
Abstract
Sonography is an essential imaging modality, known for its real-time capabilities, relative low cost, and multiple diagnostic applications. Although there are protocols which are well-established for specific examinations, there are not clear guidelines for sonographic examinations of soft tissues. Many sonographers have to establish their own imaging protocols when completing a soft tissue examination. This case series details five soft tissue examinations that represent just a few of the clinical requests generated in an Urgent Care (UC) facility. Since UC usage has increased over the past several years, it appears likely that any sonographer working in such outpatient settings will benefit from as much exposure to soft tissue examinations as possible.
Sonography is an essential imaging modality, known for its real-time capabilities, relative low cost, and utility in multiple modalities to examine a myriad of organ structures throughout the body. Many sonographers specialize in one or several modalities within this profession, following well-developed protocols established by accrediting bodies such as the American College of Radiology (ACR), the American Congress of Obstetricians and Gynecologists (ACOG), the American Institute of Ultrasound in Medicine (AIUM), the American Society of Echocardiography (ASE), and the Society for Vascular Ultrasound (SVU) to name a few. 1 While sonographers are educated and certified in specific specialties of sonography, there is little specific education or guidelines to prepare sonographers for “soft tissue” sonography. These are often ordered to evaluate superficial, palpable structures usually discovered specifically by patients or their physicians rather than through other diagnostic means. Soft tissue sonography often requires critical thinking skills on the part of sonographers and can be performed in inpatient as well as outpatient settings. The following case series details sonograms ordered through an Urgent Care (UC) facility where patients either felt a palpable mass or experienced pain or discomfort due to a superficial structure.
Case 1
A 30-year-old man presented to the UC department with a palpable lump in the left side of the neck. The patient did not report any pain and stated the lump had been there for about 1 year. The medical staff ordered a soft tissue sonogram of the left neck. A General Electric LOGIQ S8 ultrasound equipment system (GE Healthcare, Wauwatosa, WI) was used with a ML6-15 linear-array transducer. A hyperechoic structure measuring 5.7 × 0.9 × 1.8 cm3 (see Figure 1A) was noted anterior to the left lobe of the thyroid. This mass appeared to be continuous and encapsulated within the sternocleidomastoid muscle. Color Doppler evaluation demonstrated that there was no notable arterial or venous flow within the mass (see Figure 1B). A split-screen image was produced to demonstrate the unilaterality of the mass (see Figure 1C). The radiology report described the structure as a probable lipoma.
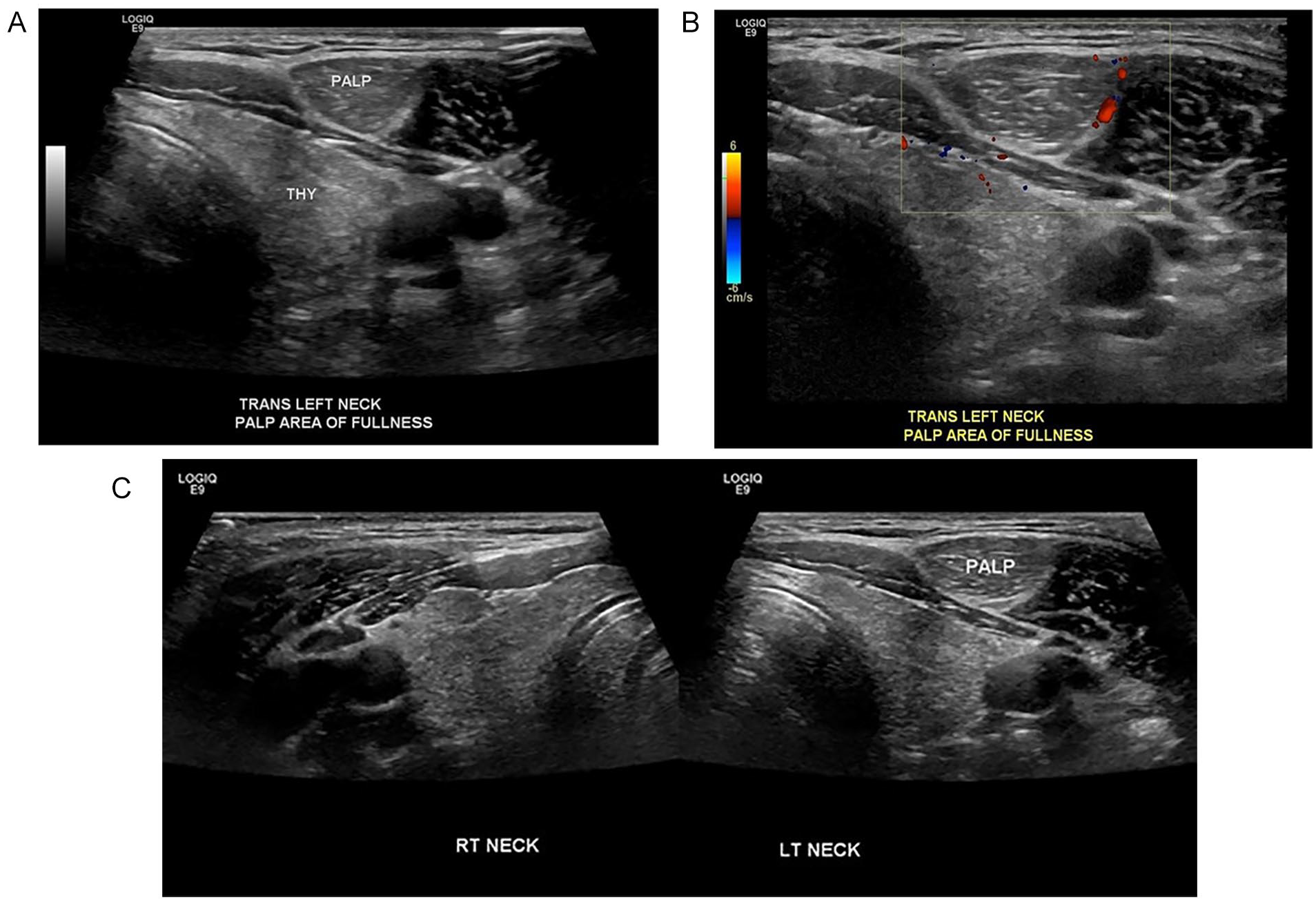
(A) This sonographic image demonstrates a palpable lump in the patient’s left neck that was diagnosed as an intramuscular lipoma of the sternocleidomastoid muscle. (B) This sonographic image shows the lipoma with color Doppler around the periphery of the mass. (C) This split-screen sonogram demonstrates the unilaterality of the mass as it does not appear in the right sternocleidomastoid muscle.
Case 2
A 56-year-old woman presented to the UC with a palpable mass over the midline of the forehead. The lump was hard and non-mobile. She stated there was no pain associated with the lump, that it had been there for about 5 to 6 years, and she was thinking of having it removed. A sonogram was ordered by the medical staff. A General Electric LOGIQ S8 ultrasound equipment system was used with a ML6-15 linear-array transducer. The sonogram was performed over the palpable area of the midline of the forehead. There was a corresponding smoothly marginated prominence of the outer table of the calvarium, measuring 0.7 × 0.7 cm2 (Figure 2A), that caused shadowing. The mass was elevated 0.3 cm above the normal calvarial contour. This caused elevation of the overlying scalp, which otherwise appeared within normal limits. There was also arterial flow noted within the structure (see Figure 2B). The radiology report described this mass was a probable osteoma. The report also included a recommendation for computed tomography (CT) correlation for further confirmation.
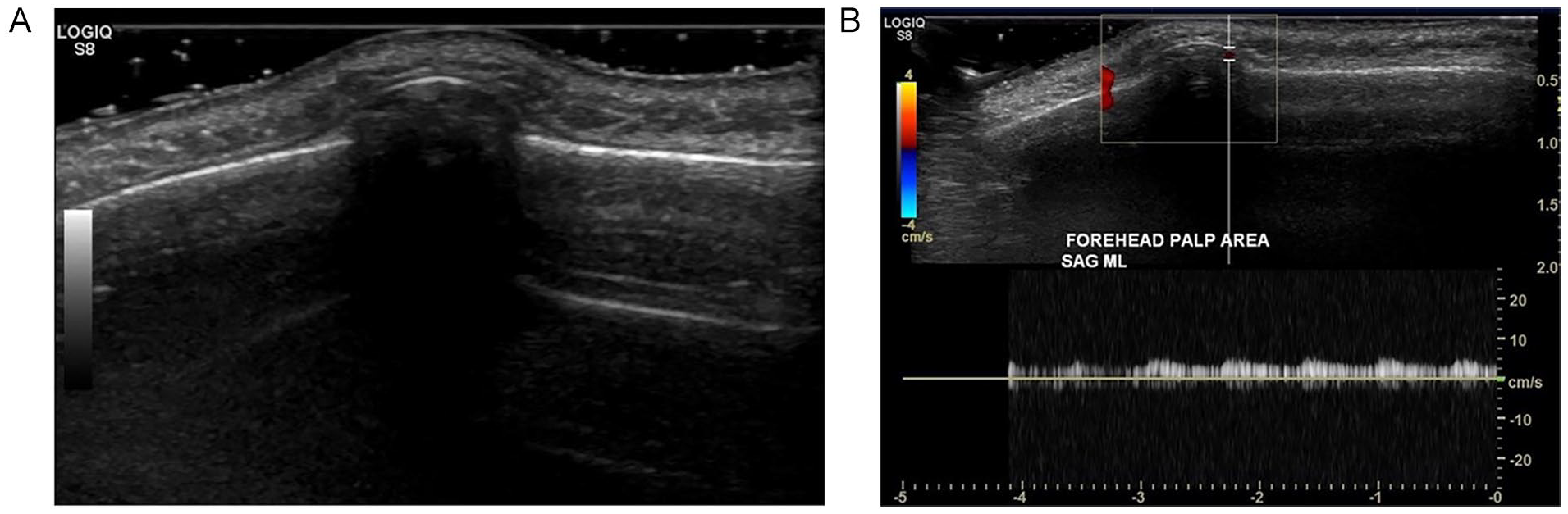
(A) This sonogram demonstrates the continuity of the mass with the frontal bone. (B) This sonographic image represents blood flow within the mass using color and pulse wave Doppler.
Case 3
A 32-year-old woman presented to the UC with pain, swelling, and erythema in the left perianal region. A sonogram was performed on the patient using a General Electric LOGIQ S8 ultrasound equipment system with a ML6-15 linear-array transducer. The sonogram demonstrated a small area of heterogeneous tissue measuring 1.6 × 1.5 × 2.0 cm3 (see Figure 3A). The structure was seen 0.5 cm deep to the skin surface, with blood flow surrounding the tissue, and was suggested in the radiology report to represent a developing abscess. A superficial wound culture was ordered. The lab report ultimately described a mixed skin flora, including multiple gram negative rods and heavy growth. The patient was treated by the medical staff with antibiotics and discharged.
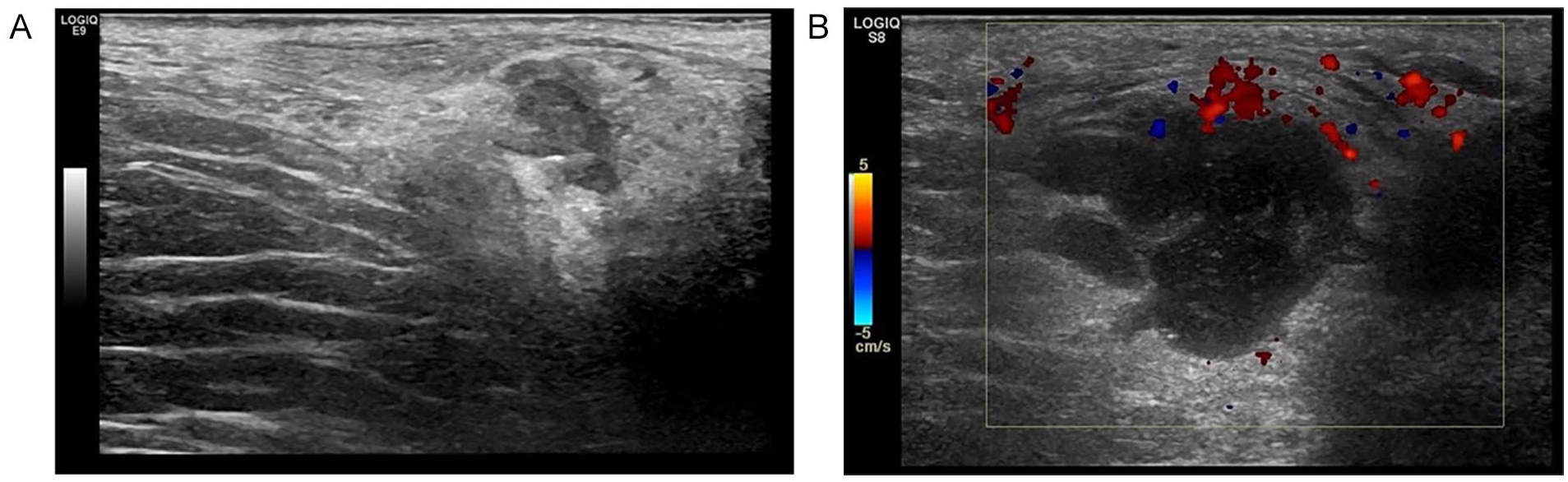
(A) The hypoechoic mass demonstrated with sonography indicates a perianal abscess captured during the initial Urgent Care visit. (B) Sonography of the perianal abscess at 1-week follow-up with hyperemic flow around the periphery of the abscess. In the 1-week follow-up image, the abscess has increased in size significantly.
Seven days later, the patient returned to the UC with more pain and swelling in the left perianal region. A sonogram was performed on the patient using a General Electric LOGIQ S8 ultrasound equipment system with a ML6-15 linear-array transducer. A complex cystic structure, irregular in shape, measuring 3.2 × 1.9 × 2.9 cm3 was visualized. The structure contained echoes, and septa, which enhanced through transmission, with blood flow demonstrated around the periphery (see Figure 3B). After the second UC visit, the patient was referred for a colorectal surgical consult and was scheduled for an anal fistulotomy. One month later, as it was believed, this structure was a perianal abscess that ultimately had become an anal fistula.
Case 4
A 52-year-old man presented to UC with a hard, tubular, palpable mass right lateral to the scrotum. He expressed to the sonographer that he had recently started bicycling and was doing it almost every day for most of the past year. The patient noticed that the mass was in the area where the bicycle seat made contact with the perineal region. The medical staff ordered a sonogram to rule out a mass. A General Electric LOGIQ S8 ultrasound equipment system was used with a ML6-15 linear-array transducer. In the region of concern, a tubular hypoechoic structure with internal echoes was visualized measuring 4.0 × 0.9 × 1.0 cm3 (see Figure 4A and 4B). No internal flow was recognized in the structure. The radiology report proposed that this structure was likely a thrombosed vein.
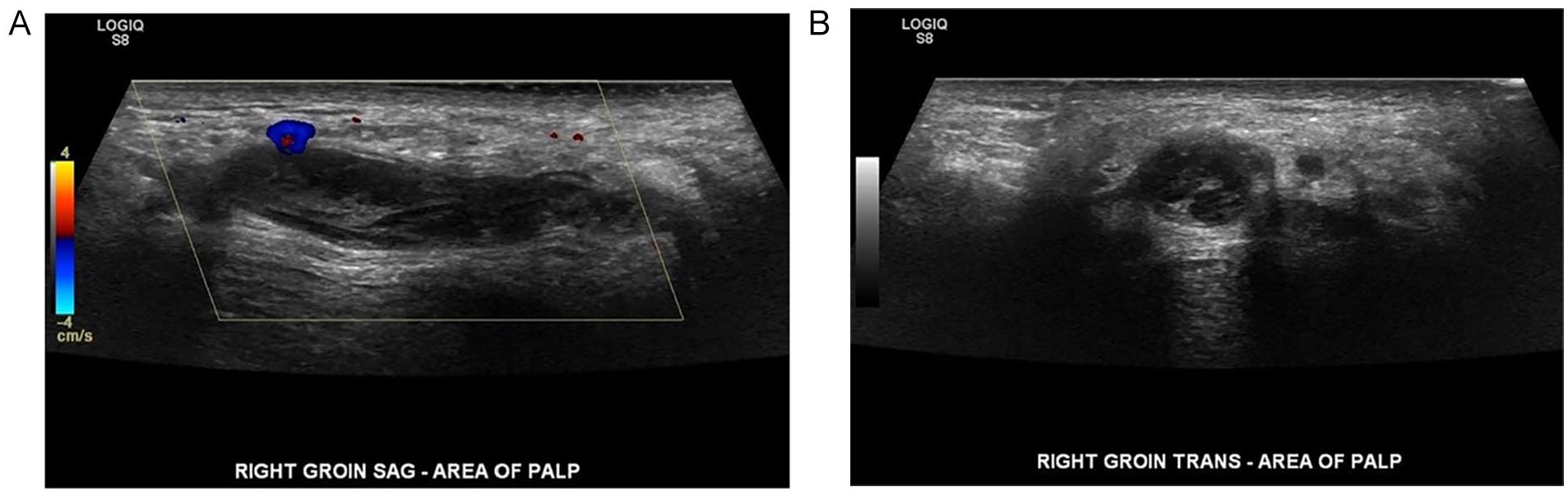
(A) A sagittal sonographic image of superficial thrombophlebitis right lateral to the scrotum with color Doppler demonstrating thrombosis of the vein. (B) A transverse sonographic image of superficial thrombophlebitis right lateral to the scrotum.
Case 5
A 29-year-old woman presented to UC with swelling, discomfort, and a palpable, soft protrusion in the right inguinal region. She expressed to the sonographer that the palpable area and discomfort were greater while standing. She was 7-months pregnant during the time of the examination, gravida 1, para 0. She stated she was an emergency room nurse, who was working 14- to 16-hour shifts and frequently standing on her feet. The medical staff were concerned this mass might be an inguinal hernia and ordered a soft tissue sonogram. A General Electric LOGIQ E9 ultrasound equipment system was used with a ML6-15 linear-array transducer. The radiology report described a sonogram which was performed with (see Figure 5D) and without Valsava maneuver (see Figure 5C), supine (see Figure 5A), and standing. There was no visualized hernia or evidence of lymphadenopathy. There were small, benign-appearing lymph nodes visualized in the region measuring 0.9 × 0.4 cm2 and 1.0 × 0.5 cm2 (see Figure 5E). There were subcutaneous/superficial veins seen within the inguinal region, which showed color flow and were compressible. These were diagnosed as right inguinal superficial subcutaneous veins, which were patent and appeared mildly dilated.
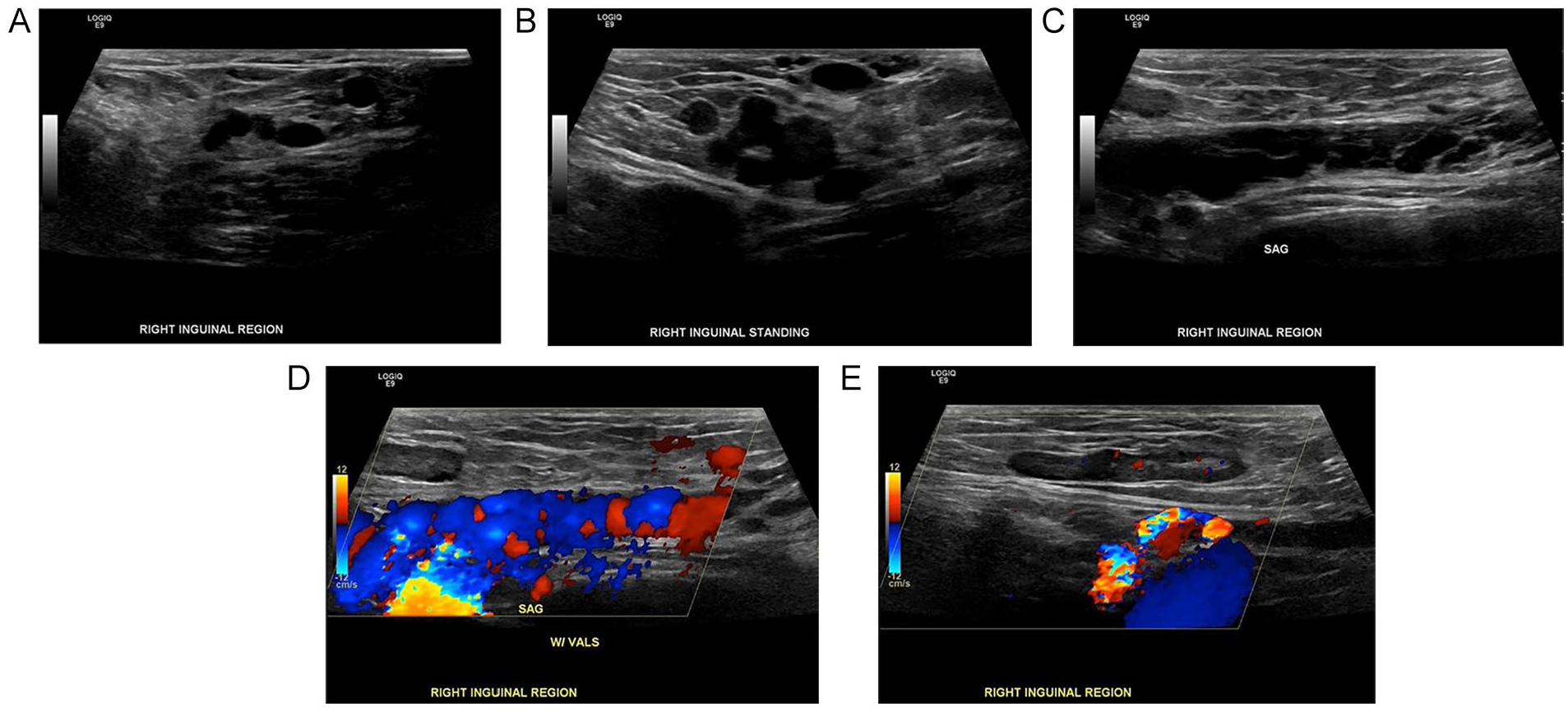
(A) A transverse sonographic image of the right inguinal region showing superficial veins with the patient in a supine position. (B) A transverse sonographic image of the right inguinal region showing superficial veins with the patient in a standing position. The diameter of the veins has increased significantly in diameter. (C) A sagittal sonographic image of the inguinal region demonstrating the network of superficial veins in the inguinal region. (D) A color Doppler sonogram captured in the sagittal imaging plane. (E) A sagittal sonographic image that demonstrated the largest lymph node in the inguinal region.
Discussion
Soft tissue sonography is a type of examination that can be performed in both inpatient and outpatient settings. With regard to these cases, outpatient, or more specifically UC settings are the focus. It has been suggested that an aging population, plus the unavailability of primary care providers in some regions, has led to an increase in more UC and emergency department (ED) visits overall. 2 In the United States, non-routine, unexpected health challenges are cause for patients to visit an ED, while lower-acuity complaints can be evaluated in an UC setting. 3 Compared with the ED, UCs provide potentially lower volume settings that also require lower costs to operate. 3 There has been an increase in ED visits for decades. Some of the problems affiliated with EDs include crowding, increased costs, long wait times, and overstretched services. Therefore, UCs often appear more attractive to patients with medical needs more similar to those of primary care. 2
Several UCs have offered radiologic services, but more recently sonographic examinations are also in demand in UCs. Sonography is an attractive imaging modality due to its low cost and lack of ionizing radiation. 4 Some UC facilities have adapted the practice of performing sonograms within the facility rather than referring to an outside hospital or imaging center. An advantage of performing sonograms within UC is “referral avoidance.” 5 Treatment of patients can be delivered more efficiently and effectively when the diagnosis can be achieved while patients are still present within the facility. In the facility where the cases in this article were obtained, the model is one of an outpatient multi-specialty medical group. This medical group is home to 77 specialties and services. Some of these services include family medicine, obstetrics and gynecology, cardiology, vascular surgery, breast surgery, pediatrics, infectious disease management, urology, and behavioral health, to name a few. Other medical groups in the region have adopted similar business models. It is through this model that sonography, which is part of the radiology department, is present on weekdays, evenings, and weekends to provide diagnostic imaging services to many specialties of which UC is included.
The incidence of soft tissue masses is estimated to be around 3 per 1000 per year. 4 In all, 98% to 99% of these masses are found to be benign, and many of them represent lipomas. 4 Lipoma is the most common benign soft tissue mass, with an estimated occurrence of 1 of 100 per year, occurring in the fourth and sixth decade of life, and they present as soft, nontender, and mobile.4,6 The utilization of sonography can assist in differentiating a deep from a superficial lipoma and lipomas from other clinically similar pathologies such as hamartomas, fibromas, or ganglion cysts. 6
Soft tissue infections frequently motivate people to seek care in UCs. Infections diagnosed with superficial soft tissue sonography include cellulitis and cutaneous abscesses, leading physicians to seek to make a distinction between the two. 7 While both may present with erythema, warmth, swelling, and tenderness, the therapeutic interventions for the two diagnoses are quite different. Therapeutic interventions for localized abscesses often include incision and drainage, while cellulitis is treated primarily with either oral or intravenous antibiotics.7,8
Osteomas are benign, slow-growing, bony tumors that sometimes appear in the midfacial area most commonly in the second to fifth decade of life. 9 They are more common in men compared with women. Osteomas are typically small in size, and only about 5% of them become symptomatic. 9 Treatment for osteomas include anti-inflammatory drugs (NSAIDs) as well as surgical treatments. 10
Anal abscesses are common conditions in which management is usually straightforward and based on sound knowledge of the anatomy of the anorectum. 11 The external sphincter is a continuation of the pelvic floor musculature (e.g., levator ani, puborectalis, and inner circular muscle of rectum) and the internal sphincter is a continuation of the inner circular muscle layer of the rectum. 11 The cause of anal abscesses has been described by Eisenhammer and Parks in which an intramuscular gland becomes infected and then the subsequent infection leads to an obstruction of its connecting duct, which prevents drainage. 11 Due to this configuration, treatment will often require surgical drainage under general anesthesia.
Superficial thrombophlebitis (ST) is an inflammatory condition of a superficial vein in the body with evidence of thrombus in the involved segment.12,13 While the exact incidence of ST cases is unknown, ST is most commonly found in the legs, with 60% to 80% of cases occurring in the greater saphenous vein. 14 While an ST diagnosis can be made clinically in patients presenting with erythema, pain, and a palpable cord, sonography has proved useful in differentiating ST from superficial phlebitis and determining whether or not the deep venous system is involved.12,15 In cases where ST is localized to a small segment of a superficial vein, treatment typically involves warm compress and over-the-counter medication to alleviate symptoms. In patients who have ST in close vicinity to a deep vein, anticoagulant medication may be prescribed to inhibit the thrombus from extending into adjacent veins. 15
Varicose veins located in the pelvic area, specifically of the labia majora and labia minora occur in approximately 18% to 22% of pregnant women. 16 It is thought that both an increase in progesterone levels earlier in pregnancy and compression of the inferior vena cava and pelvic veins due to an enlarged uterus later in pregnancy are two of the most common causes of pelvic varicosities.17,18 Pelvic varicosities in conjunction with other findings such as pelvic pain for 6 months and longer, painful intercourse, and postcoital discomfort can lead to a clinical diagnosis of pelvic congestion syndrome. 19 Pelvic varicosities that develop during pregnancy may resolve postpartum. However, conservative treatment with compression socks is recommended to help alleviate further dilation of the veins and to minimize damage of the vein valves.17,18
Conclusion
Several demographic factors have led to an increase in UC visits in the last several years. The utilization of sonography in UC has also become more popular in assisting in less critical diagnoses due to its low cost, lack of ionizing radiation, and its ability to target specific areas of interest. Attending physicians in the UC also often have the ability to oversee the examination in progress, and directly visualizing the area of interest, which ultimately reduces the number of outside referrals for patients with palpable, soft tissue complaints.
In four of the five cases presented in this article, patients arrived at UC with complaints of palpable lumps allowing sonographers to perform targeted examinations on the area of interest. Measurements were obtained for all soft tissue masses found in the palpable areas and in some cases, the utilization of color and pulsed wave Doppler allowed for further characterization of the lesions as vascular or non-vascular. Within the UC setting, where medical imaging is available, physicians also have the ability to confirm diagnosis or obtain more diagnostic information by using other modalities, such as CT. While there is currently no recommended protocol for imaging the wide range of soft tissue structures, methodical and comprehensive sonographic imaging led to several different diagnoses in the cases above.
It has been stated in this article that soft tissue sonograms typically do not follow a rigid protocol. One could suggest that loose soft tissue protocols be included in sonography departments as a guide to encourage sonographers to obtain orthogonal images for three-dimensional comparison of soft tissue structures. It could also be suggested that sonographers include color and/or pulsed wave Doppler evaluation, and machine optimization, to differentiate between cystic, solid, complex, vascular, and non-vascular structures. Furthermore, it could be suggested that unilaterality of soft tissue masses be delineated by demonstration of contralateral regions when applicable. However, given the premise that sonography remains an incredibly operator-dependent imaging modality, it may be more salient to emphasize that sonographers must rely on critical thinking skills as much as, or sometimes more than, protocols when making decisions on how to best present their findings. Critical thinking is as paramount to sonographers’ skill set as their ability to use and optimize their ultrasound equipment systems.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Permission Statement
Permission was granted by the patient to publish the case.