
Abstract
Atherosclerosis has been identified as the leading cause of mortality in developed countries, especially in Asia 1 and the Western world. 2 A study has shown that more than 2200 Americans die of cardiovascular disease every day, 3 and according to the European health report, it is projected that by 2015, one in three deaths would be attributed to this malady. 4 Cardiovascular-related diseases in Africa has been on a steady increase and is projected to be the leading cause of death in very short order. 5 Early detection of atherosclerotic manifestations in the vascular system is of fundamental clinical interest since this improves the chances of clinical management of the disease. 6 Some of these manifestations include increased intima-media thickness7,8 and alterations in hemodynamic patterns. 9 Even though intima-media thickening correlates with atherosclerosis 10 and is considered a surrogate marker as well as an independent risk factor, 8 anthropological variations, such as obesity, are a significant confounding variable. 11 A combination of other biomarkers such as the common carotid artery diameter in obese subjects 12 and some lipid profile parameters 13 with carotid intima-media thickness (CIMT) may improve sonographic predictability of atherosclerosis. Jarauta et al. 14 and Kozakova et al. 15 found that the CIMT in a population with no cardiovascular risk factors correlated with systolic blood pressure and low-density lipoprotein. This conclusion appears to reinforce the role of these biomarkers in subclinical atherosclerosis diagnosis alongside CIMT, but their findings may be population specific. This study is aimed at establishing whether this finding is applicable to another population of study by comparing lipid profiles and anthropological variables with CIMT values.
Methods
This prospective cross-sectional study was carried out between November 2015 and August 2016. It involved 215 apparently healthy subjects between 18 and 50 years. Ethical clearance was obtained from an appropriate hospital management board (BMSH/ADM/577/VOL.70/25), and both oral and signed informed consent were obtained from each subject. All prospective participants were screened using known biomarkers that predispose to atherosclerosis. They were examined by a cardiologist and had no history of hypertension. Their systolic and diastolic blood pressure values were less than 140 mmHg and 90 mmHg, respectively, while lipid profiles were as follows: fasting blood glucose level <126 mg/dL, total plasma cholesterol <220 mg/dL, low-density lipoprotein <160 mg/L, high-density lipoprotein >40 mg/L, and triglycerides <200 mg/L. Excluded from the study were gravid subjects, smokers, and those with a body mass index (BMI) ≥30 kg/m2. The BMI was measured using a MedTrue stadiometer (Nanjing, China), while lipid profiles were obtained using a Cobas C-111 autoanalyzer (Roche Diagnostics GmbH, Mannheim, Germany). All scans to measure the CIMT were carried out using Siemens 3-D/4-D X-class ultrasound equipment with a 7.5-MHz linear-array transducer (Siemens, Tokyo, Japan). Each patient, upon arrival at the sonography suite, rested for at least 10 minutes before the scan started. Blood pressure was taken using a sphygmomanometer by a certified and experienced nurse, and the procedure was once again explained to them. The patient then lay down on the examination couch, with the head and neck at the same level as the rest of the body. The patient was asked to rotate the neck to the contralateral side, and using a linear probe with a variable frequency (5–12 MHz), a general assessment of both carotid arteries was performed for the possible presence of atheromatous plaques. The long-axis view of the carotid artery was obtained, and the image plane was taken to pass through the diameter of the vessel when the intima reflection was observed along the entire length of the vessel visible on the screen (Figure 1). The common carotid artery was traced up to its bifurcation to display the bifurcation view consisting of the bulb and internal and external carotid artery in a single image (Figure 2). In some cases in which this was not possible, the probe was angled and/or rotated and the patient’s position adjusted to obtain the bifurcation view. In a few cases in which obtaining the image failed, measurements of the internal and external carotids were taken individually. For each vessel, measurement of the intima thickness was taken at the far wall at 2 cm from its origin, as illustrated in Figure 3. Two vascular sonographers with more than 10 years of clinical experience and who were blinded to each other’s findings performed manual measurements. Each sonographer took three measurements, and the average of the three was taken as the final measurement.
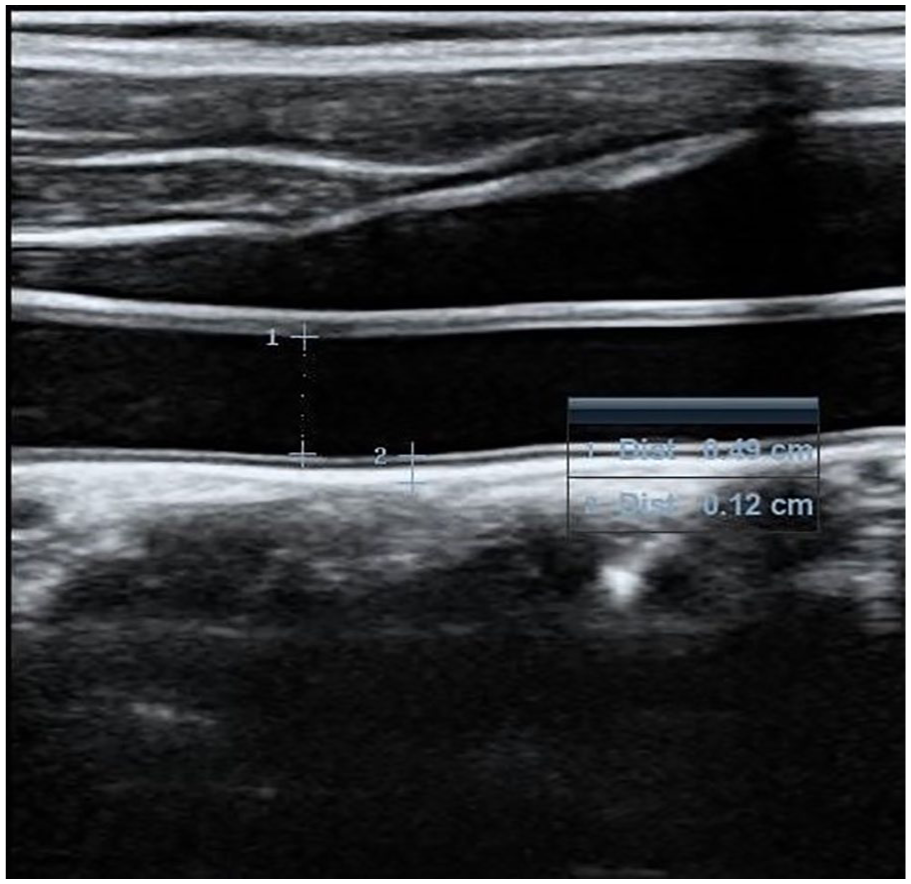
Measurement of the intima-media thickness for the common carotid artery.
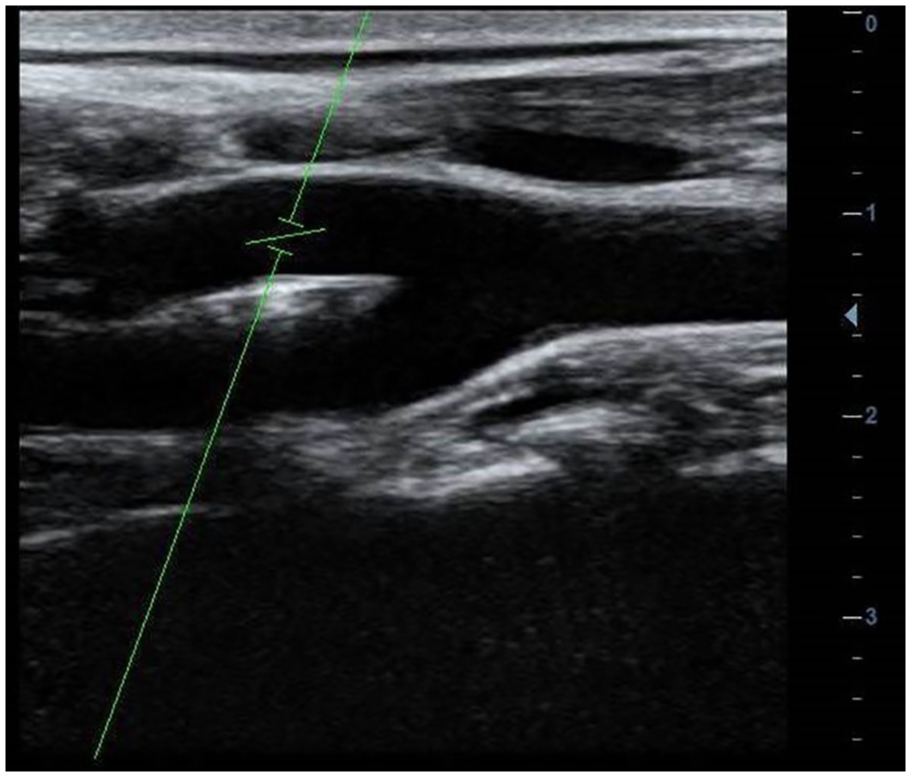
Bifurcation view for the carotid artery.
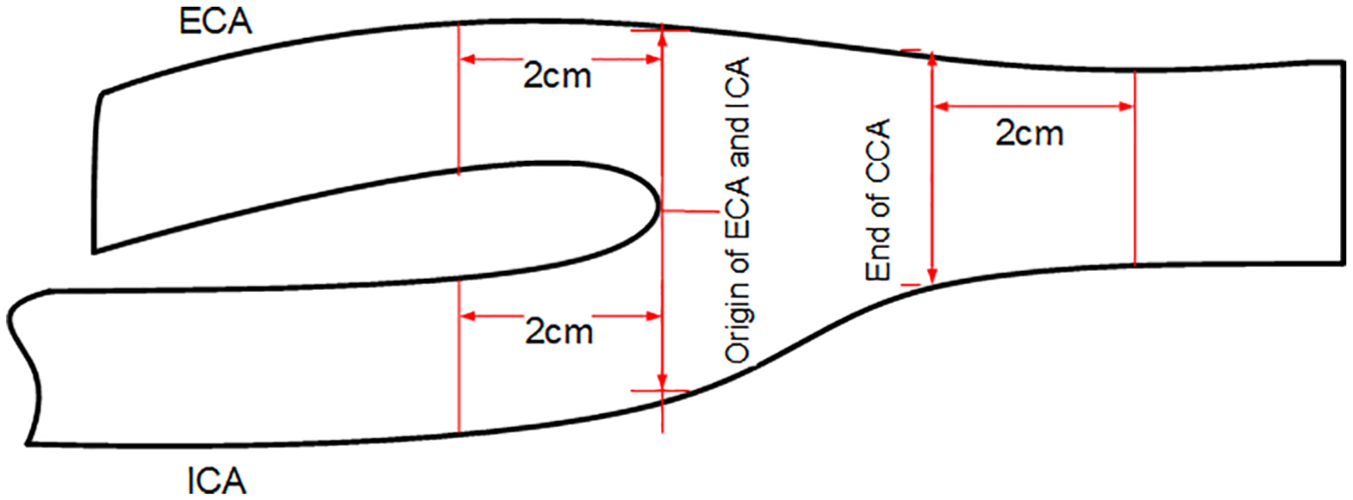
Illustration of the point at which carotid intima-media thickness measurements were taken at the various segments of the carotid artery.
Statistical Analysis
Data were analyzed using SPSS v.24 and R for Windows v.3.9. The strength of the association between CIMT on all segments and biometric parameters was assessed using η2 values. The reference range of CIMT was obtained using polynomial regression, and multivariate linear regression was used to determine the variables that were predictive of CIMT.
Results
Thirty-four of the recruited subjects did not complete the study, as they had visible plaque deposits on at least one of the carotid artery walls. Of the remaining 181 subjects, 87% were younger than 45 years and 58% (n = 106) were women. Other demographics of the study population are shown in Table 1. When controlling for the effect of gender, associations between CIMT and lipid profiles across all segments of the carotid artery were significant but moderate η2 = 0.09–0.24, except for triglycerides and high-density lipoprotein (η2 < 0.04). Conversely, the strength of association was higher for triglyceride–low-density lipoprotein and low-density lipoprotein–high-density lipoprotein ratio. A similar trend was observed for the left mean CIMT and in individual carotid segments measured. Age and BMI had the strongest association with CIMT across all segments (η2 > 0.7). Apart from the internal carotid artery, age, when compared with BMI, had a stronger association and correlation (Table 2). A stepwise multiple linear regression analysis demonstrated that age was the only significant predictor of CIMT (adjusted R2 = 0.79 and 0.78 for the right and left carotids, respectively). None of the lipid profile parameters had a significant effect on the regression model. Even though some biometric parameters such as BMI were positively correlated with CIMT, they were not statistically significant (P < .05).
Summary of Measurements in Male and Female Subjects.
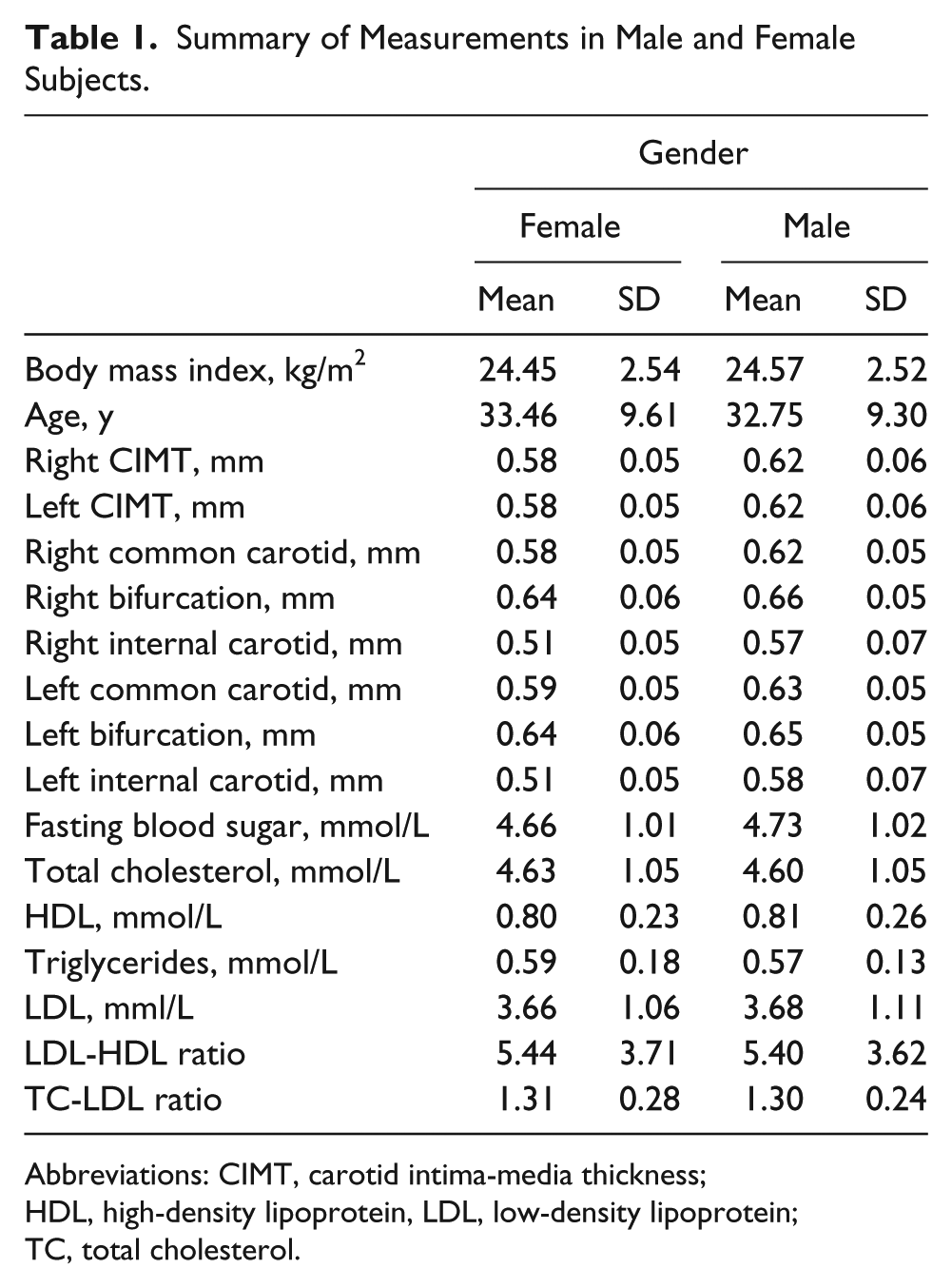
Abbreviations: CIMT, carotid intima-media thickness; HDL, high-density lipoprotein, LDL, low-density lipoprotein; TC, total cholesterol.
Correlation Between Left and Right CIMT With Age and Body Mass Index, Controlling for the Effects of Gender. a
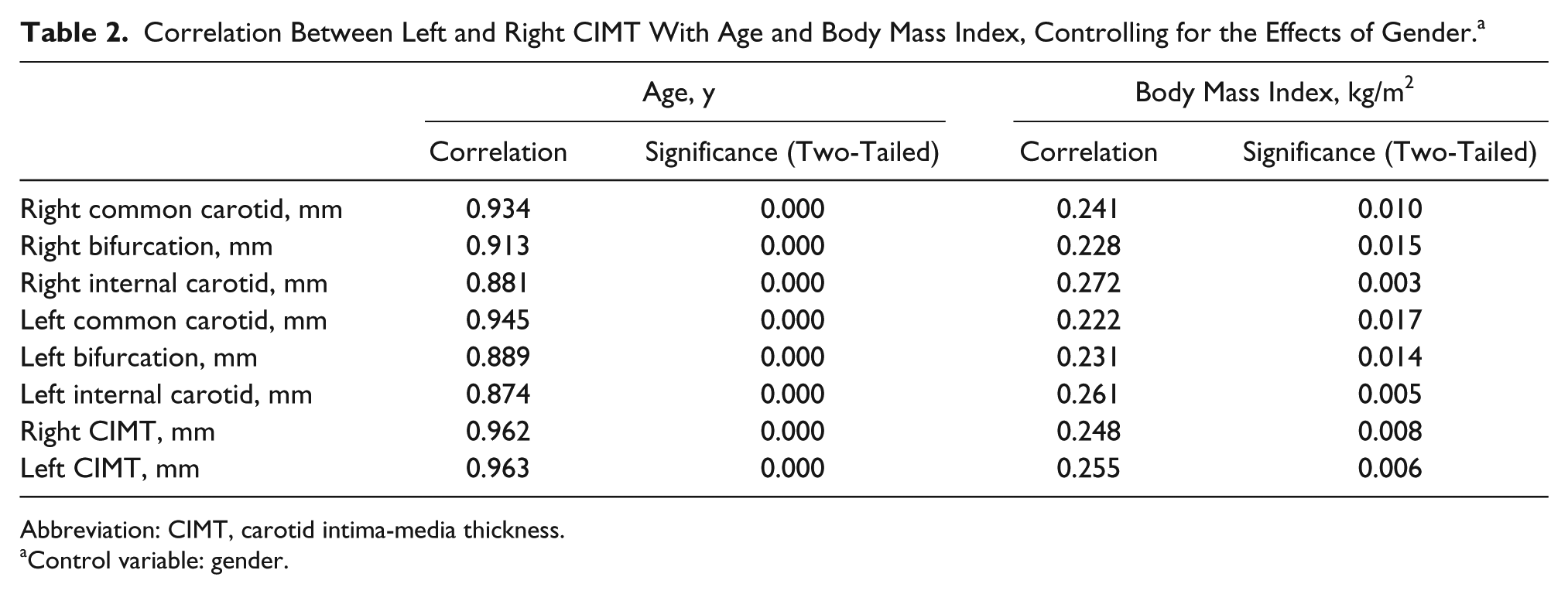
Abbreviation: CIMT, carotid intima-media thickness.
Control variable: gender.
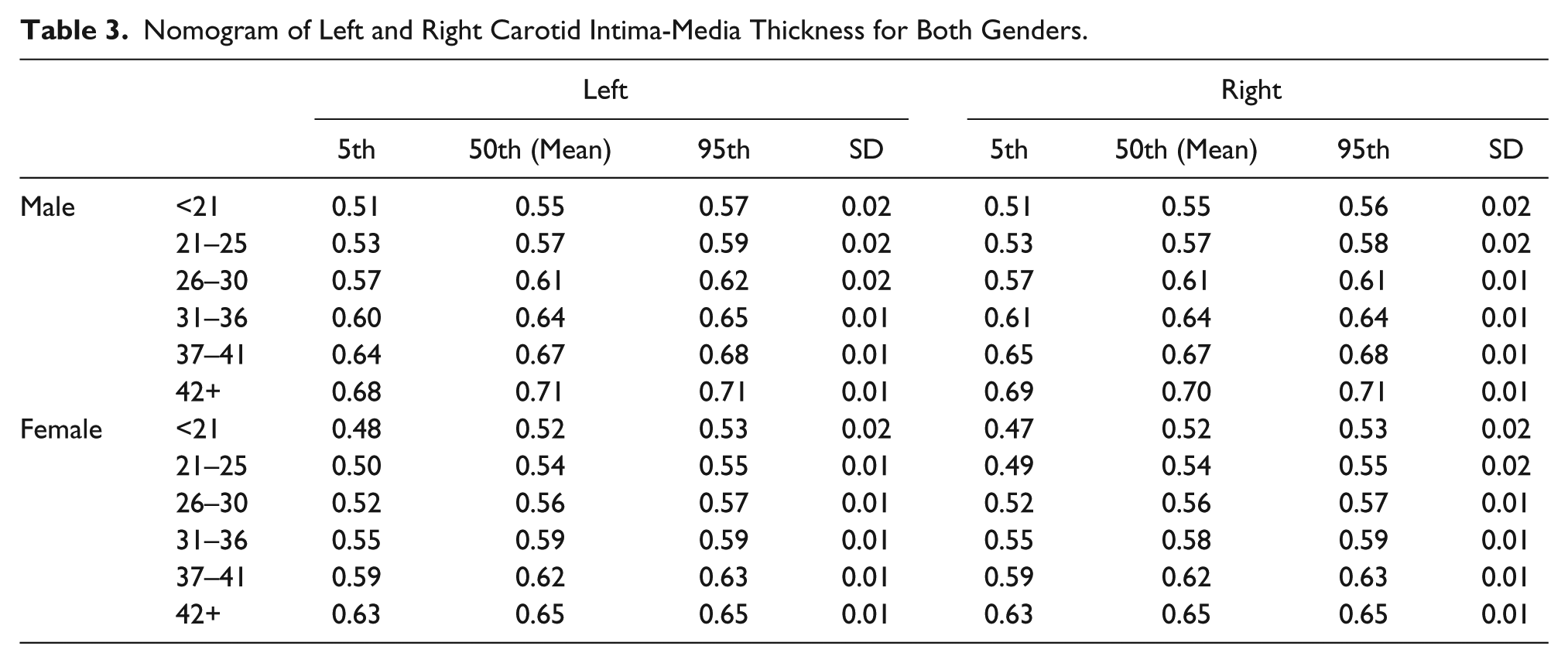
For the nomogram, a linear model (R2 = 0.93 for both gender) satisfactorily fitted the data for both the right CIMT and left CIMT, resulting in the following mathematical relationship between age and the right and left CIMT, respectively: men:
Nomogram of Left and Right Carotid Intima-Media Thickness for Both Genders.
Discussion
The insidious nature of atherosclerosis requires that early clinical diagnosis and intervention be sought, and a visible early sonographic feature is an alteration in the measured thickness of the intima of large arteries.16–18 The carotid artery has the highest predilection for deposition of atheromatous plaques. 1 Other arteries with plaque could include the abdominal, coronary, renal, and iliac arteries. 19 Ever since a direct relationship between CIMT and risk of cardiovascular events was reported in 1986, the number of studies on CIMT has increased considerably, reporting strong relationships between CIMT and atherosclerosis. CIMT is now considered as the biomarker most associated with cardiovascular events, even when compared with other traditional biomarkers combined. 20 Sonographic diagnosis of subclinical atherosclerosis relies on CIMT measurements, which could be improved when other biometric parameters are considered alongside it. Two different works14,15 have already identified low-density lipoprotein levels and systolic blood pressure as possible parameters, especially at higher levels. Hence, patients with increased CIMT who also have increased systolic blood pressure and low-density lipoprotein levels are more likely to present with atherosclerosis than patients with increased CIMT alone. In agreement with previous reports, 21 this study identified age as the strongest predictor of CIMT across all age groups. Stepwise addition of other predictors did not significantly improve the R2 value of the linear model. Even though BMI positively and significantly correlated with CIMT, the clinical significance of this is doubtful, as a stepwise inclusion of BMI in the linear model had a negligible effect on the R2 value of the final model. Other studies have reported that BMI plays a significant role in CIMT measurements,12,22 but the present study does not support this.
Several authors have published reference ranges,23–28 and findings on the difference between CIMT measurements in males and females are similar. An exception is the study by Umeh et al., 27 whose CIMT measurements in the female population were higher than that of the male population. Since the authors did not refer to the composition of the BMI of the population, it is possible that a large proportion of the female subjects recruited for the study had higher BMI than their male counterparts. In addition, the recorded BMI has previously been reported to affect CIMT. 11
The strength of this study lies in the fact that all subjects were carefully screened for the presence of clinical and sonographic features of atherosclerotic changes that could have affected the normal range values. Similar studies in this locality provided nomograms of CIMT but combined male and female data. This type of data set reduced the robustness of the nomogram that was created. The present work provides a separate nomogram for both genders, which is a better representation of CIMT values. A weakness in the present study was a lack of control for early subclinical atherosclerotic changes involving carotid wall thickening. This would include the inability of sonography to detect alterations in wall shear stress and carotid artery remodeling, which are common features in early atherosclerotic changes. 29 These parameters may have skewed the nomogram that is present in this study. Further studies that involve measurement of wall shear stress should be carried out to further elucidate the role that routine vascular sonography could play in the management of subclinical atherosclerotic changes.
Conclusion
This study presents a nomogram of the CIMT in a specific population of adults. It is hypothesized that clinical biomarkers of atherosclerosis, such as lipid profiles and BMI, may not improve the predictive value of CIMT in the sonographic detection of atherosclerosis.
Footnotes
Acknowledgements
We wish to thank Mr. Eke Christian and Mrs. Chinyere for their assistance in lipid profile laboratory sample analysis.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.