
Abstract
Objective:
The aim of this study was to assess the sonographic changes within the testis, epididymis, and the corresponding appendages, in contributing to the pediatric differential diagnosis, of an acute scrotum.
Materials and Methods:
A retrospective extraction of pediatric patients’ (age <13 years) data was completed for those initially seen with an acute scrotum. The data procured from the medical records included demographic characteristics, clinical and sonographic findings, and the final diagnosis.
Results:
The final diagnoses among a cohort of 86 pediatric males (average age 6 ± 3.9 years) with acute scrotum were as follows: epididymal and testicular appendix torsion (44.7% and 17.6%, respectively), testicular torsion (15.3%), trauma and hematoma (5.9%), incarcerated hernia (4.7%), idiopathic scrotal edema (4.7%), epididymitis (4.7%), and Henoch-Schonlein purpura (3.5%). The heterogeneous testicular appearance in patients with testicular torsion was significantly compared with the appendix torsion. The increased testicle size noted on the sonogram favored the diagnosis of testicular torsion. In cases of testicular torsion, the vascular flow was reduced or absent, although it was normal or increased in appendix torsion. Increased epididymal vascular flow was more common in cases of appendix torsion.
Conclusion:
Based on the diagnostic findings in this cohort, the following were the most common and accurate sonographic findings in distinguishing the causes of a pediatric acute scrotum: an epididymis enlargement coexisting with a small adjacent avascular mass, due to the torsion of intra-scrotal appendages and a mass shape of the epididymis.
Keywords
An acute scrotum is an emergency condition, in children and adolescents, that occurs suddenly and is accompanied by pain, swelling, and redness of the scrotum. The worldwide prevalence of an acute scrotum is not well established due to the varying definitions and diagnostic criteria used in different studies. However, the annual incidence has been reported at almost 3.5 per 100 000 young males. An acute scrotum is considered as a limb-threatening or life-threatening condition that requires urgent treatment. Testicular torsion is one of the most serious causes affecting the scrotum components and can lead to the loss of a testicle. 1 The testicle may be twisted around the axis of the spermatic cord, causing swelling and occluding the venous and arterial pathways, which leads to ischemia. 2 When considering testicular torsion, the testicular parenchyma can only tolerate ischemia for a short time. The torsion should be diagnosed as soon as possible, detorted, and repaired through surgical intervention.
Other causes of acute scrotum are the intra-scrotal appendicular torsion (the twisting of the appendages inside the scrotum), trauma, hernia, Henoch-Schonlein purpura, epididymitis, and acute scrotal edema.3 –5 The most common cause of acute testicular pain, in pediatrics, is torsion of the intra-scrotal appendages. However, the differential diagnosis between testicular torsion and torsion of the intra-scrotal appendix is usually challenging, due to the overlap of symptoms and signs. 6
Considering the wide range of causes of acute scrotum and their potentially irreversible complications (such as testicular torsion), identifying the cause of the acute scrotum is of considerable importance. It is vital to achieve a timely diagnosis and management of these emergency cases. It is imperative that the diagnostic tools for discerning the etiology of scrotal pain and swelling demonstrate a high degree of accuracy. This ensures that a team of health care professionals can arrive at a precise diagnosis, within a shortened timeframe.
Sonography is the primary diagnostic choice for the examination of patients with an acute scrotum, although sonographic findings of the causes of acute scrotum are not pathognomonic. Therefore, a radionuclide imaging study or surgery may be needed for pathologic differentiation. The aim of this study was to assess the sonographic changes within the testis, epididymis, and the corresponding appendages, in contributing to the pediatric differential diagnosis of an acute scrotum.
Materials and Methods
A total of 86 patients, under 14 years of age, with acute scrotum were referred to the radiology department at the local children’s hospitals between 2017 and 2022. The patients were included in this cross-sectional study through enumeration sampling. The inclusion criteria were acute scrotal evidence, such as pain, swelling, or redness, in the scrotum. Patients older than 13 years, a lack of acute scrotal evidence, or those unwilling to participate were excluded from the study. The medical ethics committee of Mashhad University of Medical Sciences approved this study (approval number IR.MUMS.MEDICAL.REC.1398.825). The parents or guardians of all the patients signed an informed consent.
Sonographic findings of 86 patients with acute scrotum included the size, axis, shape, echo pattern, and vascularity of the affected testis and epididymis and were evaluated with the following ultrasound equipment systems: Esoate (Genova, Italy), WS80 (Samsung, Seoul, South Korea), and E6 (GE, Waukesha, Wisconsin). The ultrasound systems used multi-frequency surface transducers that had a frequency of 10 to 12 MHz. Patients’ information including demographic characteristics, clinical findings at the time of referral, and final diagnosis was all extracted from their medical records for analysis. The final diagnosis was based on the clinical, para-clinical tests (mainly the sonogram), and the surgical findings (if surgery was performed).
The normal epididymis was observed as comma-shaped with the elongated structure located on the posterior/posterolateral border of the testis; the epididymal head and tail were found at the superior and inferior poles, respectively, attached to the testis through the mediastinum. In patients with testicular torsion, the epididymal head and tail were not seen in the upper and lower poles of the testis, whereas they were aggregated on the mediastinum, forming a mass-like configuration. The twisting of the appendages inside the scrotum or torsion of intra-scrotal appendages (testicle or epididymis) was seen as small oval or round mass. Patients were assigned into two groups of testicular torsion and appendage torsion (i.e., a testicular group or epididymal group) according to their final diagnoses. The distribution of testicular and epididymal sonographic findings was compared between the two groups.
Data Analysis
The planned data analytics were performed using SPSS version 25 (IBM, Chicago, Illinois). An alpha level of p < .05 was considered as statistically significant. Patients’ demographic data and general characteristics were provided using descriptive statistics. The relationship between the qualitative data was also determined using the chi-square and Fisher’s exact tests. The strength of association between variables was also determined by a Pearson’s test for normally distributed data and the Spearman’s test for non-normally distributed data.
Results
This study included data from a total of 86 males with an acute scrotum. The average age of the patients was 6.03 ± 3.93 years (range = 2 days to 13 years). Pain was present in all patients, and the most common clinical finding was swelling (41.2%). The symptoms were on the left side in 45 patients (52.9%), on the right side in 35 patients (41.2%), and bilaterally in 5 patients (5.9%). The most common locations of pathology were the epididymis and the testis (58.8% and 28.2%, respectively). Other anatomical sites were the scrotal wall, cord, and process vaginalis. The differential diagnoses of children with acute scrotum in our study are shown in Figure 1.
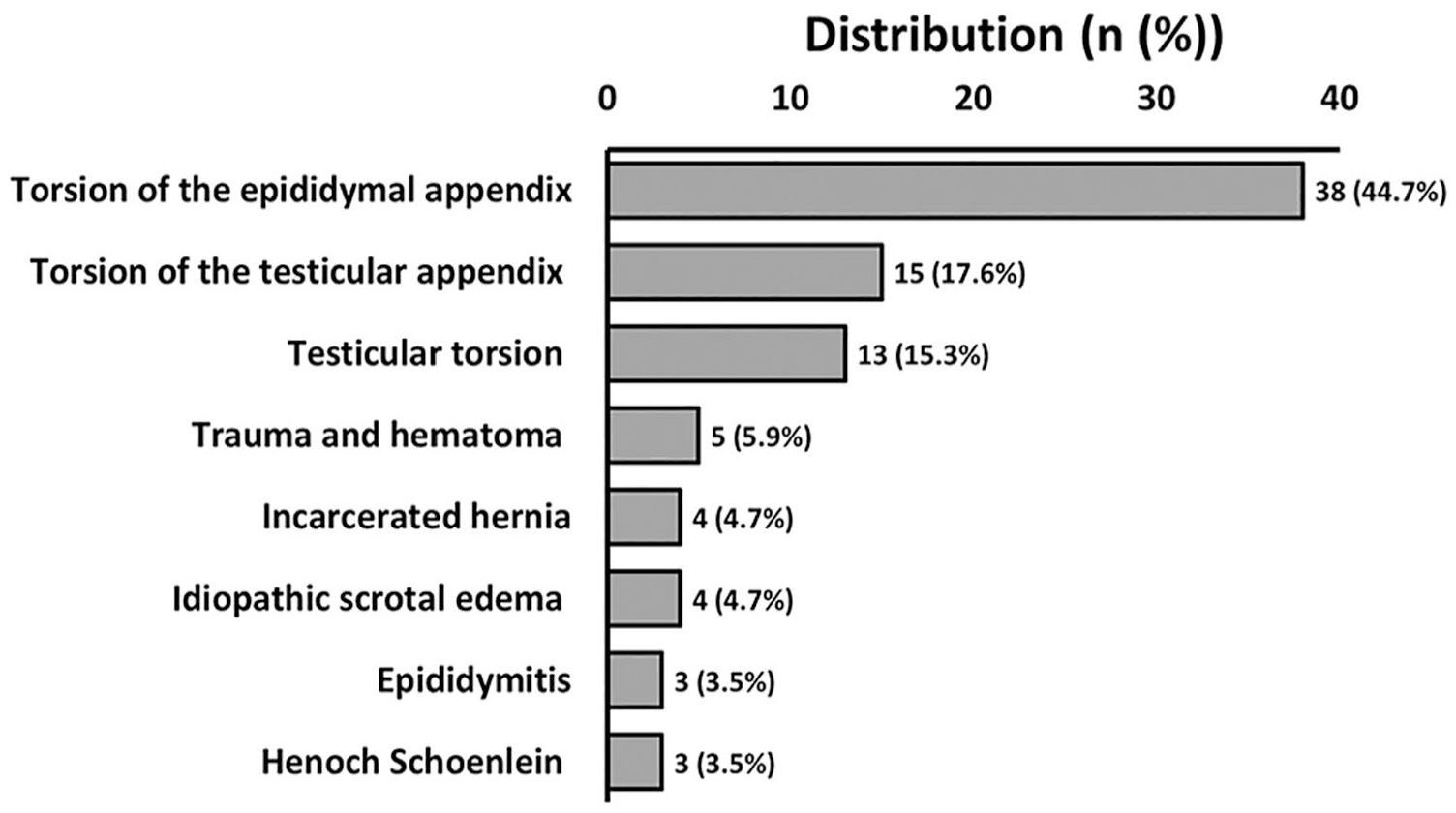
A bar graph that provides the varied differential diagnoses of pediatric patients with an acute scrotum.
Other uncommon causes of acute scrotum including epididymitis, hematoma, and acute scrotal edema are shown in Figure 2.
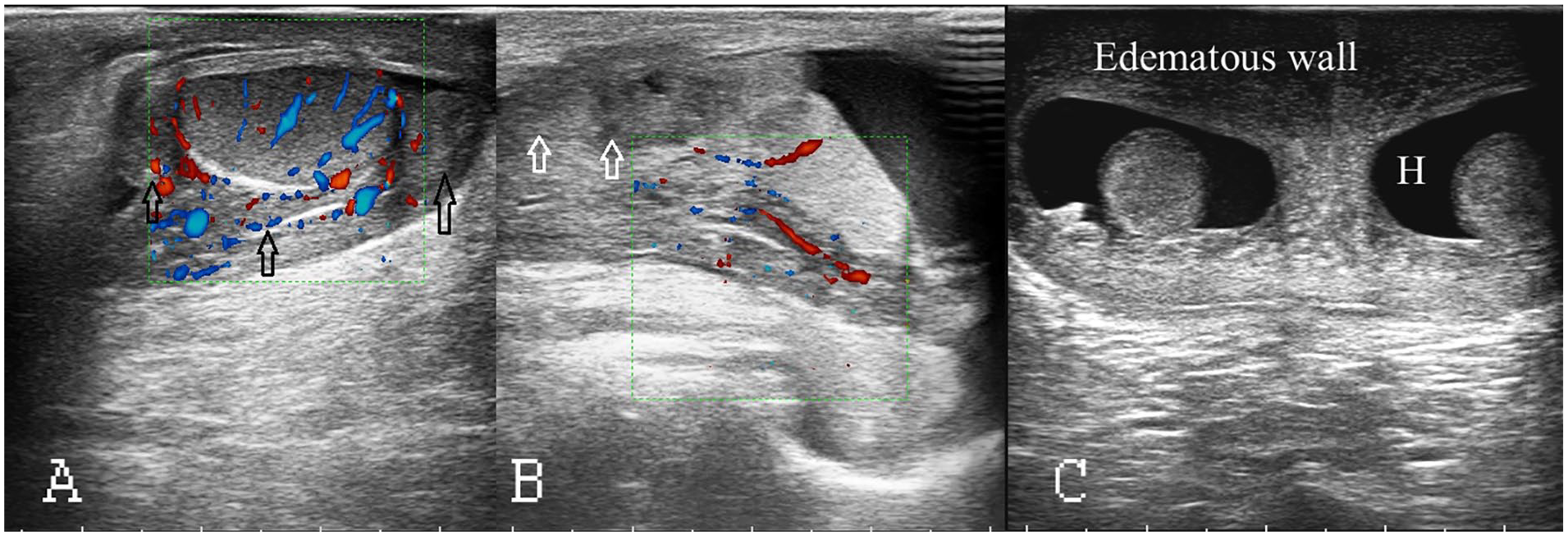
In this study, there were documented other uncommon causes of an acute scrotum. (A) Epididymitis: a sonographic image is provided of an enlarged epididymis that was observed as comma-shaped with the elongated structure located on the posterior border of the testis. The epididymal head and tail were found at the superior and inferior poles and are demarcated by black arrows. (B) Hematoma: a sonographic image is provided of a spermatic cord hematoma, which is indicated by white arrows. (C) This sonographic image demonstrates a thickened edematous scrotal wall with hydrocele and that is the hallmark for acute scrotal edema.
The most frequent sonographic finding (72%) was an appendage mass. A torsion of the intra-scrotal appendages (testicle or epididymis) was seen as oval or round mass, that was hyperechoic in 28 (53%), spongy in 13 (24.5%), and hypoechoic in 12 (22.6%) patients. The testis and epididymis enlargement were seen in 15 (17.6%) and 52 (61.9%) patients, respectively. Heterogeneity was seen in 11 (12.9%) testes and 34 (45.2%) epididymides. Vascular flow assessment using color Doppler showed reduced or absent testicular vascular flow in 14 (18%) patients. An absence of blood flow was detected with Doppler in the epididymis in four (5.1%) patients. Increased vascular flow was seen in eight (10.3%) testes and 38 (48.7%) epididymides. A hydrocele was the most common associated finding in 38 (44.7%) patients. The documentation of cryptorchidism and a cord cyst were other uncommonly associated diagnostic findings.
Figure 3 illustrates the testicular and epididymal sonographic findings in patients with testicular torsion and intra-scrotal appendicular torsion. As testicular torsion and intra-scrotal appendicular torsion are two common causes of acute scrotum in pediatric age, they were compared in two groups. Abnormal testicular axis was seen in both groups (nine out of 13 testicular torsions, and 18 out of 53 appendages torsions), with a statistical significance of p = .042. The epididymis enlargement was seen in 33 (62.3%) patient cases with appendicular torsion and nine (75%) patient cases with testicular torsion, with a statistical significance of p = .515. The heterogeneity of epididymis was seen in seven (53.8%) of the testicular torsion patients and in 22 (41.5%) of the appendage torsion patients, with significant difference of p < .001.
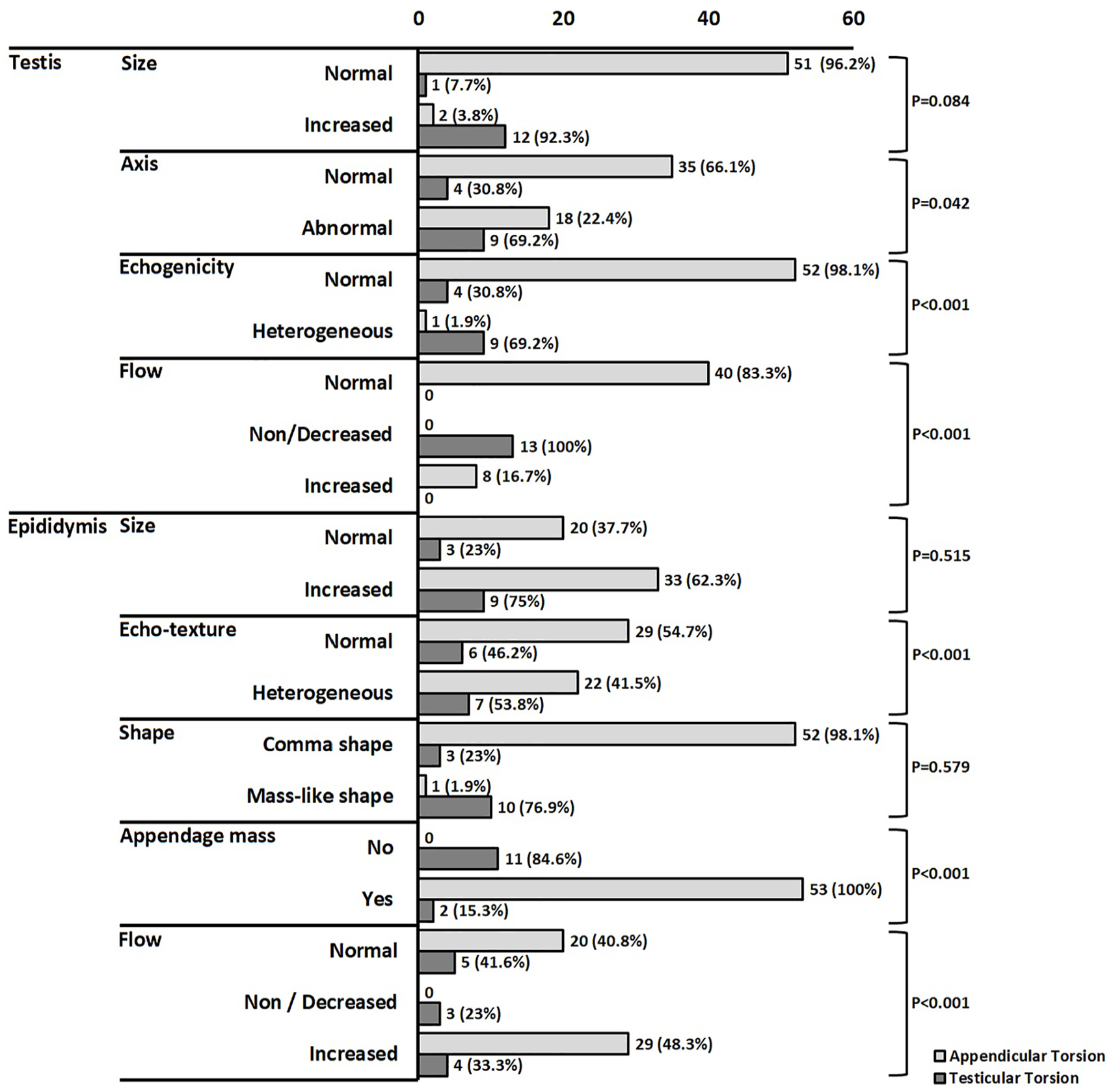
A bar chart is provided for the testicular and epididymal sonographic findings in this cohort of pediatric patients with testicular torsion and intra-scrotal appendicular torsion.
Testis enlargement was seen in two (3.8%) patient cases with appendage torsion and 12 (92.3%) patient cases with testicular torsion, with a statistical significance of p = .084. Testis heterogeneity was seen in nine children with testicular torsion and one with appendage torsion, with a statistical significance of p < .001. Decreased testis flow was seen in all patient cases with testicular torsion and none of appendage torsion. Decreased epididymis flow was seen in three (25%) of the patients with testicular torsion and none with appendage torsion.
The appendage mass was seen in 53 (100%) patient cases with appendicular torsion and two (15.3%) patient cases with testicular torsion, with a statistical significance of p = .001. Mass-like epididymis shape was seen in one (1.9%) case with appendicular torsion. There were 10 (76.9%) patient cases with testicular torsion and with a statistical significance of p < .579.
There were no missed patient cases of testicular torsion, recorded as part of this study. Two patients diagnosed with Henoch-Schonlein purpura, underwent unnecessary surgeries.
Discussion
An acute scrotum is presented with sudden testicular pain and swelling. This can have many underlying causes, some of which are potentially dangerous and require immediate treatment because untreated or untimely patient cases can lead to the loss of the testicle. Etiologically, twisting of a vestigial appendage (located along the testis) is referred to as torsion of the appendix testis, whereas the torsion of the appendix epididymis (the tube-like small appendage on the top of epididymis) is its crumpling.
As testicular torsion and intra-scrotal appendage torsion are two common causes of acute scrotum in pediatric age, the differential diagnosis between the testicular torsion and the appendicular torsion is usually challenging due to the overlap of the symptoms and signs. 7 This study was designed to assess the sonographic changes in the testis, epididymis, and the corresponding appendages as a means of creating a pediatric differential diagnosis of acute scrotum.
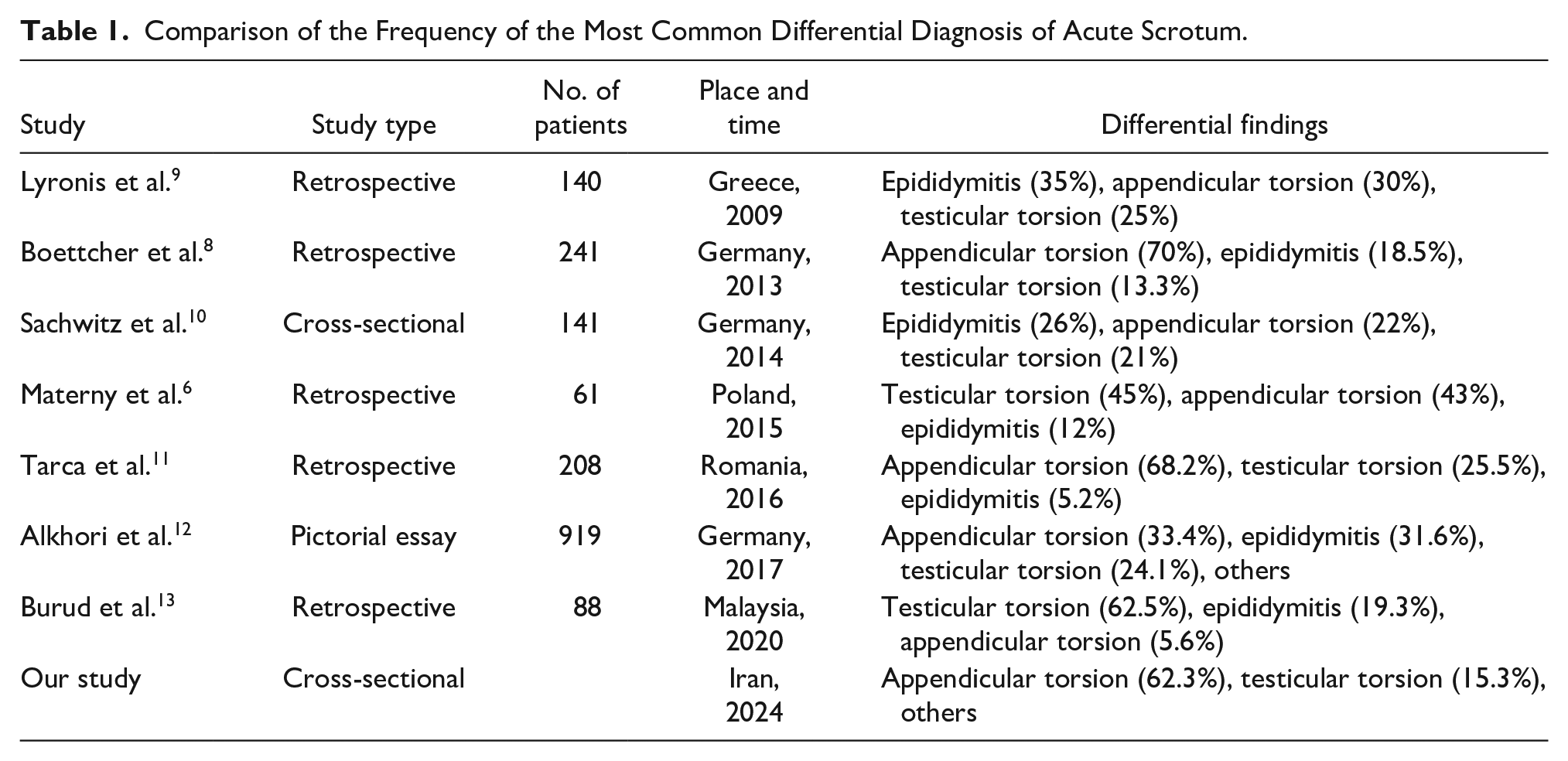
Boettcher et al. reported on the sonographic study of 241 young males with acute scrotum. These patients showed testicular appendicular torsion in 70%, epididymitis in 18.5%, testicular torsion in 13.3%, and idiopathic scrotal edema in 1.3% of patients. 8 Torsion of the testicular appendix was more common in the colder season of the year. The authors stressed that a history of dysuria and the tenderness of epididymis are the best factors in favor of epididymitis. 8 In addition, they stated that the presence of the “blue-dot” sign was the most important factor in favor of the torsion of the appendix, as these signs can be clinically used to differentiate the two mentioned conditions. 8 Table 1 compares the frequency of the most common differential diagnoses of acute scrotum among different studies. It is noted that in more recent studies, the shift from epididymitis to appendicular torsion, as the cause of acute scrotum, has increased. This is probably due to the increase in image quality and resolution, due to more recent ultrasound equipment systems that better detect small masses, caused by torsion of the appendix. Owing to the small size of appendicular torsion, the condition was probably considered as epididymitis. In this study, the common causes of acute scrotum were torsion of the appendix of the epididymis (44.7%), torsion of the appendix of the testis (17.6%), and torsion of the testis (15.3%), respectively. Epididymitis was the seventh most common cause of acute scrotum (3.5%).
Comparison of the Frequency of the Most Common Differential Diagnosis of Acute Scrotum.
The normal epididymis was observed as comma-shaped with the elongated structure located on the posterior border of the testis; the head and tail were found at the superior and inferior poles, respectively, attached to the testis through mediastinum. Torsion of intra-scrotal appendages (testicle or epididymis) was seen as small oval or round mass. Although clinical “blue-dot” sign is seen in a small percentage of patients with appendicular torsion, but a small avascular mass adjacent to epididymis or testis is a common ultrasound finding. It has hyperechoic, spongy, and or hypoechoic echotexture (See Figure 4).
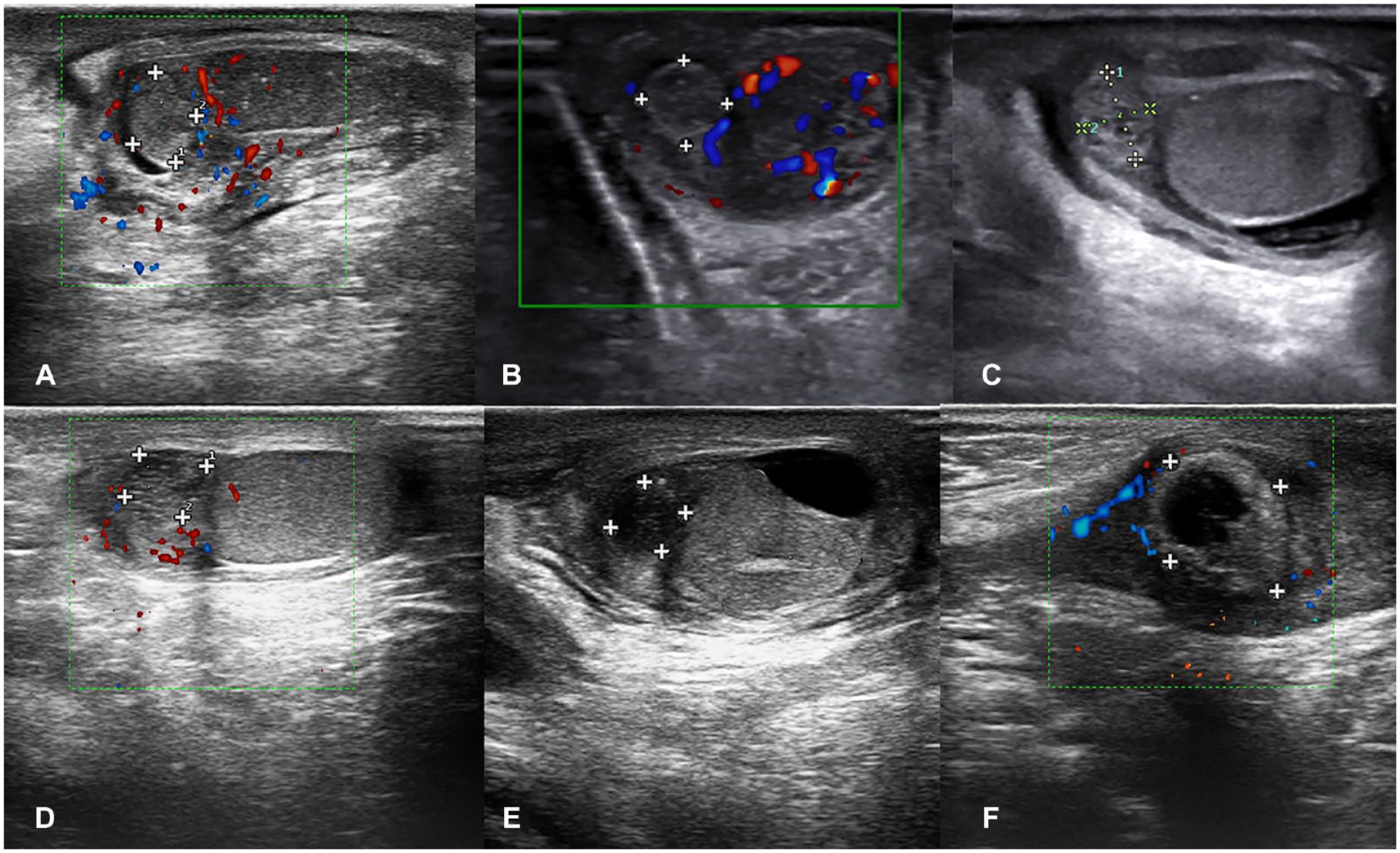
A series of sonographic images that demonstrate torsion of the intra-scrotal appendage: torsion of the intra-scrotal appendage was seen as an oval or round mass (labeled with +), which at first becomes hyperechoic (images A and B), gradually becomes spongy (images C and D), and finally hypoechoic or cystic (images E and F).
Conversely, attention should be paid to a small mass adjacent to the epididymis or testis during sonography. This will allow for differentiating between the torsion of the epididymal/testicular appendix and other pathologies. Acute ischemic appendicular torsion is usually associated with enlargement of normal shape (comma shape) epididymis.
The mass-like shape of enlarged epididymis was seen in 1 (17.6%) patient case with an appendicular torsion and in 10 (61.9%) patient cases with testicular torsion, with a statistically significant difference of p < .001. In patients with testicular torsion, the epididymis aggregated on the mediastinum, forming a mass-like configuration, and head and tail of epididymis were not seen in the upper and lower poles of the testis. The sonographic changes of the epididymis (enlargement associated with mass-like shape or adjacent small mass) are the most common diagnostic findings in pediatric patients with acute scrotum. In addition, these clinical findings helped to create a differential diagnosis for these patients (See Figure 5).
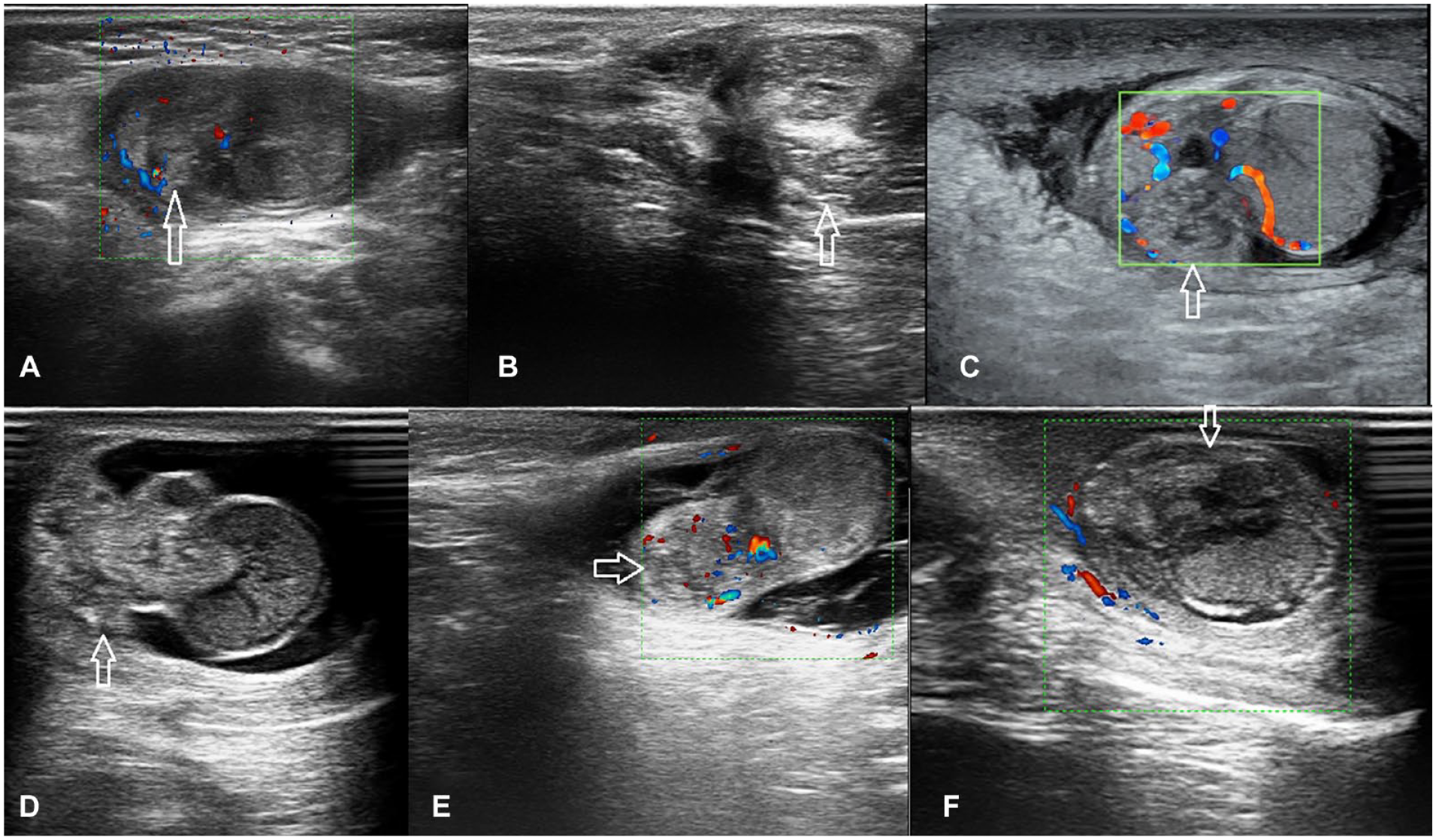
This set of sonograms demonstrates testicular torsion. The epididymis (marked by white arrows) is not seen in the upper and lower poles of the testis and aggregates in the mediastinum of the testis, with a mass-like configuration.
Materny et al. compared the preoperative color Doppler results with the final postoperative diagnosis in 61 pediatric patients with acute scrotum. The specificity of color Doppler for the diagnoses was 46%, 20%, and 57%, respectively. 6 They concluded that color Doppler possesses a low specificity for diagnosing the cause of acute scrotum and surgical intervention is recommended, even if the sonogram is normal. 6
Among the eight mentioned studies performed on diverse geographical populations, only the data of the retrospective study by Boettcher et al. were collected with sonography. This is compatible with this study, which may be the first prospective report dedicated to sonographic findings in pediatric patients with acute scrotum. This cohort’s results may suggest that sonographic findings are helpful in differentiating testicular torsion from appendage torsion (See Table 1).
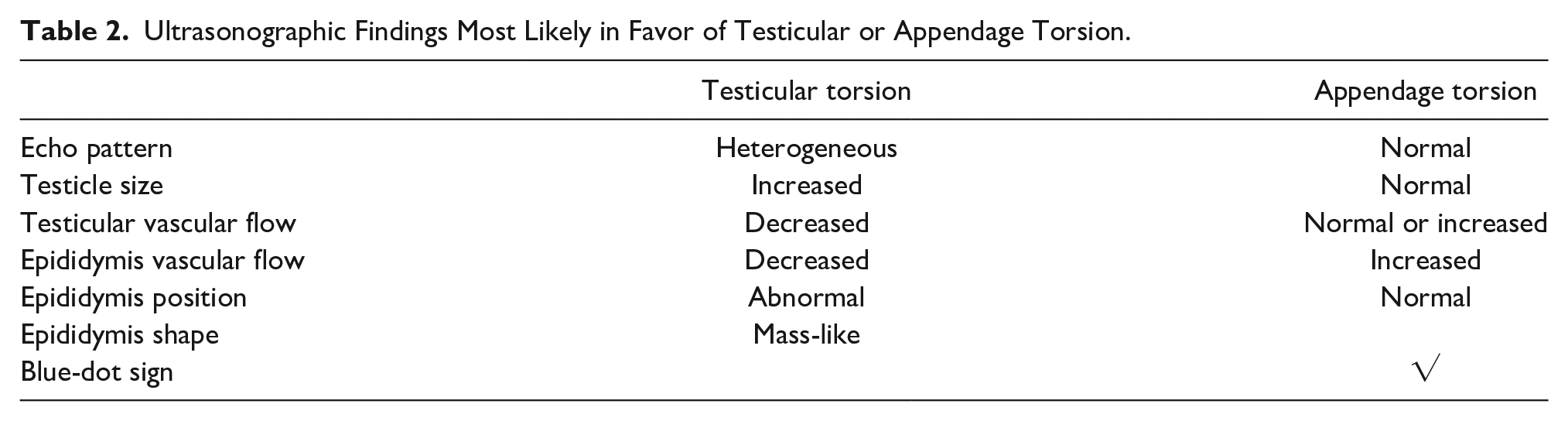
This study’s sonographic findings showed that the heterogeneity of the testicular echo pattern, the increased size of the testicle, the decrease in the vascular flow of the testicle, and the decrease in the vascular flow of the epididymis are in indicative of testicular torsion. Conversely, the normality of the testicular echo pattern, normal size, normal or increased vascular flow, within the testis, and increased vascularity within the epididymis may be indicative of torsion of the appendices (testis or epididymis). The testicular parenchymal heterogeneity, reduced testis, or epididymis flow, and abnormal epididymis position have been mentioned as the most specific findings of testicular torsion. It was also mentioned that testicular enlargement does not help in differentiating the epididymitis and testicular torsion. 14 However, in this study, testicular enlargement may be indicative of testicular torsion compared with epididymal torsion or testicular appendix torsion. Table 2 provides the most likely ultrasonographic findings in favor of testicular or appendage torsion.
Ultrasonographic Findings Most Likely in Favor of Testicular or Appendage Torsion.
Limitations
The major limitation of this study is the research design and the patient sample by convenience. These factors result in threats to internal and external validity; therefore, this work cannot be generalized beyond this cohort. The relatively low sample of patients was also a limiting factor for this study. Hence, further multi-centric studies with a larger sample size are advocated, to investigate this pathologic condition more precisely. A comparative study of epididymal changes in acute scrotum in adolescents would also be valuable.
Conclusion
This study compared the sonographic findings of pediatric patients with testicular torsion and those with appendage torsion. The results of this cohort showed that a mass-like epididymis with decreased vascular blood flow and heterogeneous testis echo pattern may be indicative of testicular torsion. In addition, it is worthwhile to consider normal testicular size, a normal epididymis position, normal testicular echo pattern, normal or increased vascular blood flow, and a “blue-dot” sign, as indicators of a possible appendage torsion.
Footnotes
Acknowledgements
The authors appreciate the pediatric surgeons and pathologists at Akbar Children’s Hospital and the Clinical Research Development Unit, Ghaem Hospital, Mashhad University of Medical Sciences for their advocate help and support. The authors also appreciate the help and support by the Clinical Research Development Unit, Ghaem Hospital, Mashhad University of Medical Sciences.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of the article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research project was financially supported by Mashhad University of Medical Sciences, Mashhad, Iran (#981070). The authors declare no conflict of interest regarding this manuscript.
Ethics Approval
Ethical approval for this study was obtained from The Medical Ethics Committee of Mashhad University of Medical Sciences (approval number IR.MUMS.MEDICAL.REC.1398.825).
Informed Consent
Written informed consent was obtained from legally authorized representatives before the study.
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because no animals were used during the study.
Trial Registration
Not applicable.