
Abstract
Objective:
Growing evidence indicates that depressive disorders (DDs) are an important risk factor for atherosclerosis. The aim of this study was to evaluate the presence of common carotid artery (CCA) intima-media thickness (IMT) and circulation inflammation markers in patients with DD.
Methods:
A cross-sectional prospective study was undertaken comparing 40 patients with DD to 40 individuals free of depression, matched for age and gender. The Beck Depression Inventory questionnaire, serum total cholesterol, triglycerides, high-sensitivity C-reactive protein, interleukin-6, tumor necrosis factor α, P-selectin, and E-selectin levels were measured. The CCA-IMT was assessed with duplex sonography.
Results:
Patients with DD were more likely to smoke (65% vs 40%; P = .03) and have higher levels of serum total cholesterol (211 mg/dL vs 181 mg/dL; P = .010), triglycerides (138 mg/dL vs 97 mg/dL; P = .005), and P-selectin (0.87 ng/mL vs 0.61 ng/mL; P = .05) and lower levels of interleukin 6 (4.4 ± 2.1 pg/mL vs 10.3 ± 1.1 pg/mL; P = .002). The CCA-IMT was similar in both groups (0.07 ± 0.02 cm vs 0.06 ± 0.01 cm; P = .31). Among those with CCA-IMT in the upper quartile, subjects in the DD group had lower levels of interleukin 6 (P = .05) and triglycerides (P = .01) and higher levels of soluble P-selectin (P = .03).
Conclusion:
Patients with DD do not present with higher CCA-IMT than a control group, although smoking and a higher level of serum lipids are present. Inflammatory biomarkers seem to be higher in patients with DD.
Cardiovascular disease (CVD) and depressive disorders (DDs) are currently the two most common causes of disability in developed countries. 1 Their relationship has been widely established and seems to be bidirectional. A recent study showed that nearly two-thirds of adults aged 50 years and older who met the diagnostic criteria for DD also had a diagnosis of heart disease, stroke, hypertension, and/or diabetes. 2 The American Heart Association recently suggested that major DD and bipolar disorder predispose even young individuals to accelerated atherosclerosis and early CVD. 3 Conversely, depression is a frequent complication of CVD; thus, a higher percentage of patients present with clinically evident atherosclerosis and DD. 1 A significant percentage of patients who have had a stroke experience depression afterward, while heart failure has been associated with a greater risk of depressive symptoms.4,5 The pathogenesis of this interaction is believed to be based on inflammation, endothelial dysfunction, increased platelet activity, and neurohormonal and autonomic nervous dysfunction.1,6,7
A body of research has emerged that tests the hypothesis that depressive symptoms increase the risk of CVD, as revealed by markers of subclinical atherosclerosis. Study protocols, strategies of measurement, and cutoff levels for both subclinical atherosclerosis and mental symptom assessments vary widely.1,8 Most studies were inconclusive and had high heterogeneity, providing mixed results.1,8–10 The common carotid artery (CCA) intima-media thickness (IMT) has been widely used as a marker of subclinical atherosclerosis.11–14 Despite differences between CCA-IMT protocols and population features among the studies, >60% of the CCA-IMT variance is consistently not explained by traditional cardiovascular risk factors, especially when CCA-IMT is measured in plaque-free locations.15–18 However, the prognostic role of IMT in atherosclerosis has been in doubt in recent years, and the prognostic role of carotid plaque has been highlighted. Recently, a meta-analysis showed that the sonographic assessment of carotid plaque, compared with that of carotid IMT, had a higher diagnostic accuracy for the prediction of future coronary artery disease events. 19 Another clinical study, the BioImage study (A Clinical Study of Burden of Atherosclerotic Disease in an At-Risk Population; NCT00738725), 20 has shown that carotid plaque burden is the strongest cross-sectional predictor of coronary artery calcium score, and its clinical utility as a predictor of future cardiovascular events is important. Meta-analyses conducted to examine whether carotid IMT is an independent predictor of future CVD events have reported inconsistent results.21,22
Growing evidence indicates that depression is an important risk factor for coronary heart disease. A recent study highlighted that patients with recurrent DD, even at the age of 30, exhibit early signs of carotid intimal and media changes, indicating a less healthy arterial wall, despite clinical signs of CVD. 23 In the Brazilian Longitudinal Study of Adult Health (ELSA-Brazil) cohort baseline, individuals with more symptoms of anxiety and/or depression had higher CCA-IMT values compared with peers of the same age, sex, and race. 8 These results suggest an association between anxiety/depressive symptoms and accelerated subclinical atherosclerosis. Additionally, serum markers of inflammation have been evaluated in order to assist in the identification of patients at risk of an asymptomatic carotid artery stenosis. C-reactive protein (CRP) is commonly used for cardiovascular risk evaluation, and other markers, such as fibrinogen, sVCAM, and erythrocyte sedimentation rate (ESR), have been shown to have some association with carotid atherosclerosis. 24 Interleukin 6 (IL-6), high-sensitivity CRP (hs-CRP), soluble P-selectin and E-selectin, sVICAM1, and MMP-3 and MMP-9 have also been evaluated with carotid disease. 24 Plasma low-density lipoprotein (LDL) cholesterol level is considered one of the most important risk factors for atherosclerotic plaque instability. 25
The aim of the present study was to evaluate the prevalence of CCA-IMT and the role of circulation inflammation markers in patients with and without a diagnosis of DD.
Methods
Patient Selection: Inclusion and Exclusion Criteria
The prevalence of CCA-IMT and the role of circulation inflammation markers in patients with DD in comparison to mentally healthy individuals have not been previously described. A power analysis based on the first 20 patients of each group (patients and controls) was conducted with G-Power v3.1 software and used preliminary data to determine the estimated power to inform the final sample size. The results indicated that a sample size of 32 for each group would be adequate to achieve a power of 0.8, as suggested in the literature. 26 Therefore, it was decided to end the sampling after reaching 40 participants for each group. Thus, the present study included 80 patients: 40 consecutive patients (case group) recruited from the psychiatric outpatient clinic suffering from an active DD and 40 age- and sex-matched subjects (control group) with venous varicosities who were scheduled for surgery. This study involved the collection of existing data and diagnostic tests that were recorded in such a manner that subjects could not be identified, either directly or through identifiers linked to the subject. The study was approved by the institutional review board and patients signed informed consent.
Both groups were assessed for depressive symptoms by using the Beck Depression Inventory (BDI) questionnaire.27,28 The case group completed the questionnaire in the Psychiatry Department, whereas the control group did so 1 month after their varicose veins surgery. The BDI questionnaire consists of 21 multiple-choice questions and is a self-report inventory, widely used for measuring the severity of depression. Each answer is scored on a scale of 0 to 3. Higher total scores indicate more severe depressive symptoms. The standardized cutoffs used differ from those of the original BDI: 0 to 13, minimal depression; 14 to 19, mild depression; 20 to 28, moderate depression; and 29 to 63, severe depression. All patients with DD had a BDI questionnaire score >13 and were included in the DD group, while patients treated for varicose veins with a BDI questionnaire score <13 were in the control group; patients with varicose veins that were treated with any antidepressant drug were excluded from the study.
Patients in the control group were categorized according to the Clinical Etiologic Anatomic Pathologic (CEAP) classification categories into class 2 (with varicose veins) and class 3 (with edema). No patient with a higher CEAP category was included in the study (with pigmentation, lipodermatosclerosis, atrophie blanche, or healed or active ulceration; classes 4–6). Patients with a known medical history of peripheral arterial disease, diabetes mellitus (fasting plasma glucose ≥126 mg/dL or use of antidiabetic medication), coronary heart disease, or hypertension were excluded from the study due to potential calcification of the arterial wall. Patients with previous interventions on the carotid arteries, neck irradiation, and a diagnosis of carotid or peripheral arterial disease, were excluded. Smoking status was recorded.
Primary Outcomes
The potential difference between the two groups in terms of the CCA-IMT was the primary outcome. All patients underwent duplex sonography of the carotid artery by the same operator. The CCA-IMT was measured 1 cm proximal to the carotid bifurcation (with the mean value of three measurements used) after imaging with a 12-MHz linear-array transducer (Logiq e; GE Healthcare), as shown in Figure 1. All individuals were placed in the supine position on an examination bed with their head in slight extension and medially rotated. The presence of any atheromatous plaque confirmed on the CCA-IMT, focally increased 0.14 mm,13,29 was recorded.
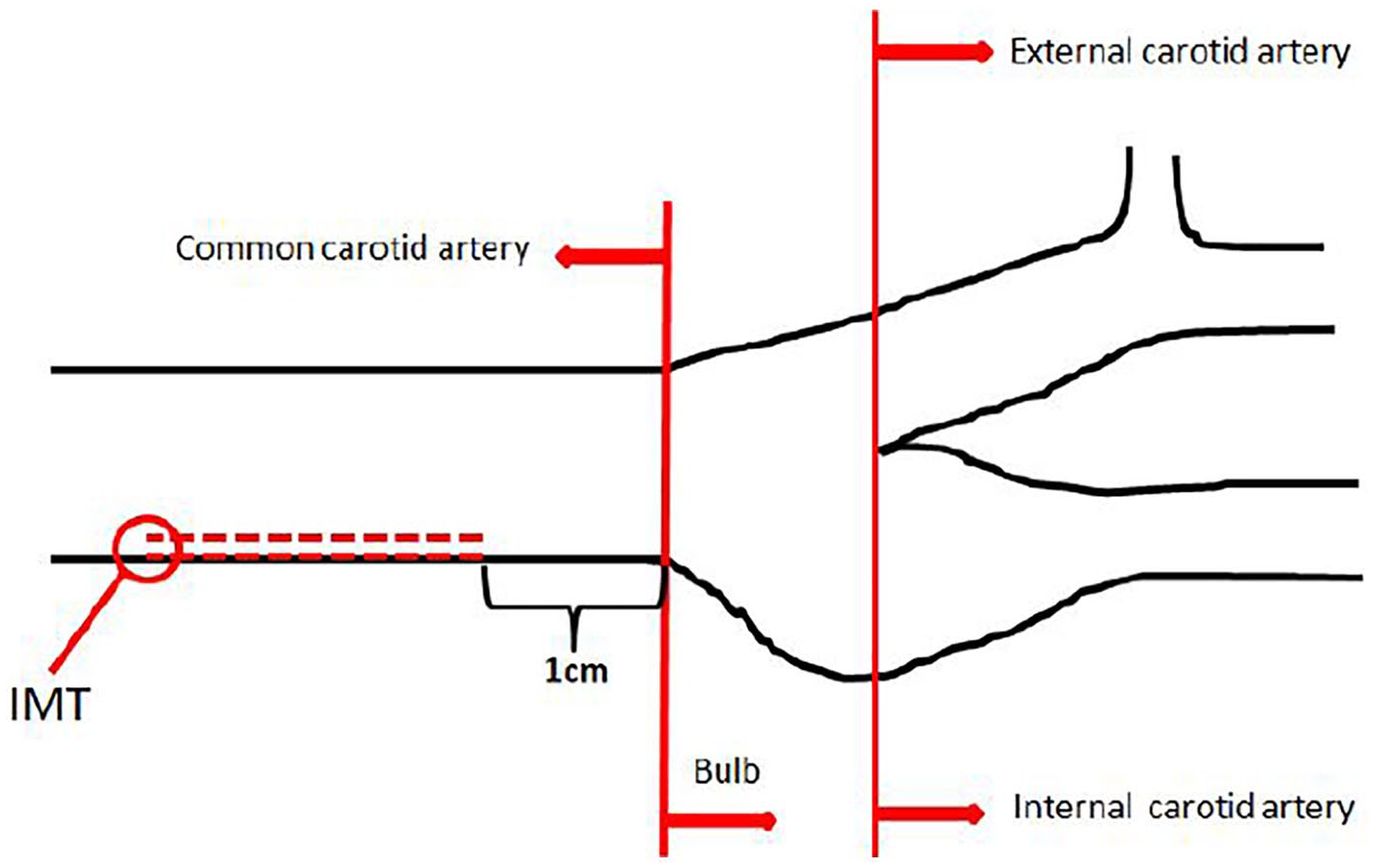
All patients underwent duplex ultrasound of the carotid artery by the same operator, and the common carotid artery intima-media thickness was measured 1 cm proximal to the carotid bifurcation (with the mean value of three measurements used) by a linear-array 12-MHz ultrasound transducer (Logiq e).
Secondary Outcomes
Secondary outcomes were defined as any potential differences between the two groups in terms of circulation inflammation markers. A fasting blood sample was collected from all patients (from the control group before surgery) in 10-mL vacutainer tubes (Becton & Dickinson) for the assessment of hematocrit, hemoglobin, fibrinogen, total cholesterol, high-density lipoprotein (HDL), LDL, triglycerides, creatinine, hs-CRP, IL-6, tumor necrosis factor α (TNF-a), sVCAM-1/CD106, sICAM-1/CD54, vascular endothelial growth factor, soluble P-selectin/CD26P, and soluble E-selectin/CD62E levels. The tubes were centrifuged at 3000 rpm for 10 minutes with the Hettich Rotofix 32A and frozen at −80°C until analysis.
Statistical Analysis
Data were expressed as mean ± standard deviation (SD) as appropriate, except for non-Gaussian parameters, which were presented as median (range). Comparisons of continuous variables were performed by the Student t test for normally distributed variables. The Mann-Whitney U test was used for nonnormally distributed variables, while the chi-square test was used for categorical variables. To assess the effect of the independent variables on the presence of DD within the study context, each one was initially examined separately and significant predictors at the P1 = .25 level were identified. These were then used in a Firth penalized likelihood logistic regression model. After testing for the effect of interactions at a P2 = .10 significance level, the factors eligible for entering the model at P3 < .05 were identified. General linear models were used to assess the statistically significant effects on all recorded factors and covariates on CCA-IMT. Significance was set at .05 and all analyses were carried out with the SPSS v20.0 statistical package for Windows (IBM Corp.).
Results
Demographics and patient characteristics are shown in Table 1. Smoking was more prevalent in the case group (65% vs 40%; P = .03).
Patient Demographics and Characteristics According to Different Study Groups. a
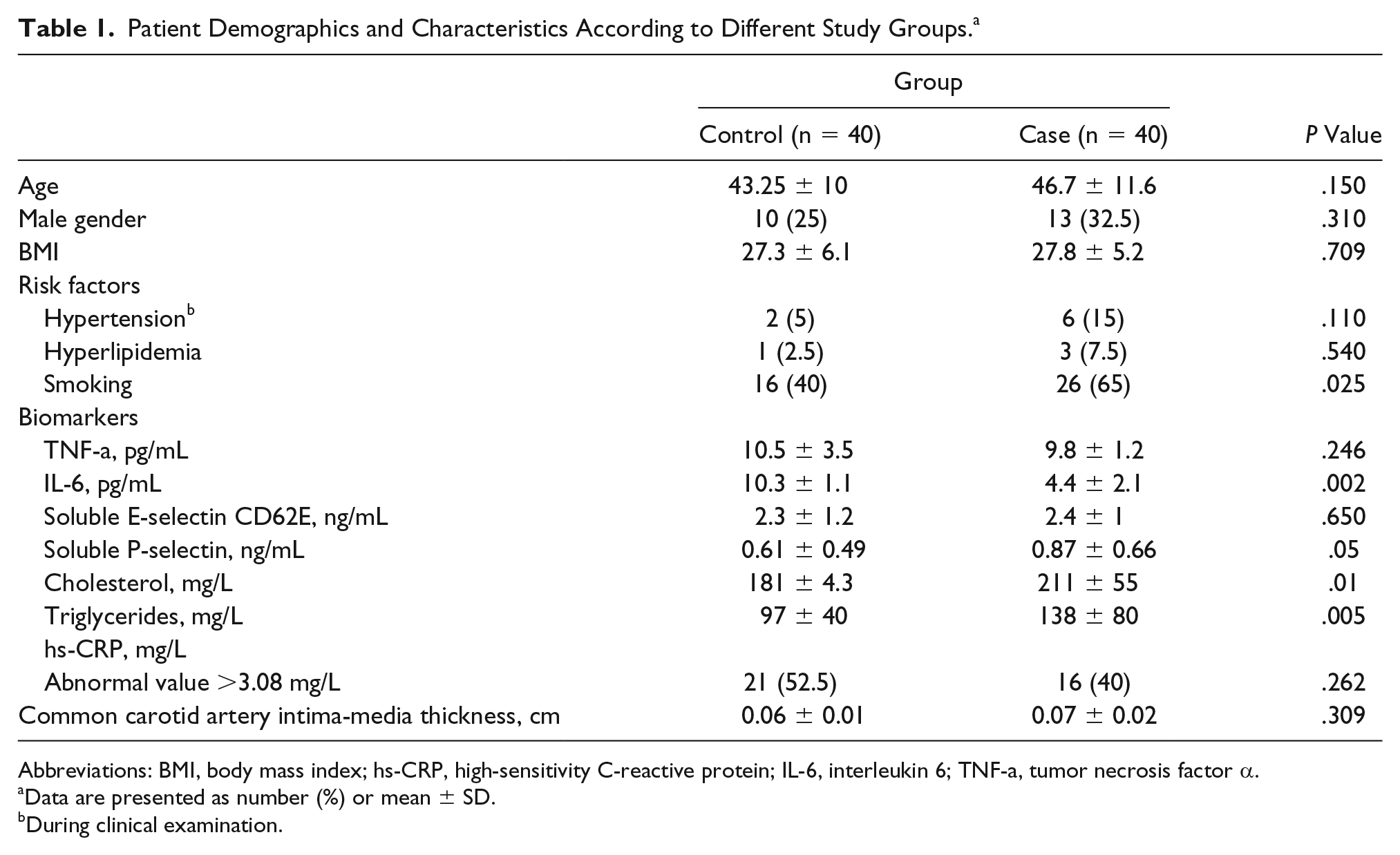
Abbreviations: BMI, body mass index; hs-CRP, high-sensitivity C-reactive protein; IL-6, interleukin 6; TNF-a, tumor necrosis factor α.
Data are presented as number (%) or mean ± SD.
During clinical examination.
Also, case group (patients with DD) had higher levels of total cholesterol (211 mg/dL vs 181 mg/dL; P = .01), triglycerides (138 mg/dL vs 97 mg/dL; P = .005), and P-selectin (0.87 ng/mL vs 0.61 ng/mL; P = .05), but lower levels of IL-6 (4.4 ± 2.1 pg/mL vs 10.3 ± 1.1 pg/mL; P = .002) when compared with the control group. No difference was found between the two groups with respect to all other inflammatory biomarkers (Figure 2).
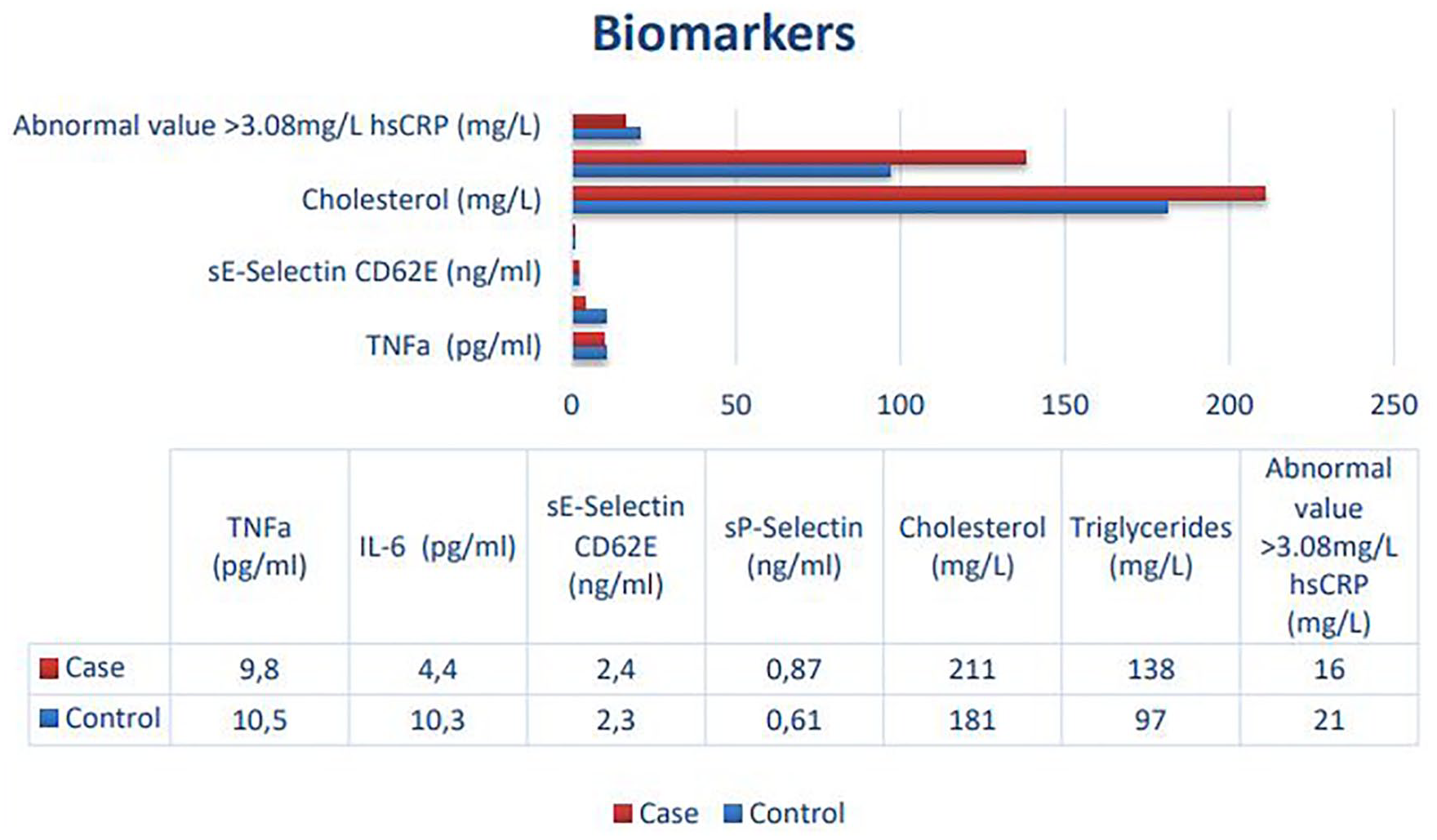
No difference was found between the case and control groups with respect to all other inflammatory biomarkers.
None of the individuals in the groups were diagnosed with an atheromatic plaque. The CCA-IMT was not different between the two groups (0.07 ± 0.02 cm vs 0.06 ± 0.01 cm; P = .31) (Figure 3). Among patients in the case group, those with CCA-IMT in the upper quartile had significantly lower levels of IL-6 (P = .05), triglycerides (P = .03), compared with those in the control group with CCA-IMT in the upper quartile (see Table 2). Only one patient in the DD group had carotid plaque and none in the control group.
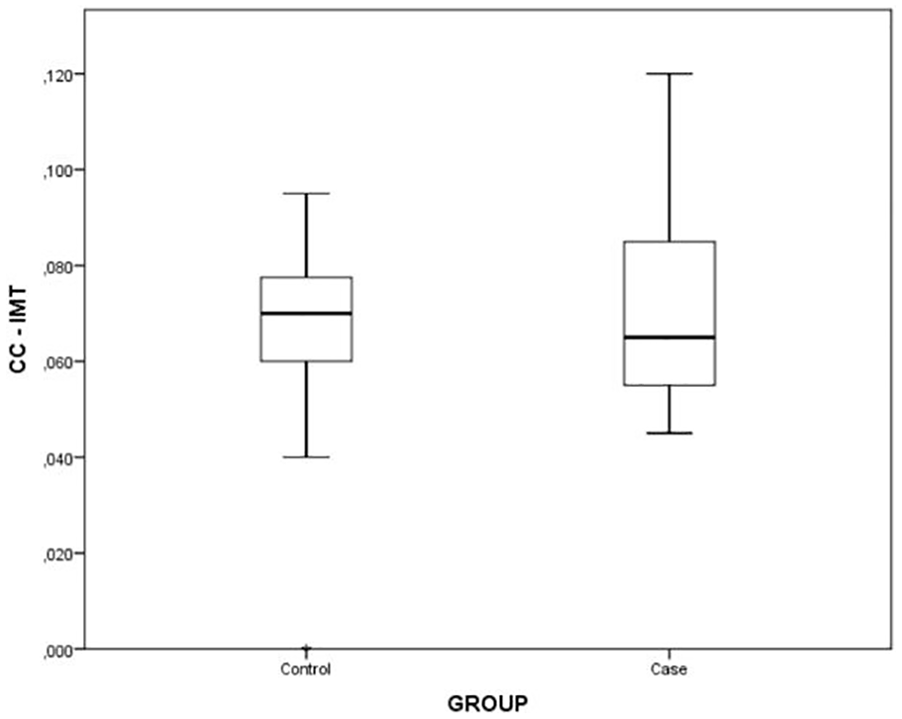
Distribution of common carotid artery intima-media thickness between the case and control groups.
Patients With Common Carotid Artery Intima-Media Thickness in the Upper Quartile. a
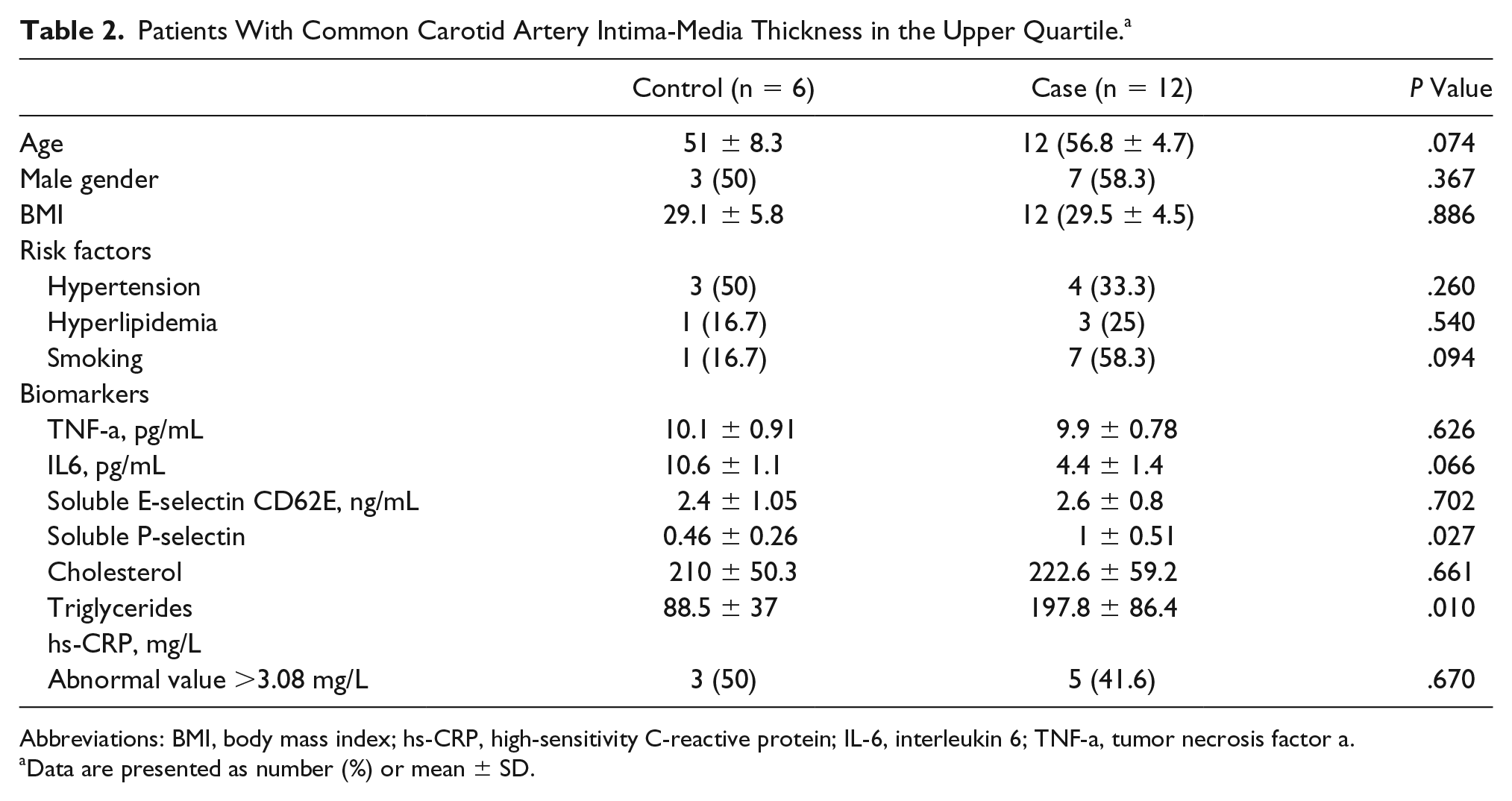
Abbreviations: BMI, body mass index; hs-CRP, high-sensitivity C-reactive protein; IL-6, interleukin 6; TNF-a, tumor necrosis factor a.
Data are presented as number (%) or mean ± SD.
A post hoc analysis based on 80 participants, 40 in each group, showed that the power reached was 0.877.
Discussion
The interaction between atherosclerotic CVD and DD has attracted some interest over the past decades. Some select publications agree that individuals with depression or DD are subject to higher cardiovascular risk.30–32 A higher burden of common atherosclerotic disease risk factors, alterations in platelet function, hypercoagulability, and disturbances in autonomic nervous system functions have all been proposed to explain the higher incidence of cardiovascular events in individuals with DD.30–32 The establishment of the association of DD and subclinical atherosclerosis is still debatable because of the substantial heterogeneity among the relevant studies. The prevalence of atherosclerotic factors and the related characteristics vary among different populations. A worldwide-validated assessment has not been widely accepted.
CCA-IMT has been recognized as a marker of atherosclerosis which can be predictive of future cardiovasular events and mortality.11–14,33,34 Despite differences between CCA-IMT protocols and population features among the studies, >60% of the CCA-IMT variance is consistently not explained by traditional cardiovascular risk factors, especially when CCA-IMT is measured in plaque-free locations.15–18 Thus, its diagnostic value may not be important among different populations. This work may represent the first study in Greece evaluating whether CCA-IMT could be a marker of early atherosclerosis in patients with DD. In this study, the CCA-IMT values of patients with DD were no different than those of individuals matched for age and gender without DD. This observation is in agreement with a previous study in which no association of DD and mean CCA-IMT was found among South American Hispanics. 35 Similar findings were found in another multiethnic study including 6500 subjects of four different ethnicities. 36 Nevertheless, in other reports8,37 contradictory findings were obtained showing that depressive symptoms were independently associated with an accelerated progression of CCA-IMT in subjects with cardiovascular risk factors. Apparently, these conflicting results may be attributed to different atherosclerotic patterns across race/ethnic groups and the heterogeneity in study designs and populations.
Despite the abundant initial evidence that an increased CCA-IMT was a marker of atherosclerosis to predict cardiovascular morbidity and mortality, its value has been questioned due to the atheromatous plaque and volume being noted as powerful predictors of future cardiovascular events.38–40
Besides CCA -IMT, there are other markers of subclinical atherosclerosis in patients with DD. Seldenrijk et al., 41 investigating a large cohort aged 18 to 65 years from the Netherlands, found that patients with depressive and anxiety disorders had a two- to threefold increased odds of abnormal ankle-brachial index (<0.9). Furthermore, coronary artery calcium progression, a valuable tool for subclinical atherosclerosis and CVD risk assessment, was independently associated with the presence of depressive symptoms in 346 midlife women. 42
Inflammation as a mechanism for the development of atherosclerosis and cardiovascular events is well known. 43 Previous research indicates that an association between inflammation and depression may exist in older adults, but the results are inconsistent. 44 Results indicated a cross-sectional and longitudinal association between both CRP and IL-6 and depression in older adults, with inflammation leading to depression in longitudinal studies rather than depression to inflammation. However, there was a notable heterogeneity among the studies as their results differed based on the adjustment for confounders and on how inflammation and depression were measured. These sources of heterogeneity could explain the differences in their results. 44 Additionally, the impact of inflammation on DD may be also present in younger ages; higher levels of the systemic inflammatory marker IL-6 in childhood are associated with an increased risk of developing depression and psychosis in young adulthood. 45 Inflammatory markers have been considered surrogate markers of atherosclerotic burden, potentially having a direct role in atherosclerotic plaque rupture and thrombosis.46,47 P-selectin has been related to the early stages of atherogenesis by recruiting leukocytes into developing atherosclerotic plaques. 48 In the present study, patients with DD compared with individuals without DD had higher P-selectin levels, no difference in TNF-a, but surprisingly lower IL-6 values. This is important in itself because a recent study revealed that patients with chronic venous insufficiency present with significantly lower levels of IL-6 and TNF-a, however in the present study, the levels of IL-6 were even lower in DD patients. 49 A recent meta-analysis found higher mean levels of IL-6 and no correlation with TNF-a levels in patients with major depression compared with controls without depression. 50 The small sample size in this study may account for these discrepancies, although adequate data regarding these inflammatory atherosclerosis biomarkers on a large Greek population with DD are missing.
In this study, no difference was observed between the two groups with respect to hyperlipidemia. Several studies have suggested an association between lipids or lipoproteins and depression, but the findings are contradictory. However, studies did not always take into consideration potentially mediating factors or the heterogeneity of symptoms, which may clarify contradictory findings. A recent study demonstrated that melancholic features were independently associated with lower HDL cholesterol, and atypical depression was independently associated with higher total and LDL cholesterol. 51 Elevated depressive symptoms were associated with a lipid profile characterized by high cholesterol, high triglycerides, low HDL cholesterol, high LDL cholesterol, and dyslipidemia; the associations were partially mediated by ischemic heart disease and stroke. These findings imply that an unfavorable lipid profile may be involved in late-life depressive symptoms independent of atherosclerotic disorders.52,53 However, statins may improve DD. Salagre et al., 54 in a meta-analysis of three randomized controlled trials, showed that statins, as an add-on treatment, largely improved depressive symptoms in 165 participants with moderate to severe DD. Additionally, aspirin has been found to decrease depression risk in older men with high plasma homocysteine. 55 These observations may imply that statins and aspirin improve DD in addition to their well-known preventive CVD effect. Nevertheless, larger prospective studies are needed to clarify the role of the best medical treatment in such a specific population.
Smoking was more prevalent in our DD group. This observation has also been demonstrated in other reports.56,57 Obviously, smoking cessation prevents CVD development in patients with DD too. Despite such differences in smoking between the case and control groups in our study, no particular effect in the CCA-IMT was found.
The present study is the first to look into the association of DD and atherosclerosis in a Greek population. Its findings should be interpreted cautiously, though, as there are several limitations. First, it was not possible to assess the presence of atheroma in the carotid bifurcation as a marker of early atherosclerosis in patients with DD. Also, it could be argued that the control group suffering from chronic venous insufficiency may have had an impact on the inflammation markers. However, a recent study showed that inflammation markers were higher in patients with severe chronic venous insufficiency compared with mild 58 ; therefore, in this study, only patients with CEAP classes 2 and 3 were included. Additionally, a recent systematic review of the literature showed that circulating estradiol, homocysteine, and vascular endothelial growth factor were the markers most consistently associated with primary chronic venous insufficiency. 59 Another limitation is that the control group answered only the BDI score without a clinical assessment from a psychiatrist. In the DD group, some patients were already on antidepressant therapy, and thus this may have influenced their laboratory biomarkers. Yet another limitation is the lack of data on statin administration, which would have been useful. None of the patients from the control group were on veno-active drugs. Additionally, the vast majority of patients in the DD group had mild to moderate DD, and this may have obscured differences with the control group.
Conclusion
In this study, patients with DD did not present with higher CCA-IMT than the control group, although they smoked more and had higher levels of serum lipids. In this cohort, inflammatory biomarkers seemed to be higher in patients with DD.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.