
Abstract
Intratesticular epidermoid cysts are rare, benign, well-defined, and solitary keratinized intratesticular lesions. They usually present as a painless, discrete, and firm swollen area before being diagnosed. Preoperative diagnosis of epidermoid cysts is often difficult. Sonography is a useful imaging modality in the preoperative assessment of testicular lesions. Although it is difficult to distinguish epidermoid cysts from germ cell tumors, certain sonographic characteristics such as the classical “onion-peel” appearance, the negative tumor markers, and the underlying symptoms should raise the suspicion of epidermoid cysts.
Intratesticular epidermoid cysts are uncommon, benign keratin-containing lesions, occurring in any age group from young children to elderly male populations.1,2 They are typically round to oval in shape and 2 to 3 cm in mean size. 3 Most epidermoid cysts present as unilateral, solitary, painless, and palpable masses. 4 Germ cell tumor markers in testicular epidermoid cases are usually negative. 5
Sonographic imaging has long been the modality of choice for evaluating the scrotum and its contents. Because of the continued improvement of sonographic technology and increasing clinical experience, sonographers and sonologists are likely able to diagnose epidermoid cysts with greater certainty. This study presents a case of an epidermoid cyst with a unique “onion-peel” sonographic appearance. This “onion-peel” sonographic appearance is formed by the alternating hypoechoic and hyperechoic concentric rings of keratin deposition. The combination of this sonographic feature and negative tumor markers enabled a proper diagnosis and prevented an unnecessary orchiectomy.
Case Report
A 14-year-old male presented with a painless, palpable solid mass of the left testicle. The patient indicated that he had been aware of the lump for three weeks. The patient’s medical history was unremarkable. The patient denied any pain, fever, weight loss, or night sweats.
Physical examination on admission revealed a palpable, nontender mass of the left testicle without inguinal or cervical lymphadenopathy. The right testicle was unremarkable. Testicular serum tumor markers, including β-human chorionic gonadotropin and α-fetoprotein, were normal. The patient was referred for a sonographic examination to rule out an intratesticular neoplasm or infection.
Sonographic examination of the scrotum using an ML 6- to 15-MHz linear array transducer (GE Logic 9; GE Healthcare, Waukesha, Wisconsin) revealed a 2.9-cm × 2.0-cm × 1.8-cm well-defined, round, solid mass within the left testicle with hypoechoic and hyperechoic concentric rings (an onion-peel sonographic appearance) (Figure 1). The mass contained multiple tiny echogenic foci (calcifications) throughout (Figure 2). The remaining and surrounding left testicular parenchyma, as well as the left epididymis and the right scrotal contents, was considered to be of normal echogenicity. Although the Doppler assessment of the mass showed normal color flow in the parenchyma surrounding the mass, no vascularity was detected within the mass (Figure 3).
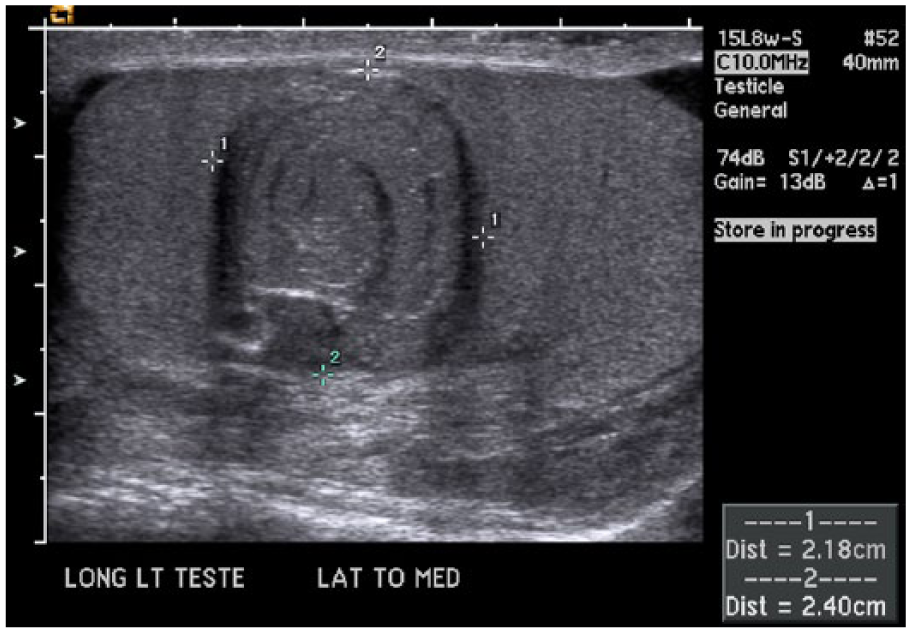
A longitudinal grayscale image of the left testis demonstrating a mass with “onion-peel” appearance (calipers) with normal-appearing surrounding testicular tissue.
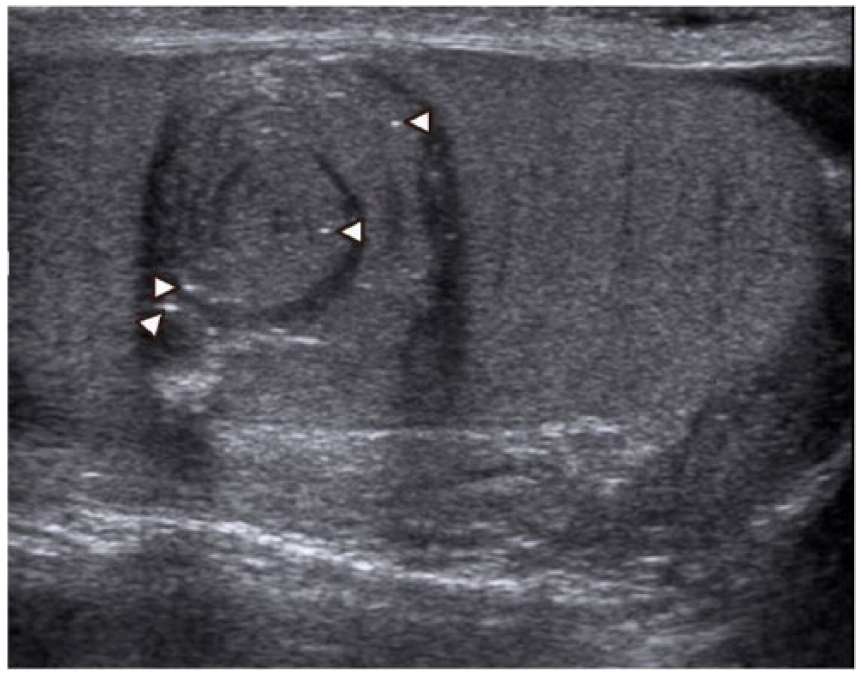
A longitudinal grayscale image of the left testis demonstrating the “onion-peel” appearing mass with tiny echogenic foci or calcifications (arrowheads).
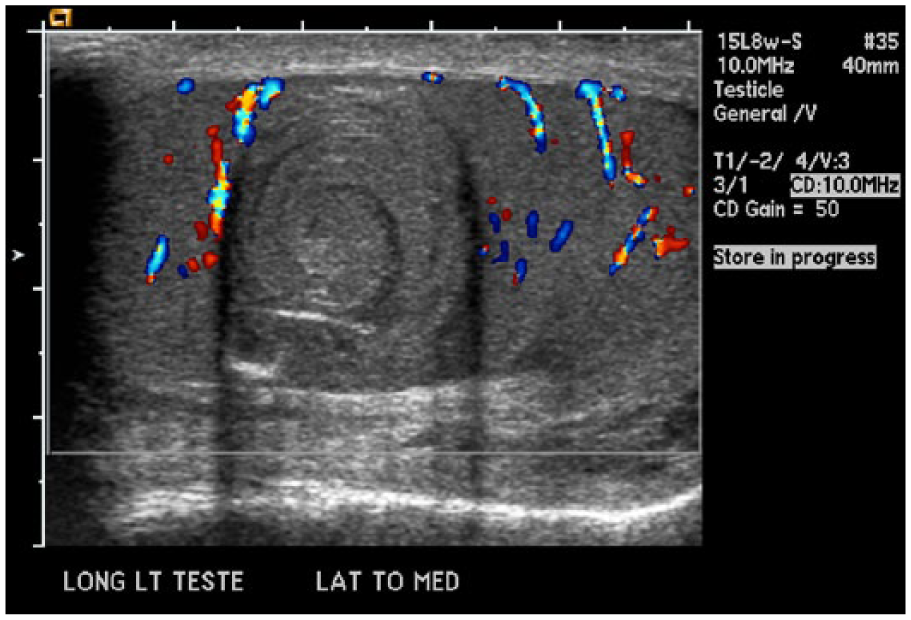
A longitudinal color Doppler image of the left testis demonstrating the absence of internal vascularity within the mass and normal blood flow in the surrounding testicular parenchyma.
The differential diagnosis for this testicular lesion included epidermoid cyst and germ cell tumors. Management options, including surgical intervention, were discussed with the patient’s family. The patient’s family elected to have surgical intervention, and a radical left orchiectomy was performed. The patient’s recovery was uneventful.
Histopathologic examination of the specimen showed a keratin-filled cyst surrounded by squamous epithelium, normal tubules in the surrounding testicular parenchyma, focal calcifications, and no teratomatous elements.
Discussion
Testicular epidermoid cysts, also known as keratocysts, were first reported in 1942 by Dockerty and Priestley. 6 Epidermoid cysts, lined by squamous epithelium, are rare, benign keratin-containing lesions that account for 1% to 2% of all testicular tumors in adults 7 and 3% of testicular tumors in children.1,8–12 Although epidermoid cysts can occur in any age group, they are most commonly seen in males between 20 and 40 years of age,8,9,11 with a higher propensity among Caucasians and Asians.7,10 It has also been reported that there is a higher prevalence of epidermoid cysts developing in the right testicle. 13
Most lesions are unilateral, solitary masses, unless they are associated with Gardner syndrome, Klinefelter syndrome, or cryptorchidism, which can be multiple, bilateral, or both.4,5,14–17 Epidermoid cysts present in varying sizes, ranging from 0.5 to 10.5 cm, with a mean size of 2 to 3 cm in diameter.4–6,18–21 Most patients with epidermoid cysts are asymptomatic and may present with a smooth, firm, well-circumscribed, palpable, and painless intratesticular mass.4,18,19,22 Other symptoms such as scrotal tenderness, pain, and enlargement have also been reported.4,10
Unlike the majority of malignant germ cell tumors, tumor markers for epidermoid cysts, including β-human chorionic gonadotropin and α-fetoprotein, and genetic markers such as 12p chromosome are usually negative.5,10,11,16,23–25
The exact nature or embryogenesis of this pathology is controversial. 26 Some researchers consider epidermoid cysts to represent an end result of a monolayer teratoma from germ cells.4,8,27,28 Others suggest that epidermoid cysts represent a squamous metaplasia of seminiferous epithelium, metaplasia of the rete testis, or inclusion of epidermal cysts.5,19,20,29
The distinction between epidermoid cysts and teratomas is often difficult. 30 Despite the difficulty of distinguishing between epidermoid cysts and teratomas, Price 20 reported that clinical and pathological criteria can be integral in making the diagnosis. He stated that epidermoid cysts (1) must be intratesticular, (2) contain keratinized debris, (3) are composed of complete or incomplete fibrous squamous epithelia in their walls, (4) lack any teratomatous components or dermal adnexal structures (e.g., hair follicles or sebaceous glands) within their walls or testicular parenchyma, and (5) do not have any scars within the remaining testicular parenchyma, which might represent an inactive malignant germ cell tumor. Others have reported that if testicular intraepithelial neoplasia is present in the adjacent tissue, the tumor should be considered a teratoma and not an epidermoid cyst. 10
In addition to the clinical and pathological criteria, the hematological, serological, and biochemical parameters may be useful in the diagnosis and differentiation of epidermoid cysts and teratomas. According to Cheng et al., 25 epidermoid cysts have negative β-human chorionic gonadotropin and α-fetoprotein and lack abnormalities in chromosome 12p and thus can be useful diagnostic tools for distinguishing testicular epidermoid cysts from teratomas. The findings in this case were consistent with the abovementioned criteria.
Sonography has enhanced the diagnosis of testicular epidermoid cysts by documenting many of the physical characteristics associated with this abnormality.19,26,31–33 The sonographic features that have been described and reported are a well-defined, well-circumscribed, intratesticular mass with normal surrounding testicular parenchyma18,21,33; a lesion with an echogenic center surrounded by a hypoechoic concentric rim, with or without a hyperechoic rim, referred to as the bull’s-eye or target appearance13,21,22; a densely calcified echogenic lesion with acoustic shadowing 34 ; and, as in this case, a lesion with alternating hypoechoic and hyperechoic concentric rings giving rise to the classical sonographic “onion-peel” appearance, representing the alternating patterns of keratin deposition.18,19,31,32 Arellano et al. 12 found 7 of 11 patients had an “onion-peel” appearance of the epidermoid cyst. They found mature lesions that appeared more cystic sonographically. 12
Other sonographic appearances have been reported such as focal or circumferential calcifications 21 ; minimal acoustic enhancement, due to the high acoustic impedance of the internal contents 31 ; cystic appearance, especially for newer lesions 10 ; lack of internal vascularity within the lesion, detected with Doppler7,18,22; and lack of hyperenhancement on contrast-enhanced sonography. 35
The treatment and management of testicular epidermoid cysts have been controversial. Many researchers have emphasized the need for orchiectomy to reach a histologic diagnosis of the lesion.10,16 Recently, additional investigation has advocated organ-preserving local excision, wedge resection, or enucleation of the lesion if negative tumor markers, 12p chromosomal analysis, and radiologic findings are specific for epidermoid cysts.8,12,25,36–38 In a literature review study of 300 cases treated with enucleation or wedge resection, Heidenreich et al. 16 found no incidence of local subsequent recurrence or peripheral metastasis. Moreover, Malek et al. 5 reported no subsequent recurrence of epidermoid cysts in 160 patients, including 28 patients who had undergone enucleation, with the longest follow-up of 23 years. In enucleation cases, open biopsy for frozen-section analysis of the lesion and adjacent parenchyma has been recommended to rule out germ cell tumor, scar, or carcinoma in situ.8,39
When the preoperative findings suggest an epidermoid cyst, some believe that testis-sparing surgery should be the treatment of choice as it improves psychologic and cosmetic results, as well as preservation of fertility.16,40–42 Overall, the treatment and management of testicular epidermoid cysts must be tailored to each patient, depending on the preoperative tumor markers and the sonographic findings and diagnosis.
Conclusion
Sonography has enabled direct visualization and identification of various scrotal abnormalities. Epidermoid cysts should be suspected when a lesion with alternating hypoechoic and hyperechoic concentric rings gives rise to the classical sonographic “onion-peel” appearance. The sonographic features, along with negative tumor markers (α-fetoprotein and β-human chorionic gonadotropin) and absence of chromosome 12p, may support the diagnosis of an epidermoid cyst. The preoperative diagnosis of epidermoid cyst may provide a critical data point regarding the treatment, management, and adequate counseling and guidance for this pathology.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.