersey), HD 11 XE (Philips Healthcare Systems, Suzhou, China), Sequoia 512 (Siemens Acuson, Mountain View, California), and Mylab 15 (Esaote, Philipsweg, Maastrichet, the Netherlands) sonographic imaging systems with multifrequency linear array transducers (7–13 MHz). On color Doppler flow imaging (CDFI) and power Doppler imaging (PDI), the system was preset according to the built-in software for scrotum interrogation to detect low-velocity flow, allowing for optimal detection of slowly flowing blood in small testicular arteries. Color Doppler and power Doppler gain were adjusted to a proper level to avoid the appearance of artifacts. Shape, volume, echogenicity, texture, location, and blood flow were evaluated and compared with the contralateral testis and epididymis. Examination included first imaging the asymptomatic hemiscrotum and then the symptomatic side and spermatic cords, and then the scrotum was scanned longitudinally and transversely with grayscale sonography and CDFI and PDI, respectively.
The color Doppler sonographic diagnostic criterion for testicular torsion was that the vascularity of the symptomatic testis was absent or markedly reduced compared with the contralateral side, with or without enlargement of the epididymis, twist of the spermatic cord, and change of volume and echogenicity of the testis. The sonographic diagnostic criterion suggesting successful detorsion was the resumption of testicular blood flow, with or without recession of the swelling epididymis, and disappearance of the twist of the spermatic cord. All patients underwent follow-up at least once. The sonographic patterns of testicular torsion were classified according to the echogenicity (isoechoic, hypoechoic, marked hypoechoic, anechoic, or hyperechoic), texture (homogeneous or heterogeneous), and distribution of echogenicities.
Data Analysis
The duration time of testicular torsion among different patterns was compared using one-way analysis of variance (ANOVA), and percentile loss of testicular torsion between different patterns was compared using the chi-square test; a P value <.05 was considered statistically significant. The software used was SPSS (version 11.0; SPSS, Inc., an IBM Company, Chicago, Illinois).
Institutional review board consent for the study was obtained.
Results
The torsed testes were categorized into six patterns. All patterns lacked vascularity except pattern VI, and the patterns are described as follows and illustrated in Figures 1 to 6.
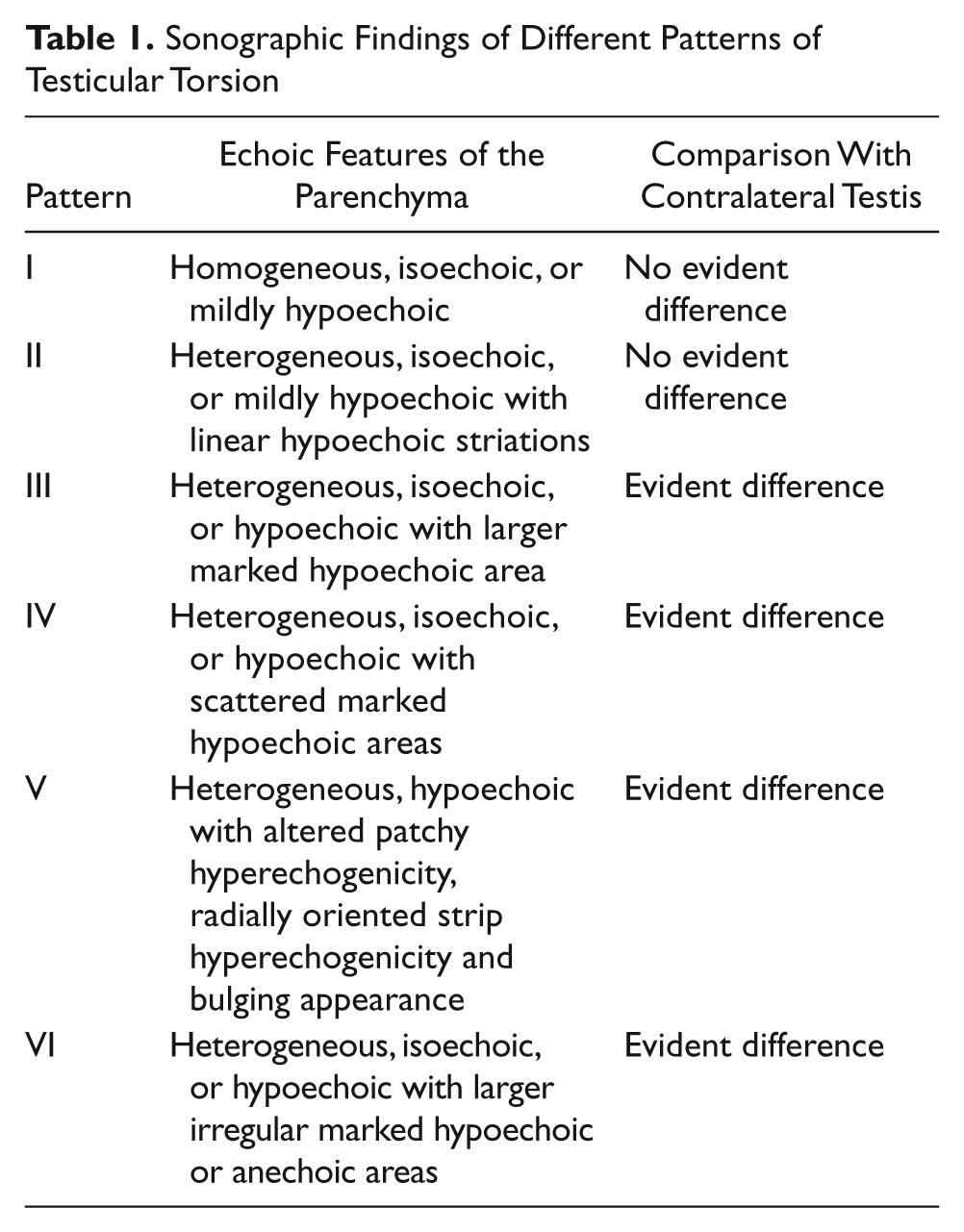
Pattern I: The volume of the symptomatic testis was equal to or slightly larger than the contralateral one, the parenchyma was homogeneous and isoechoic or mildly hypoechoic, and there was no evident difference compared with the contralateral side.
Pattern II: The volume of the symptomatic testis was equal to or slightly larger than the contralateral one, the parenchyma was heterogeneous and isoechoic or mildly hypoechoic with marked linear hypoechoic striations, and there was no evident difference compared with the contralateral side.
Pattern III: The volume of the symptomatic testis was equal to or slightly larger than the contralateral one, the parenchyma was heterogeneous and isoechoic or hypoechoic with a larger marked hypoechoic area, and there was an evident difference compared with the contralateral side.
Pattern IV: The volume of the symptomatic testis was slightly larger or smaller than the contralateral one, the parenchyma was heterogeneous and isoechoic or hypoechoic with scattered marked hypoechoic areas, and there was an evident difference compared with the contralateral side.
Pattern V: The volume of the symptomatic testis was equal to or slightly larger than the contralateral one; the parenchyma was heterogeneous and hypoechoic with altered patchy hyperechogenicity, radially oriented strip hyperechogenicity, and bulging appearance; and there was an evident difference compared with the contralateral side.
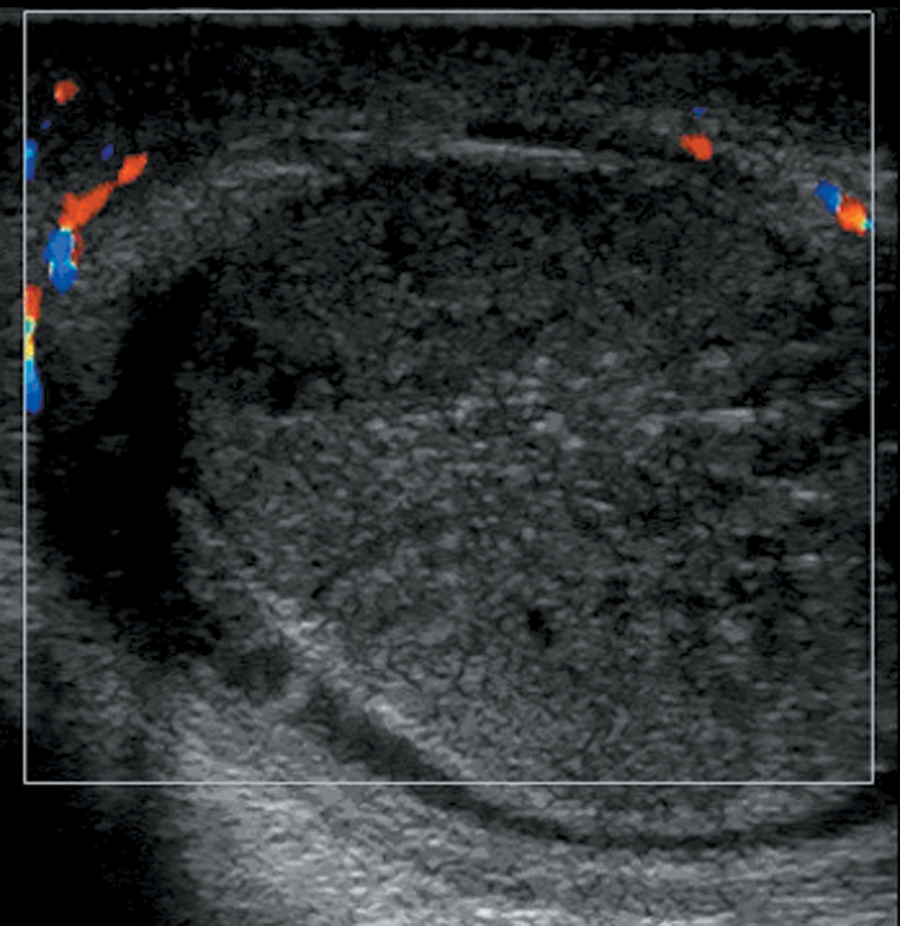
Pattern VI: The volume of the symptomatic testis was equal to or slightly larger than the contralateral one, the parenchyma was heterogeneous and isoechoic or hypoechoic with larger irregular marked hypoechoic or anechoic areas, CDFI and PDI demonstrated no vascularity or poor vascularity, and there was an evident difference compared with the contralateral side.
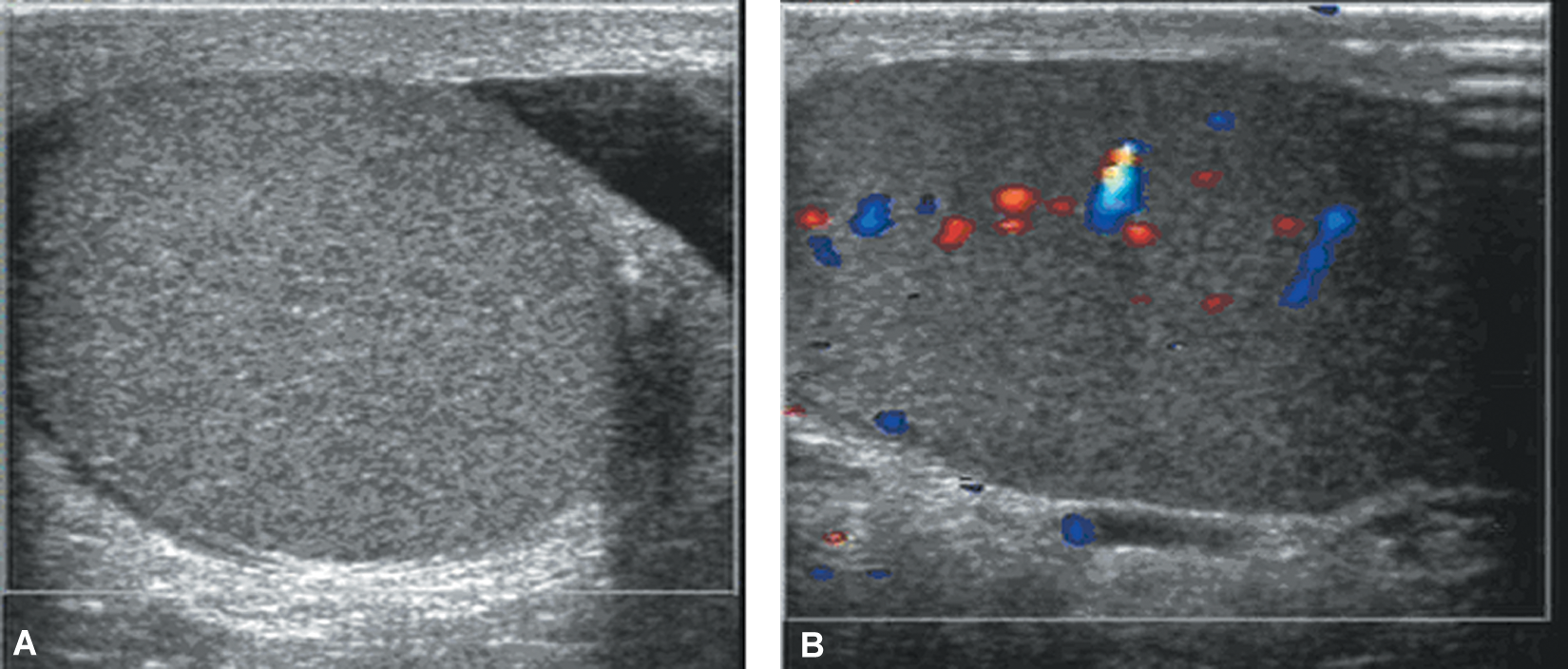
(A) A 17-year-old boy with sudden-onset pain of the left hemiscrotum for two hours. Color Doppler sonography showed the symptomatic testis was homogeneous and isoechoic with absent vascularity. (B) Testicular blood flow resumed immediately after manual detorsion.
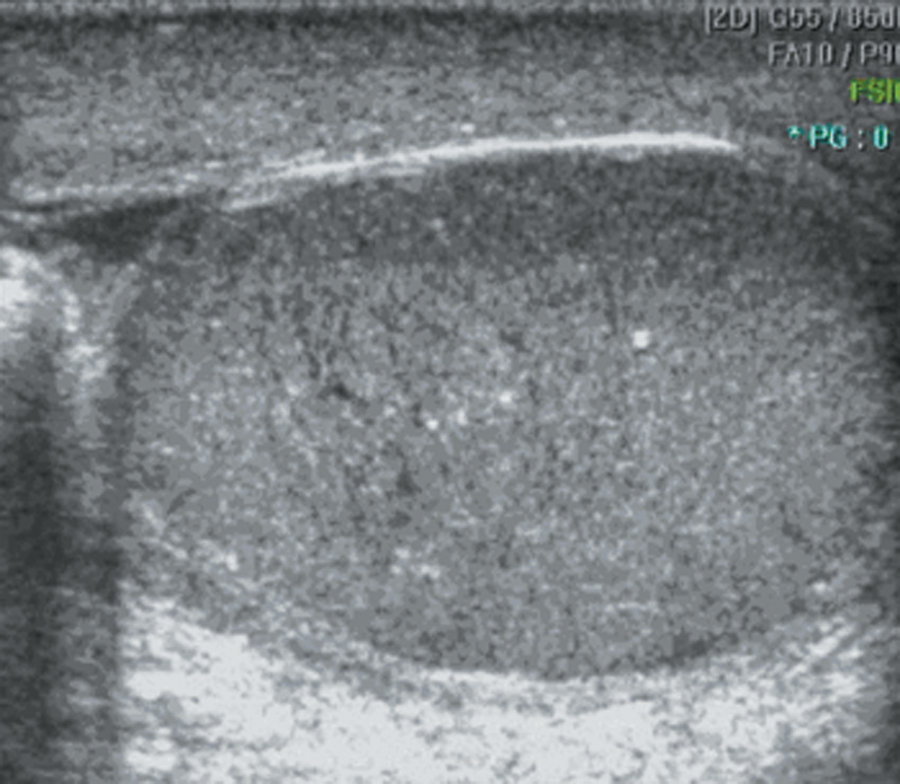
A 19-year-old man with abrupt pain of the left hemiscrotum for six hours. Color Doppler flow imaging detected no blood flow in the symptomatic testis. Sonography showed the testis was heterogeneous and isoechoic with linear hypoechoic striations. Surgical exploration confirmed testicular torsion.
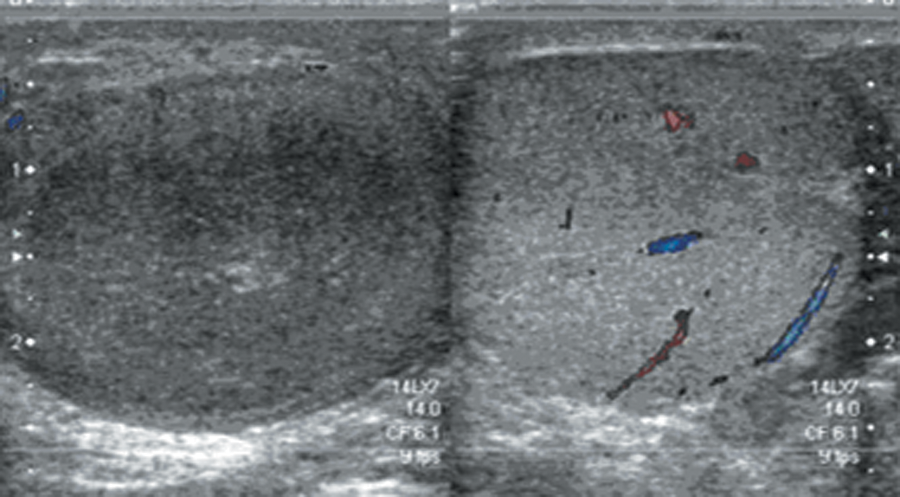
A 14-year-old boy with sudden pain of the right hemiscrotum for nine hours. Color Doppler sonography showed a homogeneous, isoechogenic central portion with heterogeneous hypoechogenecity in the peripheral region and absent vascularity in the symptomatic testis (left plot of the image). The asymptomatic testis (right plot of the image) was homogeneous and isoechoic with normal vascularity. Manual detorsion confirmed testicular torsion.
A 21-year-old man with severe intermittent left hemiscrotal pain for 47 hours. Color Doppler sonography showed that the symptomatic testis was heterogeneous and hypoechoic, with patchy marked hypoechogenicity and absent vascularity. Surgical exploration confirmed testicular torsion and necrosis.
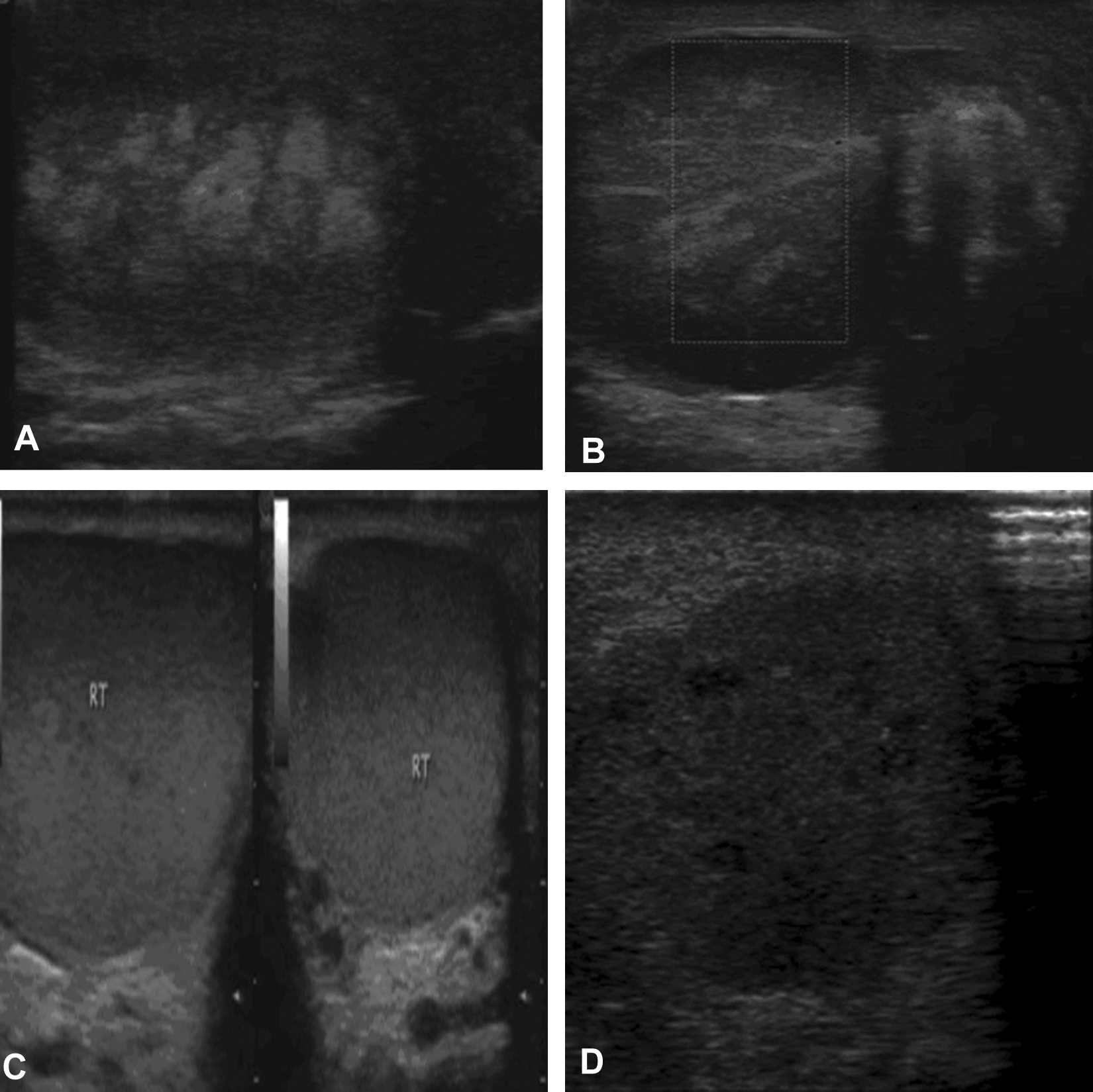
(A) A 24-year-old man with abrupt left hemiscrotal pain for 58 hours. Sonography showed the symptomatic testis was heterogeneous and hypoechoic with altered patchy hyperechoic areas with bulging appearance. (B) Color Doppler flow imaging of the symptomatic testis showed absent vascularity. The parenchyma was heterogeneous and hypoechoic with radially oriented hyperechogenicities and an overbulging appearance, indicating intratesticular hemorrhagic infarction with blood vessels. Surgical exploration confirmed testicular torsion and necrosis. (C) Sonography (left: longitudinal view; right: transverse view) showed that the asymptomatic right testis was homogeneous and isoechoic. (D) Sonography of postoperative detorsion showed the symptomatic testis was heterogeneous and hypoechoic with patchy marked hypoechogenicity, and the previous hyperechoic patchy area disappeared (the symptomatic testis was removed in three days).
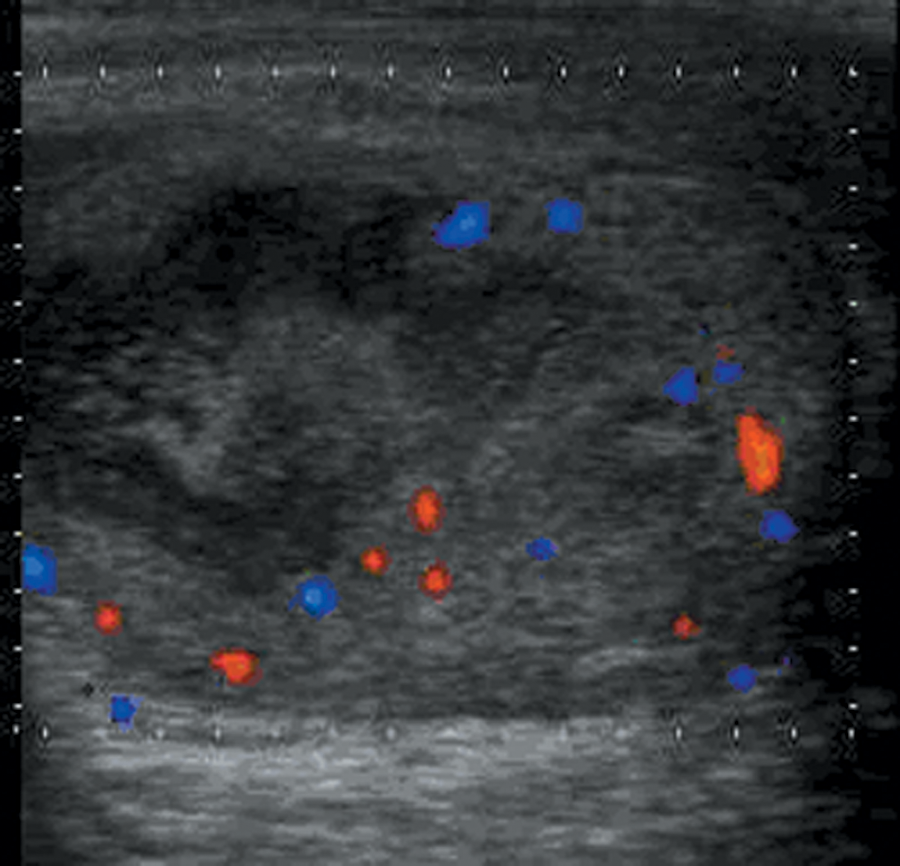
A 13-year-old boy with severe right hemiscrotal pain one hour after blunt scrotal trauma. Color Doppler sonography showed the testis in the right hemiscrotum was heterogeneous and isoechoic with irregular anoechoic areas and poor vascularity. The color Doppler sonographic diagnosis indicated right testicular trauma. Surgical exploration confirmed traumatic testicular contusion and incomplete testicular torsion.
Table 1 shows a summary of the sonographic findings of different patterns of testicular torsion. Table 2 shows the patients’ ages, duration time, management, and outcome. The differences in duration time were not significant between patterns I and II (P < .001) or patterns IV and V (P < .001), but they were significant between patterns I, II, III, IV, and V (all P > .05).
Sonographic Findings of Different Patterns of Testicular Torsion
Number, Age, Duration, Treatment, and Outcome of the Patients With Testicular Torsion
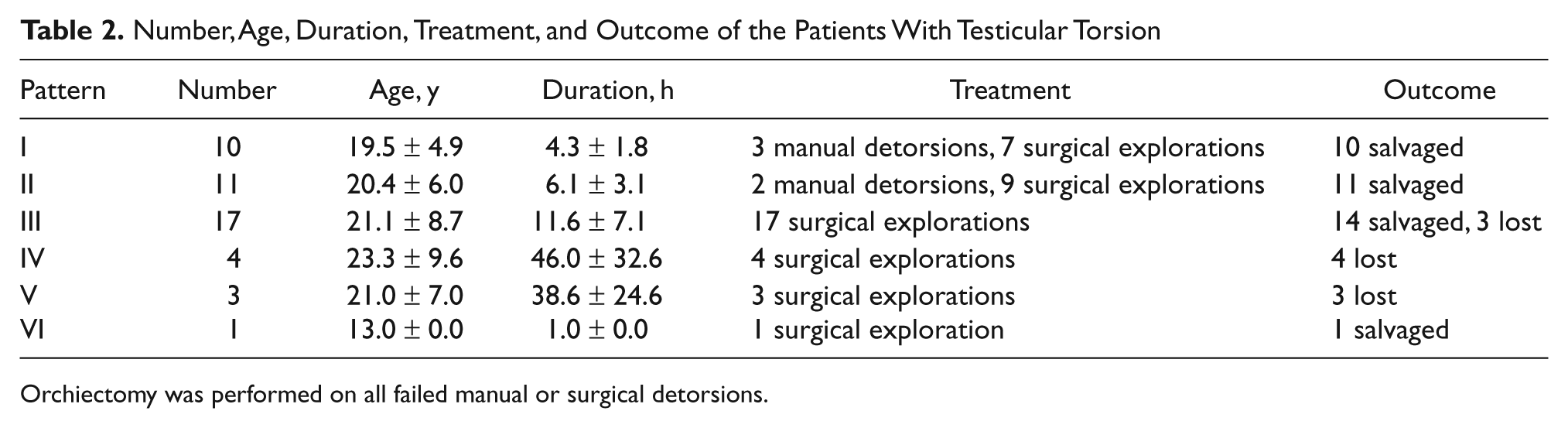
Orchiectomy was performed on all failed manual or surgical detorsions.
Torsed testes of patterns IV and V were found nonviable, and all were lost (4/4, 100%; 3/3, 100%); a small number of torsed testes of pattern III were found nonviable and lost (3/17, 17.6%); torsed testes of patterns I, II, and VI were found viable and saved. Comparing I, II, and VI with IV and V, respectively, the differences between them were all significant (P < .05).
Of the 46 patients, 9 with nonviable testes had orchiectomy, 37 patients had viable testes, 32 had orchidopexy, and 5 waived orchidopexy. All patients who had surgical detorsion had simultaneous contralateral orchidopexy.
Discussion
Scanned by color Doppler sonography, the normal testis is ovoid and has homogeneous isoechogenicity with moderately distributed vascularity, and a testicular torsion presents various echogenicities and absent vascularity. Sonography plays an important role in the diagnosis of testicular torsion, which depends mainly on CDFI or PDI1–5; grayscale sonography can find morphological abnormalities of the torsed testes, which provides a helpful complement to the diagnosis. However, the grayscale patterns are nonspecific, particularly in early stages, when sonography of the testis often appears normal or mildly swollen; as the torsion continues, the changes that cause detectable sonographic abnormalities grow evident, and testicular swelling and areas of patchy hypoechogenicity may be found. 9 These occurred in this study. The sonographic appearance of testicular torsion is associated with testicular viability, which depends on the degree and the duration of torsion. 10 To better recognize these changes, classification of different sonographic patterns is helpful. In incomplete torsion, with testicular hemodynamics compromised, testicular blood supply and drainage do not stop. In the acute phase, the testis is viable and does not display evident change. CDFI and PDI may detect vascularity in some cases and thus lead to a missed diagnosis, as demonstrated in pattern VI. In complete torsion, when the torsion is not managed effectively after an acute episode, ischemia persists, leading to subsequent change in the sonographic pattern, and the cells become nonviable. This evolution was demonstrated in patterns III and IV, as supported by some studies.6,7 As time passed, all torsed testes developed necrosis and atrophy resulting from ischemia and demonstrated a homogeneous or heterogeneous hypoechoic structure, with or without a punctuate hyperechoic element (calcification).
The patterns depend mainly on the degree of blood perfusion and ischemia, rather than the duration of symptoms, because testis perfusion can be maintained for a prolonged period after testicular torsion in some cases,10,11 especially in incomplete torsion and intermittent testicular torsion, thus suggesting that patterns may primarily reflect the degree of damage to the torsed testes and predict viability. In this study, the duration of symptoms between different patterns was various. Between patterns I and II, there was no significant difference, and all the testes were saved; between patterns IV and V, there was no significant difference, and all the testes were lost, which suggests that the patterns were related to the prognosis but did not reflect the duration of symptoms accurately. This study was consistent in general with findings by Nussbaum Blask and Rushton 8 that after 10 hours of symptoms, most testes cannot be salvaged. In this study, the percentage of loss of testicular torsion between different patterns was significantly different, which suggests the patterns are related to the pathologic changes. Testes with pattern I were all salvaged, representing an acute episode or mild degree of late-phase torsion, which is consistent with some studies.6,7 Testes with patterns II and III were mostly salvaged, representing progressive and secondary changes of patterns I and II. Testes with pattern IV were lost, representing progressive and secondary changes of pattern III, indicating diffuse necrosis and nonviability, which is consistent with a previous study. 7 Testes with pattern V were lost, representing early stages of hemorrhagic infarction and necrosis.
In this study, the classification was based on older children and adults, with more cases and sonographic characteristics related to pathologic stage, which is different from Traubici et al., 12 who divided the sonographic appearance of testicular torsion in neonates and infants into three types and proposed the findings represented different stages in the evolution of testicular torsion. However, there were some similarities in the correlation between the sonographic findings and pathologic changes: In their study, type 1 represented sonographic changes correlating with the acute phase of testicular torsion, and hypoechoic radially oriented striations were believed to be related to the thickened interlobular fibrous septa separating the more echogenic necrotic parenchyma seen on pathologic examination that also were present in pattern III in this study. In the study by Traubici et al., 12 type 3 sonographic changes reflected the later phases of progressive atrophy of the parenchyma, which also appeared in this study. In this study, the patients were all older than those in the study by Traubici et al., 12 all patients knew the beginning time of the testicular torsion, and the sonographic appearances were different.
It is necessary to point out that based on grayscale sonography, patterns I and II offer no useful information for the diagnosis of testicular torsion, which is consistent with another report. 13 For patients with scrotal trauma, even though there are no evident abnormal findings with CDFI and PDI, as pattern VI shows, doctors should be alert to avoid missing the diagnosis of testicular torsion in challenging cases.10,11
The potential limitations of the study were that the study was retrospective and case selective with statistical biases because the samples were not large enough, and there were no cases including neonates and infants.
In conclusion, testicular torsion may be classified into six patterns, and the different patterns reflect various histopathologic changes resulting from decreased or ceased blood perfusion. Patterns I and II indicate that the lesion of the testis is mild, and prompt management may enable the testis to be salvaged; pattern III suggests the lesion is somewhat serious, and necrosis may have occurred; patterns IV and V indicate the lesion is serious, and necrosis has occurred; and pattern VI indicates incomplete torsion may have occurred in scrotal trauma. Awareness of the sonographic patterns will improve diagnosis and management and avoid unnecessary orchidectomy.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.