
Abstract
A 56-year-old woman presented in 2006 with symptomatic primary varicose veins in her right leg. Venous duplex ultrasonography at that time showed what appeared to be “neovascular tissue” around the saphenofemoral junction. However, there had been no previous trauma or surgery in this area. This appearance has subsequently been described as primary avalvular varicose anomalies. She underwent endovenous treatment at that time. In 2018, she presented with symptomatic recurrent varicose veins of the same leg. Venous duplex ultrasonography showed successful ablation of the great saphenous and anterior accessory saphenous veins. All of the recurrent venous reflux was arising from the primary avalvular varicose anomalies. This report shows that primary avalvular varicose anomalies is a previously unreported cause of recurrent varicose veins and leads us to suggest that if found, treatment of the primary avalvular varicose anomalies should be considered at the primary procedure.
Keywords
Introduction
Varicose veins arising from truncal veins affects approximately one-third of adults aged 18–64. 1 A major or recurrence after open surgery is “neovascularisation” in the groin, which is the re-growth of multiple small incompetent veins, re-connecting the ends of the remaining veins after treatment, resulting in the re-establishment of pathological venous reflux. 2 If this process continues down the tract of the truncal vein that has been stripped, it is called “strip-tract revascularisation.”3,4
In 2013, the National Institute for Health and Care Excellence (NICE) produced clinical guidelines (CG168) that recommended endothermal ablation of truncal veins, and foam sclerotherapy above open surgery. 5 Endovenous thermal ablation is predominantly performed as radiofrequency or endovenous laser ablation. We have reported that radiofrequency ablation shows no neovascularisation post-operatively 6 and others have reported a very low (1%) rate after endovenous laser ablation. 7
The diagnosis of neovascular tissue after varicose veins surgery is usually made on duplex ultrasonography, showing the “presence of multiple new small tortuous veins in anatomic proximity to a previous venous intervention.” 8 In 2014, we reported that we had found similar vessels in 4.6% of patients who have not had any previous surgery or intervention in the area and we called this phenomenon “primary avalvular varicose anomalies” (PAVA). 9 However, at that time, we did not know if PAVA would be an incidental finding or whether it might have a role in the development of recurrent varicose veins if left untreated.
Case
A 56-year-old woman presented in January 2018 with right leg recurrent varicose veins, causing “heaviness” on standing and swelling of the ankle (Clinical, etiological, anatomical and pathological (CEAP) clinical classification C3). In 2006, she had previously presented with symptomatic varicose veins of the right leg. At that stage, a venous duplex ultrasound scan has shown reflux in her great saphenous vein (GSV), anterior accessory saphenous vein (AASV) with two incompetent perforating veins (IPV) distally. In addition, the duplex reported the presence of a “mass of veins appearance of gross neovascular tissue but no previous surgery” in the right groin that showed reflux. As this looked remarkably like neovascular tissue, the patient was questioned carefully. She denied having had any previous surgical or interventional radiological procedure in her right groin and there was no medical history nor scars on the skin to suggest otherwise. Also, here was no history of any trauma or extensive bruising in this area.
In 2006, the patient had been treated with radiofrequency ablation of the GSV and AASV, and both IPVs were closed with by transluminal occlusion of perforators (TRLOP). 10 The surface varicosities were removed by stab phlebectomy. The “neovascular type” tissue in the groin was left untreated, as it was of unknown clinical significance at that time.
In 2018, she presented with a 2-year history of recurrent varicose veins in her right thigh, medial right knee and upper right leg (Figure 1). She complained of heaviness of the leg, aching on standing and swelling of the ankle (CEAP clinical classification C3). Venous duplex ultrasonography showed that the previously ablated GSV and AASV had atrophied, as had both treated IPVs. The new recurrent varicose veins were found to be arising from the profuse PAVA tissue in the groin (Figure 2(a) and (b)). The PAVA tissue was predominantly in the groin, within the saphenous fascia (Figure 2(a)) and associated with a lymph node (Figure 2(b)) and so could be classified as both “truncal” and “lymph node” pattern. 9 There was no pelvic vein reflux and no communication with the inferior epigastric vein.

Photograph of right leg showing recurrent varicose veins arising from groin.
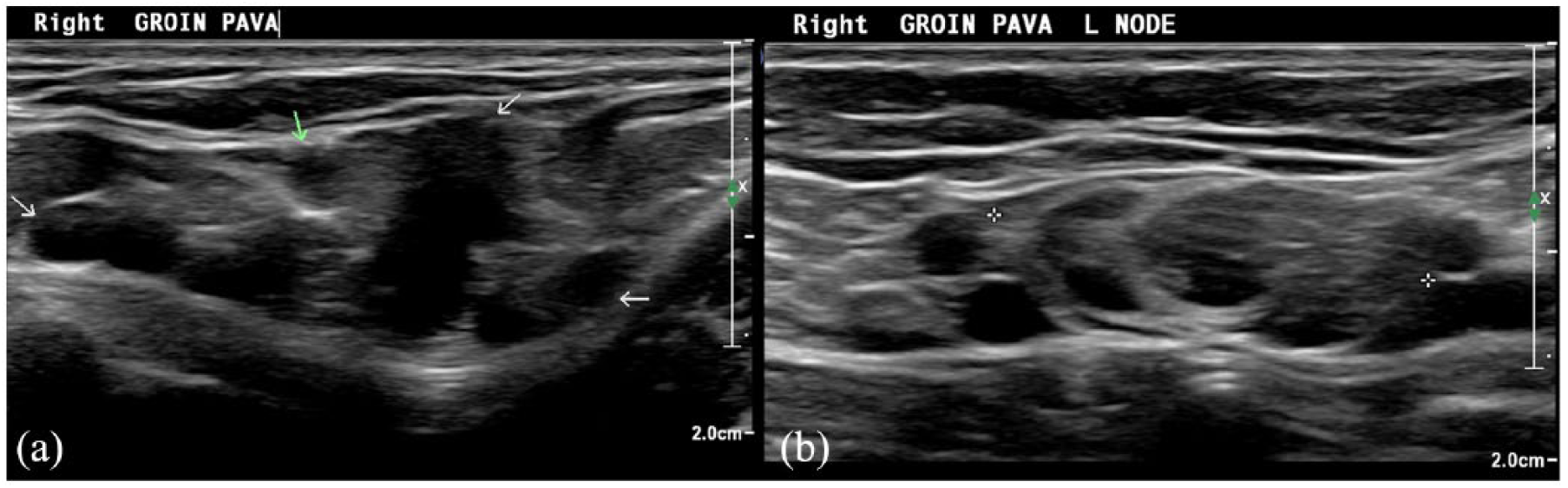
(a) Venous ultrasound showing primary avalvular varicose anomalies (PAVA) tissue in right groin within the saphenous fascia—GSV and AASV previously ablated—arrows showing the different PAVA vessels. (b) Same patient showing PAVA passing into and out of a lymph node (lymph node between crosses).
Discussion
PAVA was first described in 2014 as “a phenomenon in patients with primary varicose veins that resembles neovascular tissue in postsurgical recurrences.” 9 On venous duplex ultrasonography, PAVA is distinct from tributaries, competent or incompetent, as it appears as a serpiginous mass of thin walled veins showing reflux, winding around truncal veins or through lymph nodes.
In the first report of PAVA, we did not know if it had any clinical consequences or was merely an interesting finding that could be confused with neovascular tissue if not diagnosed preoperatively. Therefore, it was suggested that if PAVA was found preoperatively, it should be noted carefully to stop erroneous reporting of post-endovenous surgery “neovascularisation.” It was not thought that PAVA itself might progress or be the cause of progression of venous reflux disease.
As discussed above, endovenous radiofrequency ablation does not cause neovascularisation 6 and we have previously suggested that the reported low incidence of neovascularisation 7 after endovenous laser ablation was due to PAVA not being recognized in these patients preoperatively. 9
This case shows that PAVA, if left untreated, can be a cause of symptomatic recurrent varicose veins. As such, we would now suggest that not only should the presence of PAVA be noted at the diagnostic venous duplex ultrasound scan as we have previously recommended,9 but, if found, the treatment of PAVA should be considered at the time of the primary varicose vein procedure.
Conclusion
PAVA is a newly identified cause of recurrent varicose veins. When found in patients with symptomatic primary varicose veins, treatment of the PAVA should be considered at the primary varicose vein procedure to reduce the risks of recurrence.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Patient consent
The authors confirm that they have written consent from the patient for the reporting of this case and the use of the images for publication.