
Abstract
Systemic lupus erythematosus (SLE) is an autoimmune rheumatic disease that principally affects women in their childbearing years. Many cytokines have been implicated in regulating disease activity and the involvement of different organs in patients with SLE. The study was conducted to determine serum tumor necrosis factor alpha (TNFα) levels in SLE patients and its relation to clinically active disease and to assess the possible role of serum TNFα level in atherosclerosis. Thirty Egyptian female patients with SLE and 15 matched healthy control subjects had serum TNFα levels measured. In addition, the relation of common carotid artery intima-media thickness (CIMT) to serum TNFα was evaluated. Mean serum TNFα level of SLE patients was 48.36 ± 58.27 pg/ml, significantly different from the control group (17.62 ± 16.63 pg/ml; P = .014). There was a statistically significant difference in right carotid CIMT between SLE patients (0.06 ± 0.01 cm) and the control group (0.054 ± 0.009; P = .002). There was also a statistically significant difference in left carotid CIMT between lupus nephritis patients (0.07 ± 0.01) and non–lupus nephritis patients (0.06 ± 0.01; P = .027). These data indicate the activation of immune response in SLE patients suggested by their high levels of TNFα. Increased CITM in lupus patients was not related to TNFα and the lipid profile, suggesting an underlying etiology for atherosclerosis in lupus patients other than those factors. High CIMT in nephritis patients denote the role of nephritis in atherosclerosis.
Introduction
Systemic lupus erythematosus (SLE) is a chronic multisystem autoimmune disease with a broad range of clinical manifestations. Although the pathogenesis is believed to lie in the dysregulation of the immune system, the involvement of various organ systems often leads to secondary morbidities resulting in renal failure, hypertension, or central nervous system (CNS) disorders. More recently it has becoming increasingly clear that accelerated atherosclerosis associated with SLE may contribute to premature mortality.1-3
Atherosclerosis has been shown to be enhanced in autoimmune diseases; noninvasive investigations show increases in intima-media thickness, carotid plaque, and coronary artery calcifications in patients with antiphospholipid syndrome (APS), SLE, and rheumatoid arthritis (RA) compared to controls. 2 Cytokines are master regulators of the innate and adaptive immune response and, unsurprisingly, are known to regulate and coordinate many stages of atherosclerosis. Many cytokines, such as interleukin (IL)-1, IL-6, IL-10; interferon gamma (IFNγ); and tumor necrosis factor alpha (TNFα), are highly expressed in atherosclerotic regions and exhibit both pro- and anti-atherogenic actions. 3 TNFα in particular has been shown to be both a proinflammatory and an immunoregulatory cytokine.4-8 The elevated circulating levels of TNFα found in SLE patients have been found to be associated with high triglyceride and low high density lipoprotein (HDL) levels. 5
Carotid intima-media thickness (CIMT) measurements have increasingly been used in observational and intervention studies.9-18 CIMT has been applied as an outcome variable in studies on the determinants of atherosclerosis, and it has been employed as an exposure variable in studies on the prognostic value of CIMT in order to predict coronary artery disease (CAD) and stroke. Changes in CIMT over time as a marker for atherosclerosis progression and possible change in cardiovascular risk have been used in intervention studies as a primary outcome variable aimed at assessing the effects of risk factor interventions. More recently, reports on the risk factors for progression of CIMT have become available from observational studies. The current widespread application of CIMT measurements has been based on the validity, standardization, and reproducibility of the measurement and the evidence an increased CIMT can be regarded as a marker of atherosclerosis and of increased cardiovascular risk. A number of these studies have specifically addressed SLE patients.15-17
Methods
Thirty consecutive female Egyptian SLE patients mean age 27.4 ± 8.7 years were chosen according to the American College of Rheumatology criteria 19 from the outpatient rheumatology and immunological clinic. The local ethics committee of the Cairo University Faculty of Medicine approved the study, all patients were informed about the procedure, and a verbal consent was taken. Clinical activity was assessed at the time of venipuncture using the systemic lupus erythematosus disease activity index (SLEDAI). Fifteen age-matched healthy female control subjects from a similar ethnic background were also recruited and included in the study.
A full clinical history was obtained for all subjects, and laboratory testing was done to measure complete blood count, erythrocyte sedimentation rate, C-reactive protein, Complements C3 and C4, serum creatinine, serum cholesterol, serum triglyceride, low-density lipoprotein (LDL) and HDL cholesterol, urinanalysis, 24-hour urinary protein, anti–double-stranded deoxyribonecleic acid (anti-dsDNA) antibodies, and serum TNFα. In addition to the presence or absence of SLE, patients were further classified as to the presence or absence of dyslipidemia and lupus nephritis.
All subjects had bilateral carotid artery duplex sonography to measure the intima-media thickness of the distal common carotid as a single point measurement at the site of maximum thickness (Figure 1), assess for any atherosclerotic plaque, and record the peak systolic velocity (PSV), end diastolic velocity (EDV), and resistive index (RI) of the internal carotid artery. Gray-scale imaging and spectral Doppler velocity measurements were done according to our standardized laboratory protocol using an HD5000 system with a 7.5 MHz probe (Philips Ultrasound, Bothel, Washington). The same operator interpreted all studies in a blinded fashion.
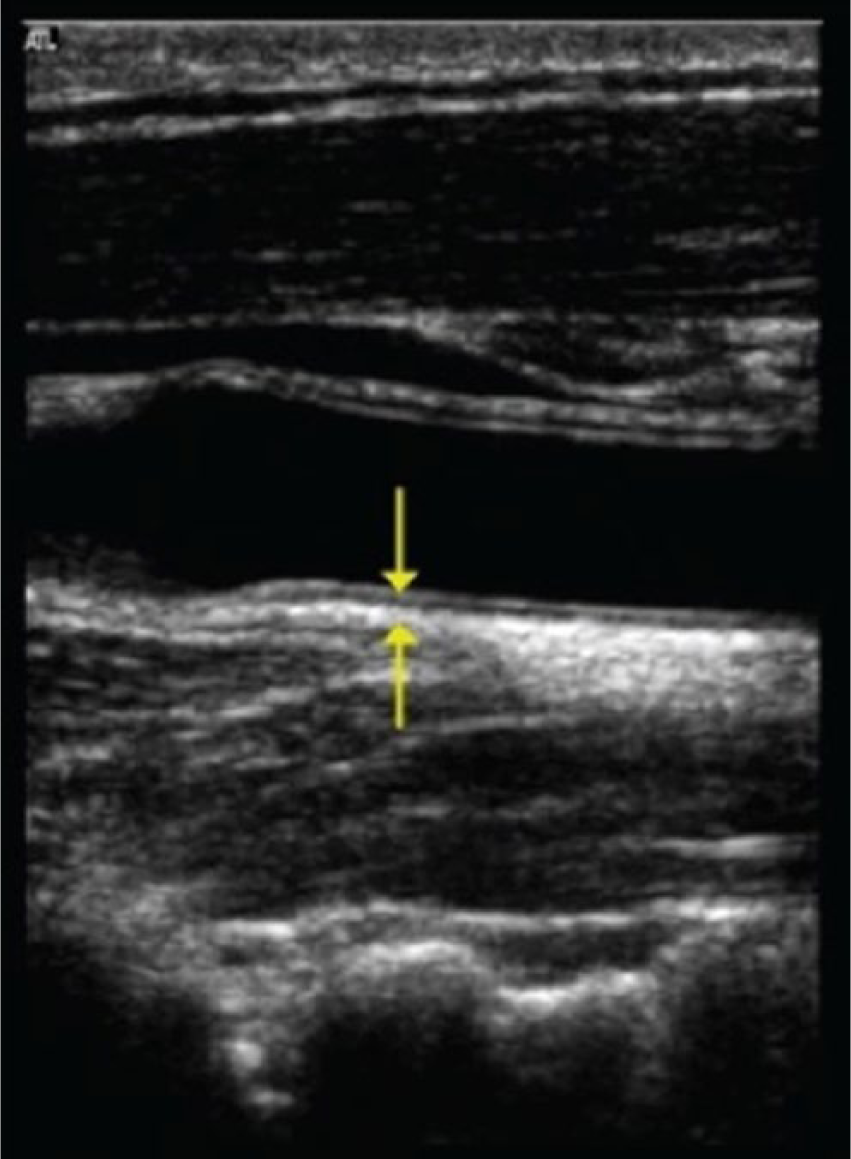
Sagittal gray-scale image of the distal common carotid artery showing the single point measurement technique for intima-media thickness.
The data were coded and analyzed using the statistical package SPSS, Version 15 (IBM, Cary, North Carolina). The data were summarized using descriptive statistics of mean, standard deviation, minimal and maximum values for continuous quantitative variables, and number and percentage for qualitative values. Statistical differences between groups were tested using the chi-square test for qualitative variables, independent sample Student t test for quantitative normally distributed variables, and the nonparametric Mann-Whitney test for quantitative variables, which were not normally distributed. Correlations were done to test for linear relations between variables. A P value of .05 was considered to indicate a significant difference between groups.
Results
Twelve of the 30 SLE patients presented with chronic dermatologic changes characteristic of discoid lupus. Clinical activity as indicated by the SLEDAI score ranged from 2 to 30, with a mean of 8.73 ± 7.45. Anemia, defined as a hemoglobin below 12 gm/dl, was found in 22 patients (73.3%), with values ranging from 9.2 to 11.8 gm/dl. Leucopenia, a total leukocyte count below 4 × 103 cells/microl, was found in 6 patients (20%), ranging from 1.7 to 3.3 × 103 cells/microl. Thrombocytopenia, a platelet count below 150 × 103 cells/microl, was present in only 1 patient (3.3%). Dyslipidemia was noted in 10 patients (33.3%) and lupus nephritis in 11 patients (36.7%).
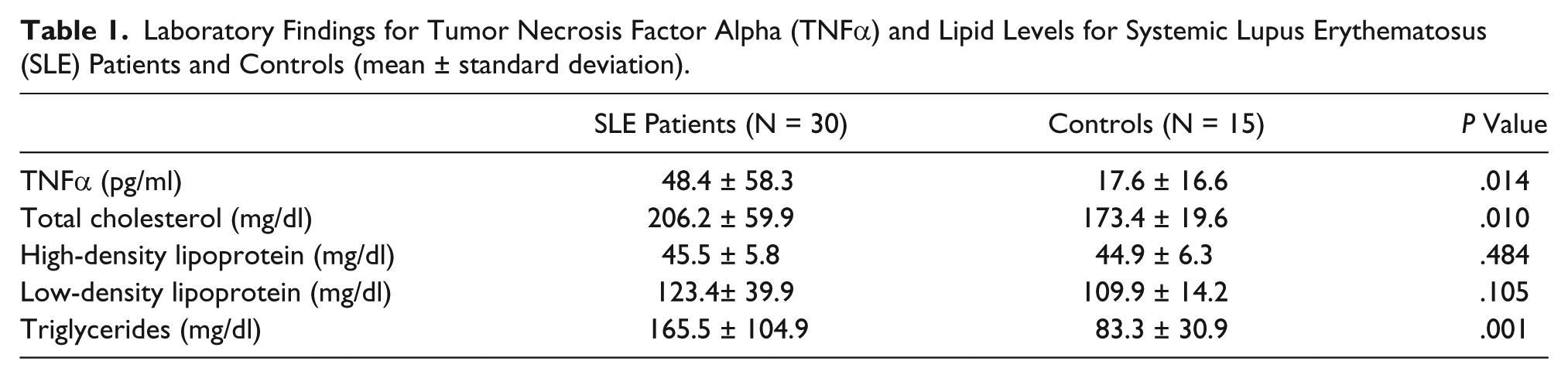
TNFα and serum lipid measurements for SLE patients and controls are shown in Table 1. The mean serum TNFα level in patients with SLE was 48.4 ± 58.3 pg/ml, significantly higher than that found in the control group (17.6 ± 16.6 pg/ml; P = .014). There also was a significant difference in total serum cholesterol level and serum triglyceride level between SLE patients and controls, with higher levels in the patient group, as shown in the table. A significant difference was found in the right carotid artery intima-media thickness between SLE patients (0.06 ± 0.01 cm) and the control group (0.054 ± 0.009; P = .002) (Table 2). Left internal carotid artery peak systolic velocity was elevated in the control group compared to SLE patients, but no other significant differences were seen in any duplex sonography-derived parameters between the 2 groups.
Laboratory Findings for Tumor Necrosis Factor Alpha (TNFα) and Lipid Levels for Systemic Lupus Erythematosus (SLE) Patients and Controls (mean ± standard deviation).
Comparison of Duplex Sonography Findings for Systemic Lupus Erythematosus (SLE) Patients and Controls (mean ± standard deviation).
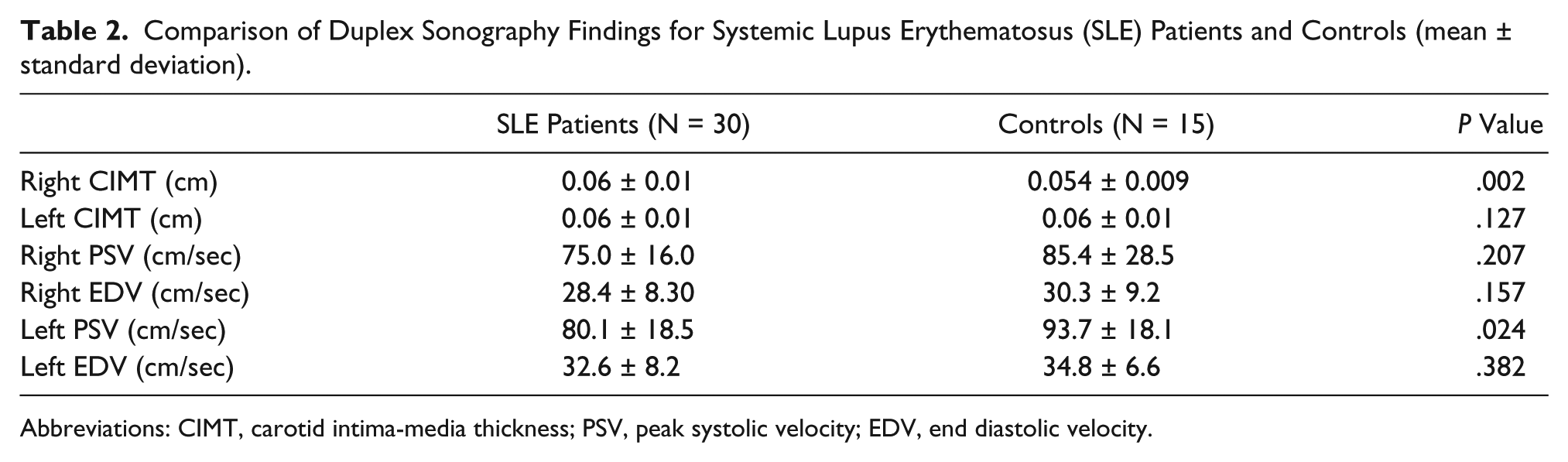
Abbreviations: CIMT, carotid intima-media thickness; PSV, peak systolic velocity; EDV, end diastolic velocity.
For SLE patients, there was significant correlation between SLE activity index scores (SLEDAI) and total cholesterol level, low-density lipoprotein cholesterol levels, 24-hour urinary protein, erythrocyte sedimentation rate, C-reactive protein, Complement3, and left carotid intima media thickness, as shown in Tables 3 and 4. However, there was no correlation between serum TNFα levels and any of the other laboratory findings or duplex sonography measurements. There were also no significant differences in serum TNFα levels between dyslipidemic SLE patients and non-dyslipidemic SLE patients (Table 5), nor for patients with and without lupus nephritis (Table 6). The left common carotid artery intima-media thickness was significantly larger in patients with lupus nephritis compared to those without (Table 6); no other duplex sonography measurements showed any significant differences when comparing dyslipidemic with non-dyslipidemic patients and patients with and without lupus nephritis.
Correlation of Laboratory Test Findings With Systemic Lupus Erythematosus Activity Index Scores (SLEDAI) and Serum TNFα Levels in Patients.
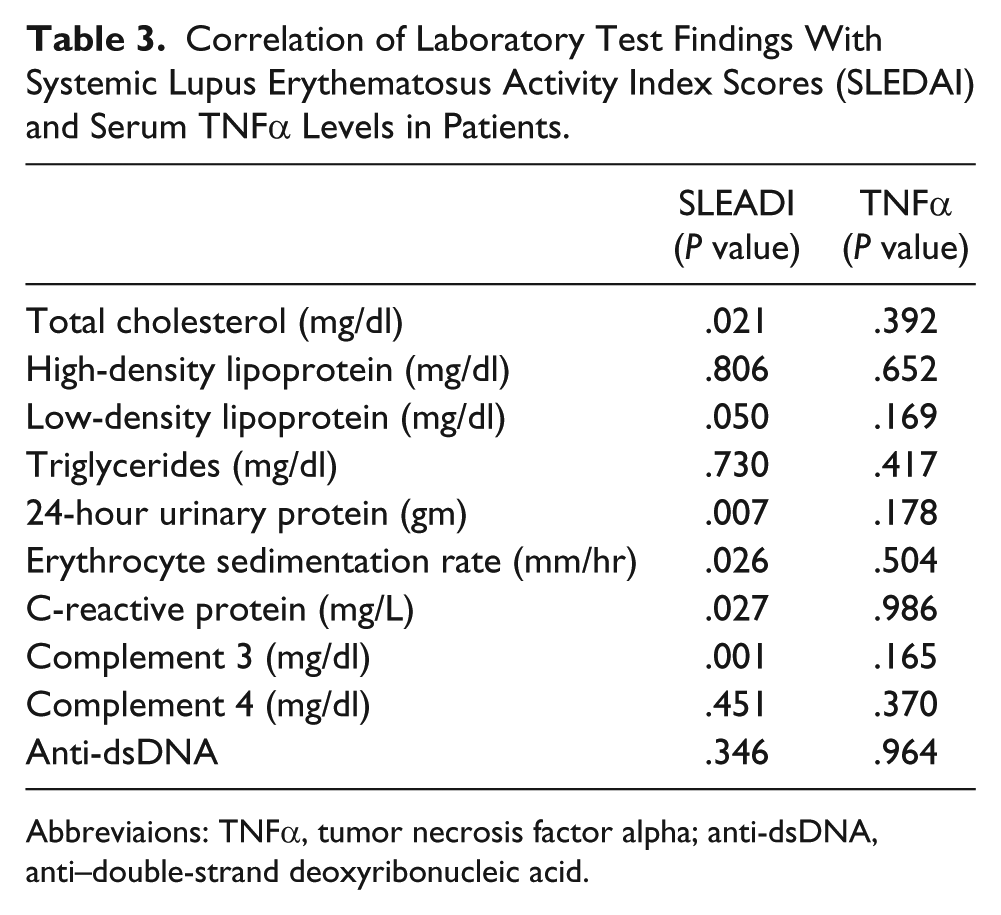
Abbreviaions: TNFα, tumor necrosis factor alpha; anti-dsDNA, anti–double-strand deoxyribonucleic acid.
Correlation of Duplex Sonography Measurements With Systemic Lupus Erythematosus Activity Index Scores (SLEDAI) and Serum TNFα Levels in Patients.
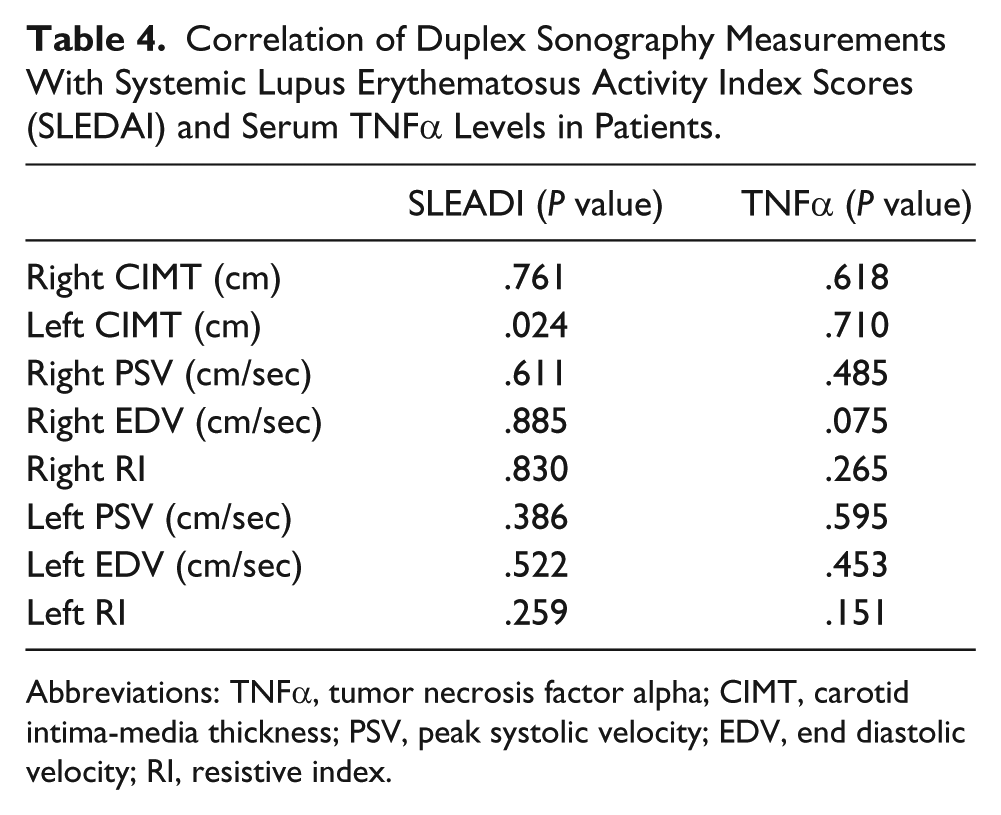
Abbreviations: TNFα, tumor necrosis factor alpha; CIMT, carotid intima-media thickness; PSV, peak systolic velocity; EDV, end diastolic velocity; RI, resistive index.
Results of TNFα Levels and Duplex Sonography Findings (mean ± standard deviation) for Systemic Lupus Erythematosus (SLE) Patients With and Without Dyslipidemia.
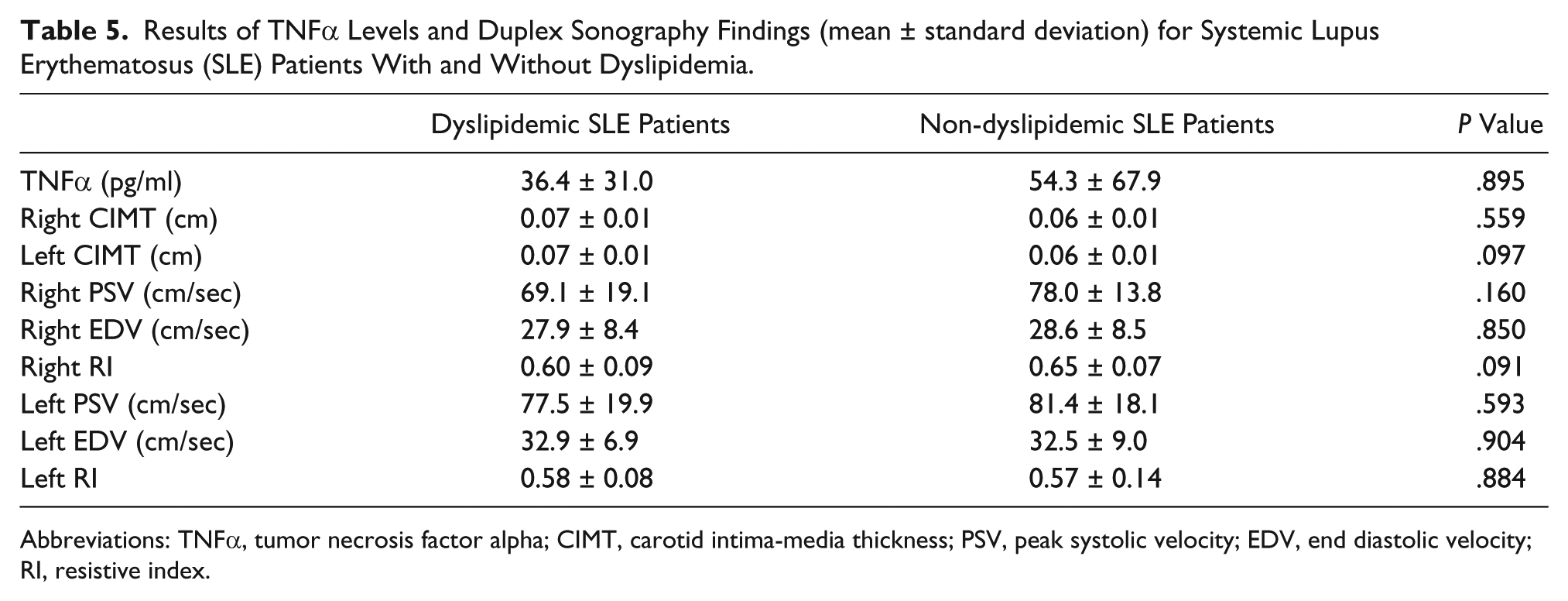
Abbreviations: TNFα, tumor necrosis factor alpha; CIMT, carotid intima-media thickness; PSV, peak systolic velocity; EDV, end diastolic velocity; RI, resistive index.
Results of TNFα Levels and Duplex Sonography Findings (mean ± standard deviation) for Systemic Lupus Erythematosus (SLE) Patients With and Without Lupus Nephritis.
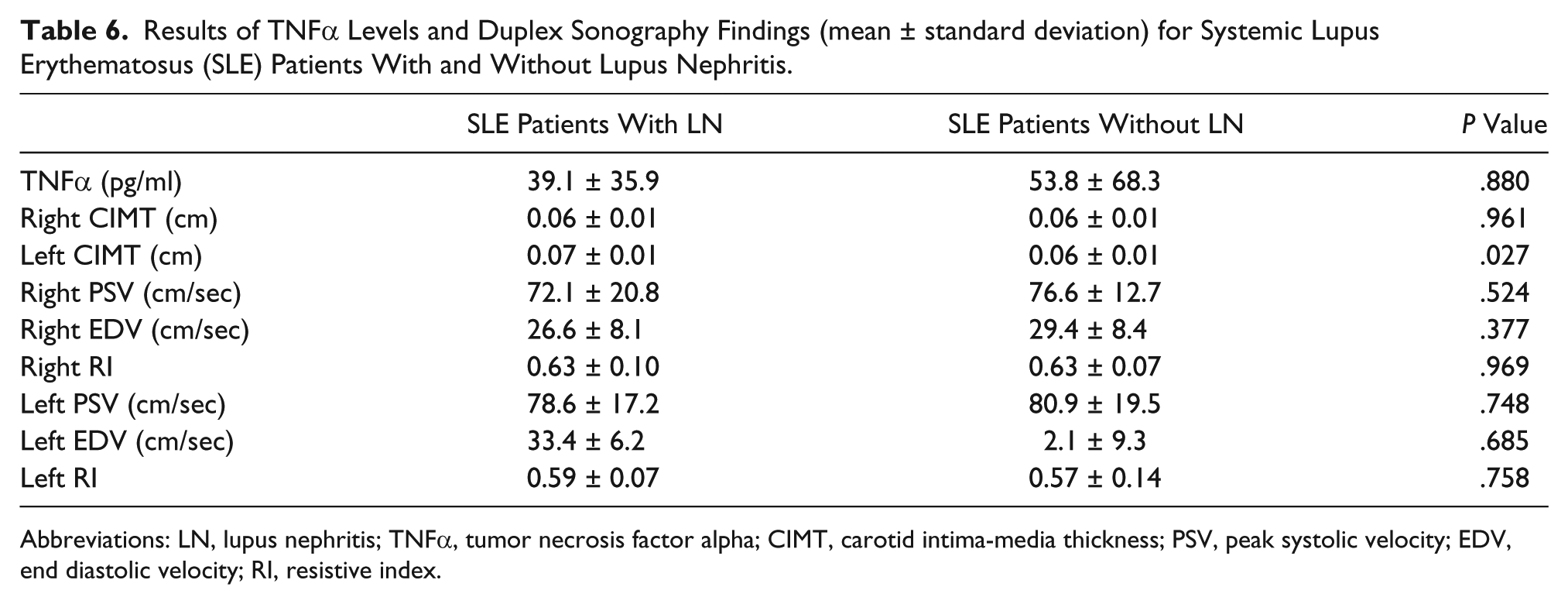
Abbreviations: LN, lupus nephritis; TNFα, tumor necrosis factor alpha; CIMT, carotid intima-media thickness; PSV, peak systolic velocity; EDV, end diastolic velocity; RI, resistive index.
Discussion
The tumor necrosis factor family of cytokines, originally characterized by their ability to induce tumor cell apoptosis and cachexia, are now considered central mediators of a broad range of biological activities. The first 2 of these factors identified were tumor necrosis factor (TNF, originally called TNF alpha) and lymphotoxin (LT) alpha. The activities of the TNF family are now known to encompass beneficial effects for the host in inflammation and in protective immune responses against a variety of infectious pathogens. TNF family members on the other hand also exert host-damaging effects in sepsis, tumor cachexia, and autoimmune diseases. In addition, the essential roles of the core members of the TNF superfamily, LT alpha, LT beta, TNF, and TNF superfamily member 14 (TNFSF14, or LIGHT), as well as their receptors, during the organogenesis of secondary lymphoid organs and the maintenance of the architecture of lymphatic tissues is beginning to be understood. 20
Autoimmune rheumatic diseases (AIRDs) are associated with higher rates of cardiovascular morbidity and mortality, primarily secondary to accelerated atherosclerosis. This phenomenon can be attributed to traditional risk factors for atherosclerosis and use of specific drugs, such as corticosteroids, but also might be the result of other autoimmune and inflammatory mechanisms that are aggravated in AIRDs. 2 SLE is an autoimmune disease characterized by a wide variety of autoantibodies, some of which are pathogenic. In recent years it has become more evident that the polyclonal B cell activation in SLE is T-cell dependent. Tumor necrosis factor (TNF alpha) is both a proinflammatory and an immunoregulatory cytokine and has differential effects on B cells, T cells, and dendritic cells, as well as on apoptosis, the process of programmed cell death. Understanding how the immune system integrates the pleiotropic properties of TNF alpha is a challenge, particularly so in diseases like SLE. 6 Patients with SLE are known to be at high risk of cardiovascular disease (CVD), and TNFα has been implicated in the pathophysiological processes of both SLE and CVD. 5
In this study, we assessed the relationship between serum TNFα level and markers of atherosclerotic vascular disease in SLE patients to highlight the different etiology of atherosclerosis in SLE patients and to demonstrate any early changes in the carotid arteries in SLE patients. The study showed a significant elevation in serum TNFα levels in SLE patients compared to an age- and ethnic-matched control population. This finding is in agreement with the results of Svenungsson et al that showed plasma concentrations of circulating TNFα higher in SLE patients with no cardiovascular symptoms compared to population controls. 5 However, they further showed that in SLE patients with cardiovascular manifestations there was a strong positive correlation between TNFα levels and plasma triglycerides. The present study showed no significant correlation between serum TNFα levels and serum triglyceride levels in SLE patients, but this may be due to differences in patient selection as none of the patients in this study had overt signs or symptoms of cardiovascular disease.
Common carotid artery intima-media thickness has been shown to be a surrogate marker for atherosclerosis associated with cardiovascular risk factors and with cardiovascular outcomes.9-11 Although measurement of intima-media thickness is promoted as a tool for cardiovascular risk assessment in primary prevention, the incremental predictive value of the intima-media thickness over and above the value of traditional cardiovascular risk factor assessment has been questioned.13,14 The present study showed a significant increase in right carotid intima-media thickness in SLE patients compared to the control groups, in agreement with Caccipaglia et al 15 who concluded that patients with SLE, despite equivalent exposure to “traditional” cardiovascular risk factors, presented with a significantly higher mean intima-media thickness of the common carotid artery than healthy subjects.
Early atherosclerosis develops in more than one-third of SLE patients. The main risk factors of early disease are the conventional ones plus factors such as antiphospholipid antibodies, persistence of chronic inflammation, decreased glomerular filtration rate, and prednisolone therapy. Chronic inflammation, particularly the influence of lupus nephritis on the process of atherogenesis in SLE, may exacerbate other risk factors. 16 Sazliyana et al have reported that aggressive treatment of severe LN and the use of cyclosporine A as a steroid-sparing agent may have protective effects against premature atherosclerosis. 17 In the present study there was a significantly larger left carotid intima-media thickness in lupus nephritis patients than in lupus patients with no nephritis.
It is hypothesized that the elevated triglyceride levels that are prevalent in SLE patients are in part attributable to anti-lipoprotein lipase and that this lipid abnormality could contribute to the premature atherosclerosis known to be present in patients with SLE patients.5,7 The present study found a significant difference in total serum cholesterol levels and serum triglyceride levels between SLE patients and the control group. However, there was no significant difference between SLE patients and controls in their high-density lipoprotein cholesterol levels. Additionally, there was no significant difference in the mean carotid intima-media thickness between SLE patients with dyslipidemia and those without dyslipidemia. This finding raises the possibility of other significant underlying factors for atherosclerosis, with or without dyslipidemia, as evidenced by increased CIMT in patients as compared to controls.
There was a significant correlation in SLE patients between SLEDAI and a number of findings, including an increased CIMT. These results indicate that increased CIMT as a marker of atherosclerosis may be related to disease activity in SLE patients and the resulting complex serum biochemistry. A significant correlation was seen as well between SLEDAI and total cholesterol and low-density lipoprotein cholesterol, in agreement with Ardoin et al. 21 Their study on children and adolescent lupus showed that active disease is characterized by elevated triglycerides and decreased high-density lipoprotein cholesterol. The pathophysiology of dyslipidemia in SLE involves a complex combination of cytokines, autoantibodies, disease activity, medications, diet, and physical activity level, as well as other possible factors. The clinical implications of these findings indicate that if lipoprotein levels are abnormal, first-line therapy should involve diet and exercise interventions, usually for a minimum of 6 months. For persistent dyslipidemia, several pharmacologic therapies are available such as hydroxychloroquine, which improves lipid profiles and should be considered for all patients with SLE.
Our study showed no significant correlation between SLEDAI and serum TNFα levels, in contrast to studies by Sabry et al who found significant correlations between TNFα and interleukin-6 serum levels and the SLEDAI score.6,8 This may be due to the low number of SLE patients with an SLEDAI of more than 10 in our study (only 10 out of the 30 SLE patients), while in the studies by Sabry et al there were 20 patients (of a total of 40) with SLEDAI scores greater than 10.
Conclusion
The high levels of TNFα in SLE patients indicate the activation of an immune response. The increased common carotid artery intima-media thickness seen in lupus patients in this study was not correlated with TNFα levels and the presence or absence of dyslipidemia, denoting an underlying combining factor for early atherosclerosis in lupus patients other than those. Increased CIMT was seen in lupus nephritis patients, which may denote a role for inflammation in early atherosclerosis.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.