
Abstract
Objective
The objective was to identify sonographer perceptions of distractions and policies for improving obstetric sonography examinations (OBUS).
Materials and Methods
A survey, with closed- and open-ended questions, was sent to OBUS practicing members of the Society of Diagnostic Medical Sonography (SDMS). Descriptive analyses, including frequency distributions overall and by various groups, were performed. Chi-square analyses were used to examine the relationships between categorical variables, including level of perceived distraction, and concordance with policies.
Results
Of the 3525 accessed e-mails, 807 responses were eligible for analysis. Over half (62%) of the respondents reported no observer policy. Sonographers reported strong agreement with observer policies and desired limits on observers. Policy disagreement themes included number of observers, children observers, patient satisfaction, and patient truthfulness. Most sonographers reported existence of (85%) and strong agreement (97%) with recording policies. Disagreements centered around the strictness of policies, policy enforcement and notification, distraction of recording, medico-legal issues, and finding anomalies while being recorded.
Conclusion
Discrepancies existed between policies regarding observers and recording in OBUS. Sonographers both desired and agreed with protocols to limit distractions. However, there were concerns regarding stringency, notification, and enforcement of policies. Further research is needed to determine if policies help limit distractions during OBUS.
Key Takeaways
Observer and recording policies are not ubiquitous, but, when in place, are generally supported by sonographers.
There are no standard methods for notifying patients/families about policies, and there are some concerns about adherence to policy potentially related to notification method.
Sonographers who work at locations without policies to limit distractions desire such policies.
An obstetric sonography examination (OBUS) is both a medical examination and a social experience. OBUS is performed for a variety of medical indications, screening purposes, and in some instances, to reassure patients that things are as they should be. 1 In US culture, OBUS is considered an event attended not only by the patient and their partner but also by their children, their parents, and perhaps even their close friends. 2 OBUS is viewed as an opportunity for individuals, especially fathers, to bond with the fetus. 3 Often the sonographer is expected to answer questions and “show” the fetus to the patient, which is unique to the role of obstetric sonographers. 4
The experience of obstetric sonographers differs from that of practitioners of other imaging modalities. In other medical imaging modalities, such as magnetic resonance imaging (MRI), radiography, or computed tomography (CT), there are specific rules about observers and the use of recording devices. 5 Nonpatient observers are often explicitly prohibited, and technologists/radiographers themselves cannot be in the room with the patient while the imaging equipment is in use. Mobile phone use is also discouraged, if not prohibited, near most medical equipment in the hospital environment. Signage to this effect is posted in most imaging settings, despite the low risk of interference posed by mobile phones. 6 However, no such built-in restrictions exist for observers of OBUS, as the equipment does not pose a risk to operators or observers. In addition, OBUS may be performed in various locations, including clinics and free-standing imaging centers where policies and procedures may be more liberal than in the hospital setting. The safety of sonography coupled with the expectation that patients must share their experience with family and friends creates an issue of crowd control. Interruptions and distractions have become commonplace in the OBUS examination room, creating a loud, chaotic, and possibly disruptive work environment for sonographers.
Research has shown that interruptions and distractions contribute to medical errors.7–9 Rivera-Rodriguez et al, posed that “interruptions have implications for safe and high quality healthcare delivery” and suggest that “further research must go into more depth to understand interruptions in light of the complexity of healthcare.” 8 As distractions have been shown to lead to compromised quality and safety in other areas of health care, it follows that this is likely true in the setting of OBUS.
A recent review of the literature found a lack of publications on sonographer’s opinion regarding the effect of distractions on the accuracy and quality of OBUS, in the United States. However, a blog post on the American Institute of Ultrasound in Medicine (AIUM) website reported a survey assessing the presence of recording policies in OBUS. 10 While this was not a peer-reviewed publication, the AIUM survey does underscore an interest, within the obstetric community, to limit the distractions faced by US sonographers. An Australian study surveyed 393 Australian and New Zealand obstetric sonographers/sonologists regarding distractions in OBUS.11,12 The authors found that the sonographers surveyed believed that “distractors impact . . . the quality and safety of the obstetric ultrasound examination” but that further research was needed to determine which distractions would impede quality and safety. 11 In a second publication, the authors discussed the need for developing policies to minimize distractors. 12 The generalizability of these studies is limited by the sample size and practice location. As the structure of the health care system in the United States differs from the national health care system in Australia, sonographer work environments and work processes are likely also different. In addition, free-standing, for-profit locations that provide nonmedical OBUS for keepsake and gender reveal experiences may increase patient expectations of a social experience.1,13 The aims of this survey were to (1) identify sonographers’ perceptions of specific distractions, (2) determine whether policies limiting the distractions were present, (3) record whether sonographers agreed with these policies, and (4) explore whether these policies improved sonographers’ job satisfaction.
We hypothesized that distractions are routinely present in OBUS in the form of unruly children, noisy observers, obtrusive mobile phone use, and unauthorized photography and/or audiovisual recording. Sonographers who work in environments where policies are present to limit these distractions likely agreed with these policies and had improved job satisfaction.
Materials and Methods
The survey design was adapted from previously published work by Najafzadeh et al. 11 There were 78 questions which assessed sonographer demographics, impressions about distractions possibly present during examinations, presence of observer and/or recording policies, the degree of adherence to any policies, and perceived frequency of poor job performance. The survey was made up of both closed- and open-ended questions, as well as Likert scales to rate the perceived level of distraction and distractor effects on the frequency of poor job performance (see https://redcap.link/hct5dmxi). Prior to distribution, the survey was reviewed by a convenience sample of maternal-fetal medicine physicians and sonographers for clarity and content. Full completion of the survey was estimated to take approximately 5–10 minutes. Institutional review board (IRB) approval was obtained (20-0251). In addition, the survey was approved for distribution to select members of the Society of Diagnostic Medical Sonography (SDMS). A survey link was distributed to 9641 nonstudent members practicing OBUS on March 3, 2020. Responses were collected anonymously through REDCap. A reminder e-mail was sent approximately 2 weeks after the first e-mail. The survey was closed for responses 1 month after the initial e-mail.
Responses to the following survey questions were collected: basic demographic questions, respondents’ perceived occurrence of poor work performance when distractors were present, and respondents’ opinions on both observer and recording policies. Collected free-form comments were analyzed using standard qualitative data methods.14,15 Comments were line-by-line, open-coded by two authors to generate in vivo codes of concepts. The research team then confirmed that they agreed with the concepts and grouped them into thematic categories if two or more comments included the same concept. The analyses focused on overall frequency distributions and frequency distributions by various groups. Chi-square analyses were used to examine the relationships between sonographer demographics and agreement/disagreement with policies.
Results
Survey responses were collected from March 3, 2020 to April 3, 2020. Of the 9641 OBUS practicing SDMS members sent the survey by email, 3525 accessed the survey link. Of those who participated, only 807 responses were eligible for analysis (see Figure 1). Demographics of the survey respondents are summarized in Table 1. Most survey respondents were female (93%) with a median age of 49 years. About half of the respondents reported having dependents, with the median number of dependents being two and the median age of the youngest dependent being 12 years. The median of years of experience was 20 years with 74% of respondents having greater than 10 years of experience. The two most common education qualifications were an associate degree (43%) followed by a bachelor’s degree (35%). The majority (45%) of sonographers practiced in suburban settings and reported performing between 0 and 4 OBUS per day (44%).
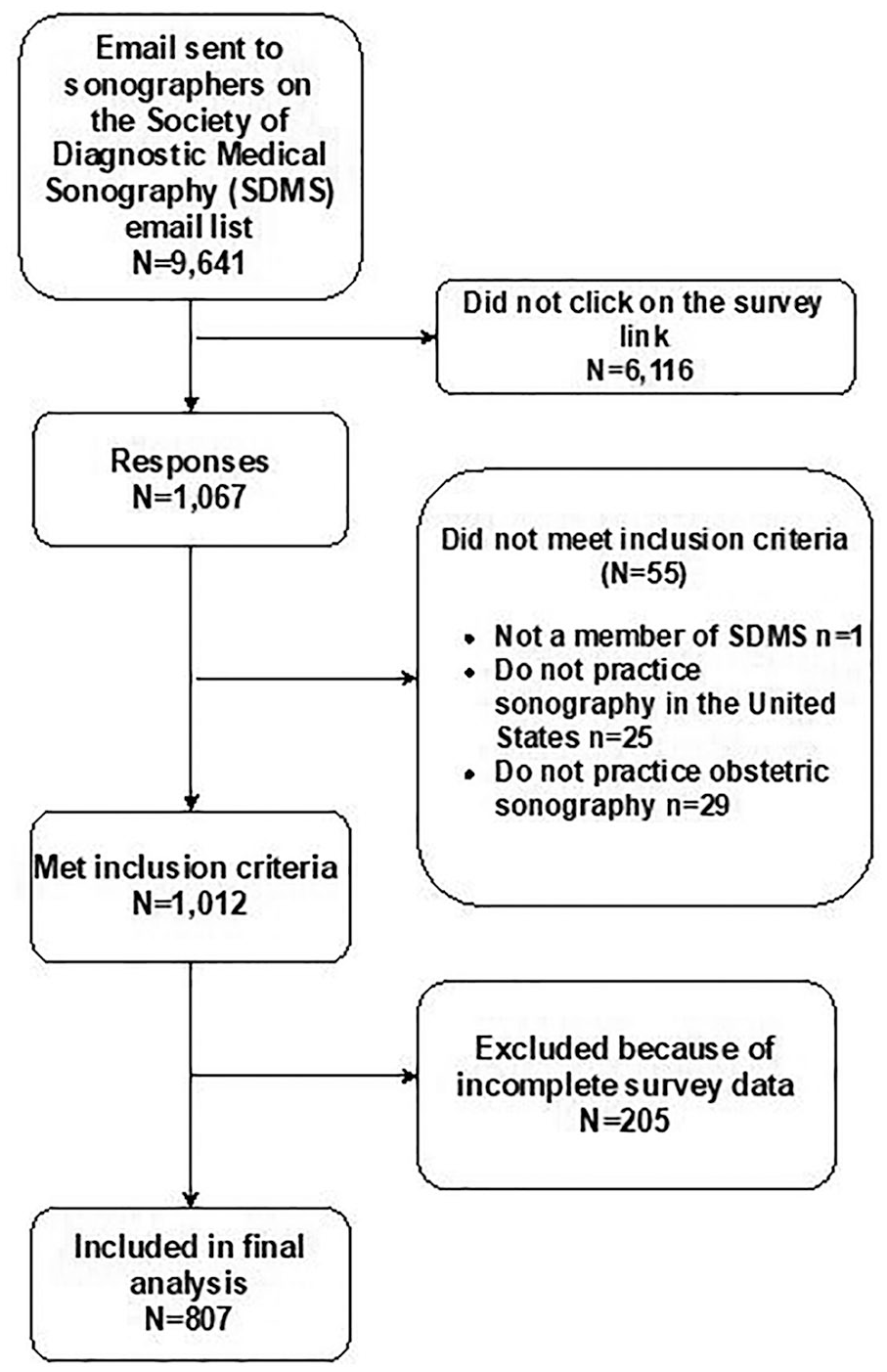
Survey respondents and exclusion criteria.
Participant Demographics (N = 807).
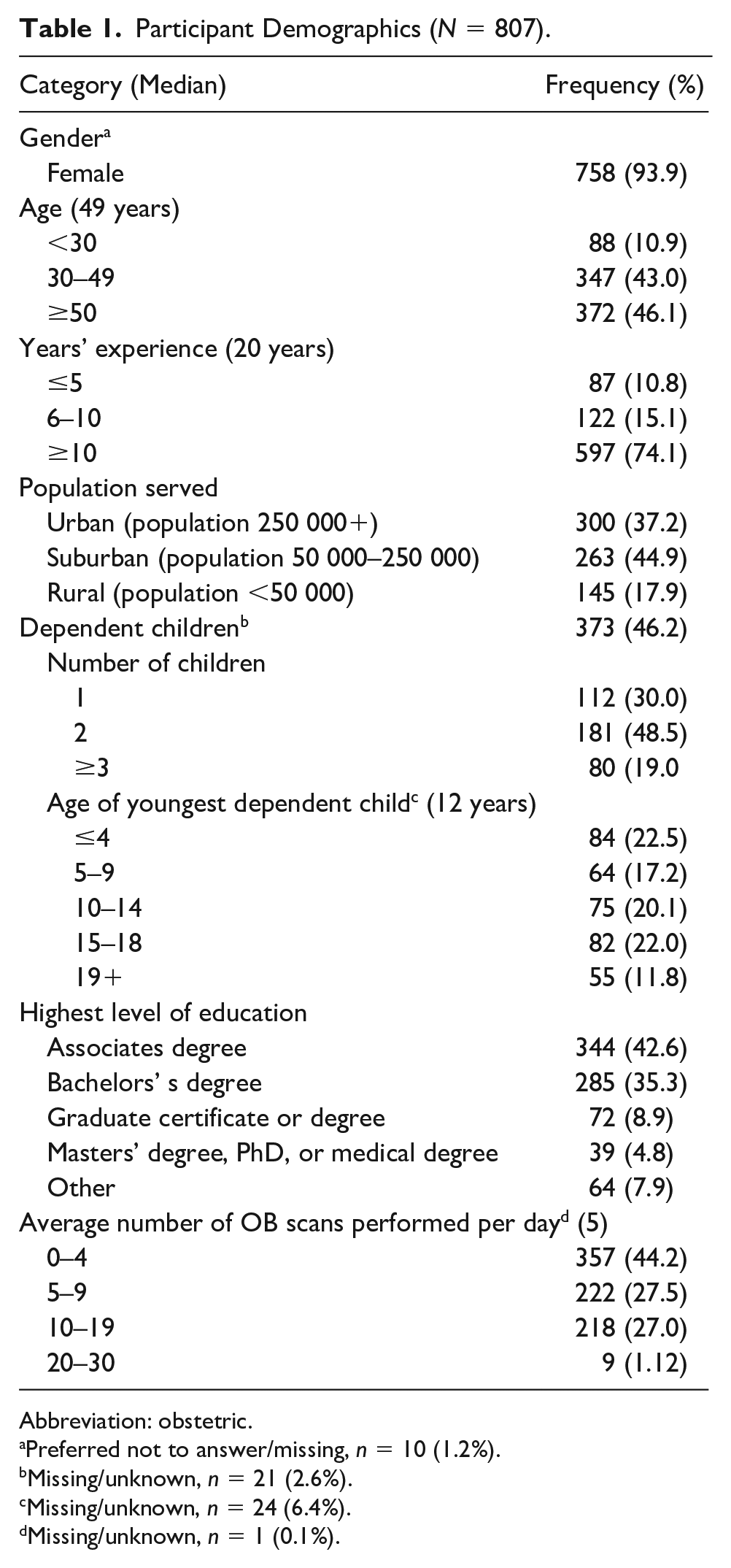
Abbreviation: obstetric.
Preferred not to answer/missing, n = 10 (1.2%).
Missing/unknown, n = 21 (2.6%).
Missing/unknown, n = 24 (6.4%).
Missing/unknown, n = 1 (0.1%).
Regarding Observer Policy
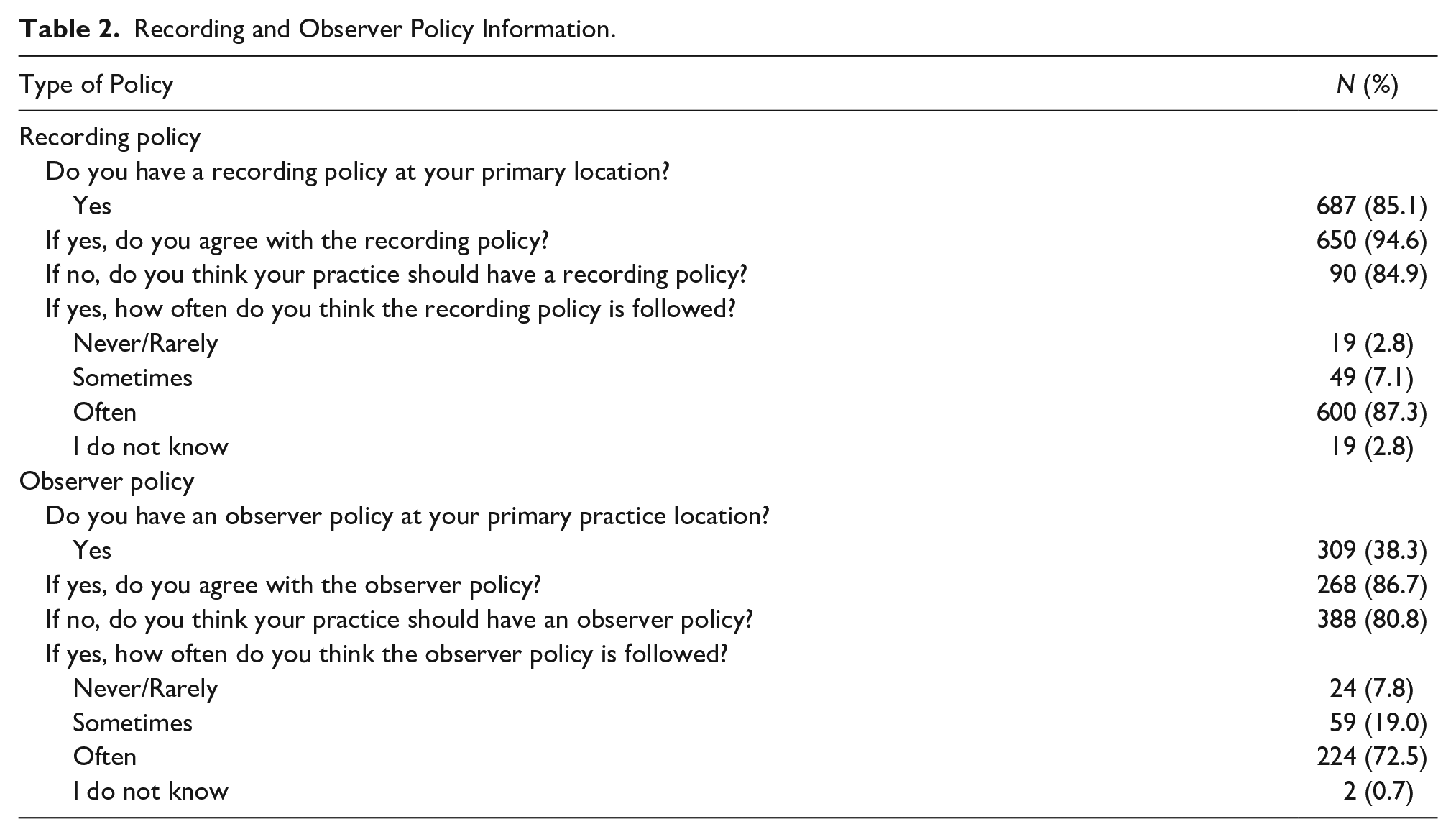
Only 38% of respondents reported there were standards in place in their department limiting the number and types of individuals allowed to accompany patients during an OBUS examination (Table 2). Respondents who reported an observer policy described varying degrees of patient adherence. Most respondents felt that patients often or always (73%) adhered to observer policies. Eight percent of respondents felt that observer policies were never or rarely followed. There were a variety of ways patients were informed of observer policies; 36% of respondents reported that patients were told at initial appointment scheduling, while 27% indicated it was the sonographer’s responsibility to inform patients at the start of the appointment.
Recording and Observer Policy Information.
Among respondents with an observer policy in place at their practice, 90% reported strong agreement with the policy. There were no statistically significant associations between agreement with practice observer policies and sonographer demographics. Sonographers who disagreed with the observer policy at their practice (10%) were given the opportunity to write free-form comments about why they disagreed with their practice’s observer policy, to which all respondents added commentary. Of those who disagreed with the observer policy at their institution, the majority (85%) believed the policy in place was not strict enough. Themes were noted around the number of observers, the presence of children, prioritizing patient satisfaction over the medical aspects of the examination, concerns about how the policy is handled, and patient truthfulness (Table 3). Those who believed the policy was too strict (15%) voiced concerns about how important the ultrasound is in making “the pregnancy becomes ‘real’ for siblings and dads” and how it “unites the family.” More than half of the respondents (60%) reported that there was not an observer policy in place at their practice. Of the respondents who reported no observer policy, 81% desired one. Among those who did not think their practice should have an observer policy, most (61%) were over 50 years old (P = .0054). No other demographic variables were found to have statistically significant associations with not desiring an observer policy.
Themes Regarding Disagreement With Observer Policy.
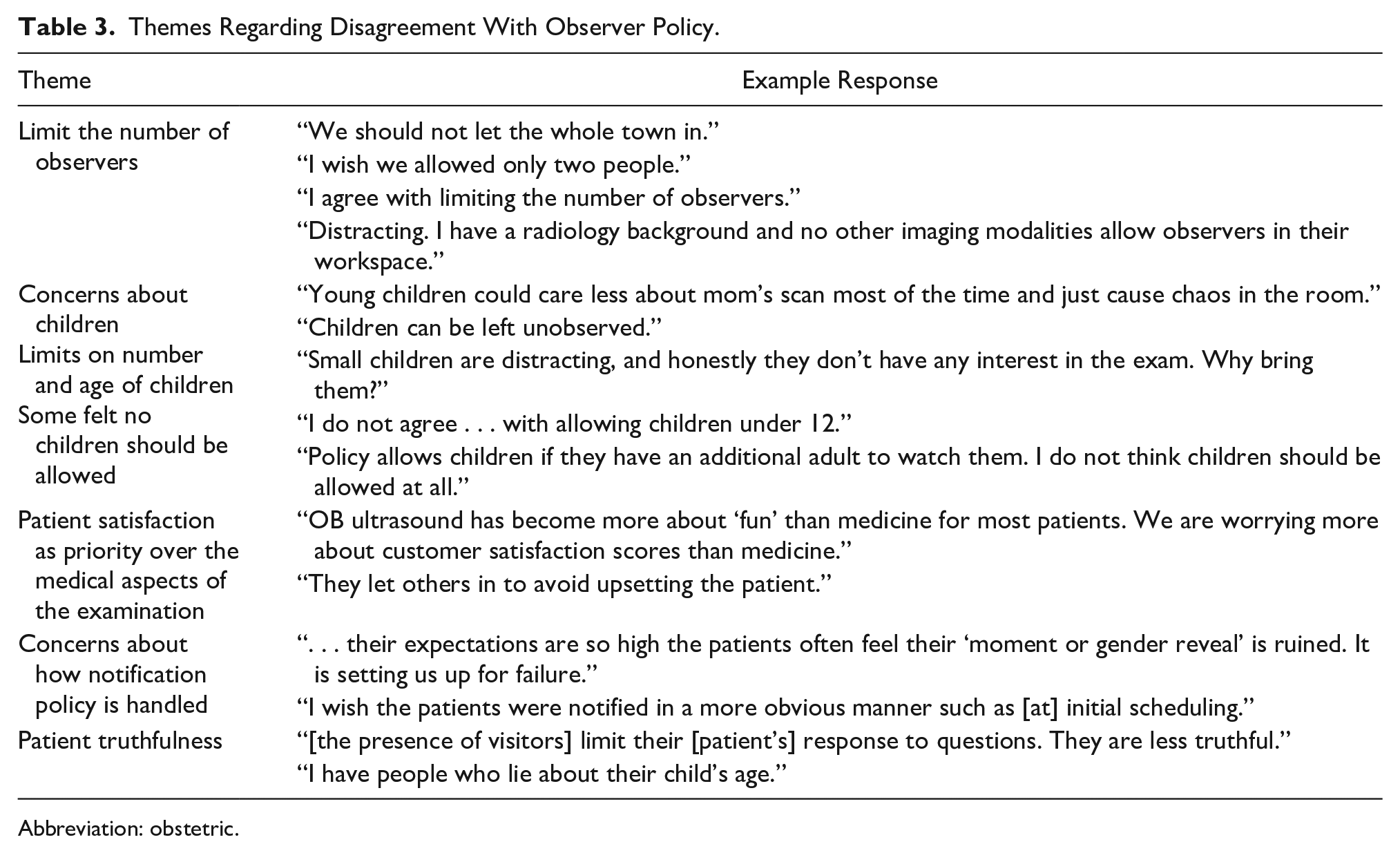
Abbreviation: obstetric.
Regarding Recording Policy
Policies which limit mobile phone or other types of recording in the examination suite were present in 85% of respondents’ practices (Table 2). Most respondents (87%) felt that patients and families often or always adhered to the recording policy, while a minority (3%) felt that patients and their families never or rarely adhered to the policy. Clinics routinely informed patients and families of their recording policy by requiring the sonographer to inform the patient of the policy at their appointment (42%) or through signs in the office (35%). Of the respondents who reported no recording policy at their practice, 85% desired one.
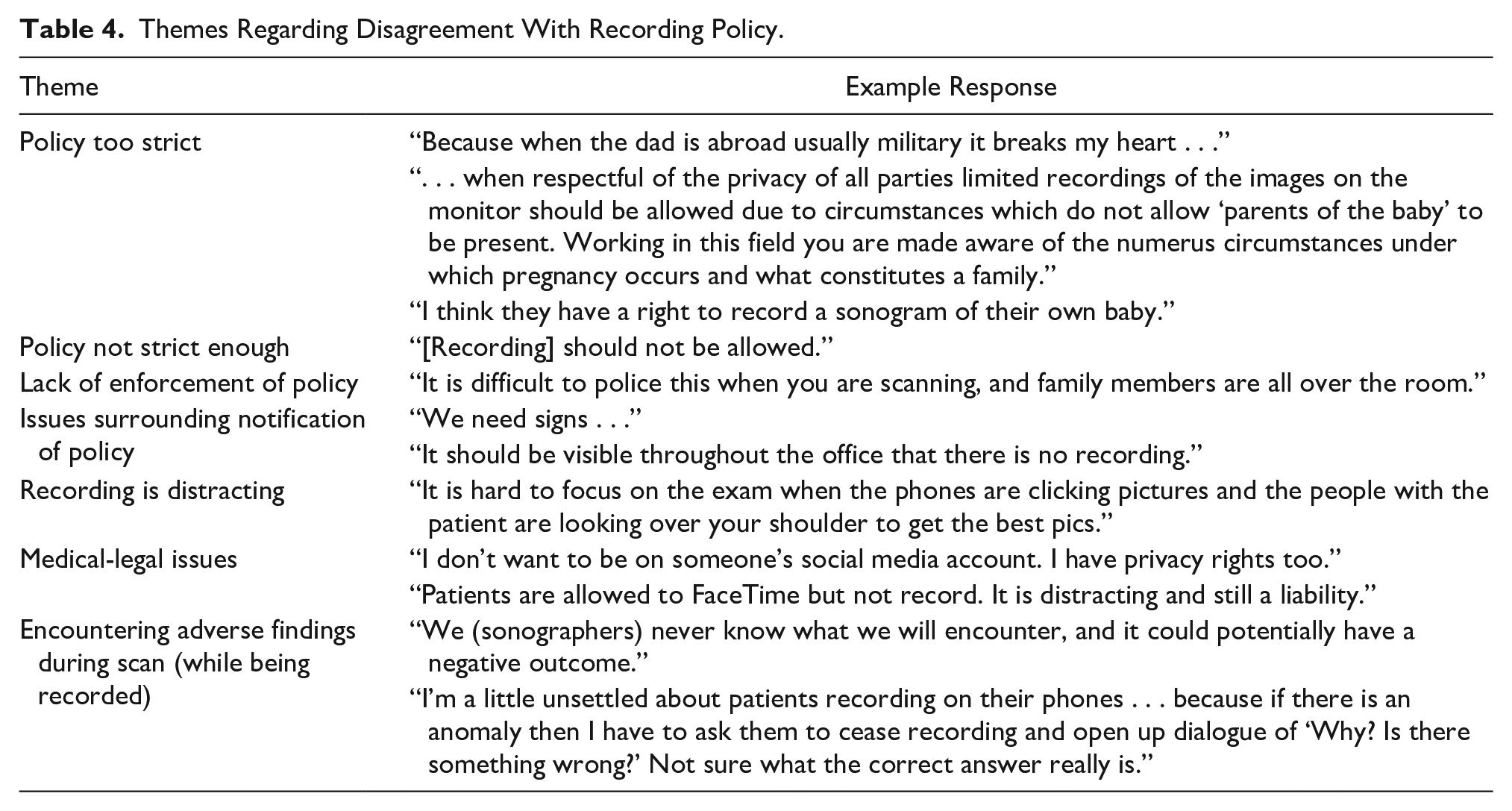
Sonographers largely agreed with the recording policy in place at their clinic (97%). There were no statistically significant associations between agreement with practice recording policies and sonographer demographics. Respondents who did not think there should be a recording policy were significantly more likely to perform 0–4 OBUS per day (P = .032). Among those who disagreed with the recording policy at their practice, 78% had dependent children (P = .0332). Ninety-five percent of those who disagreed with their practice’s recording policy responded with specific comments. The majority (75%) believed that the policy was not strict enough. Other themes were noted including the policy being too strict, a lack of enforcement/patient notification, liability/provider policy, difficulty focusing on the examination, and the issue of recording in the event of adverse findings during the examination (Table 4).
Themes Regarding Disagreement With Recording Policy.
Job Satisfaction
Participants were asked to rate how often they felt distractions from patients, children, and observers during OBUS led to decreased job satisfaction and dissatisfaction with the quality of their work. Most (80%) respondents reported that distractions, of any kind, sometimes/frequently/often resulted in them feeling a sense of decreased job satisfaction. However, a significant number of respondents (36%) reported they infrequently/never felt dissatisfaction with the quality of their work because of perceived distractions. Because these questions were asked in the context of the presence/absence of distractions, we were unable to determine if there were any associations between the presence/absence of policies and the degree of job dissatisfaction.
Discussion
This survey research demonstrated that sonographers reported confidence in existing observer and recording policies, focused on limiting distractions in OBUS. Most sonographers who worked in practices without an observer policy felt that there should be such a policy. These data suggest that sonographers who work in practices without an observer policy may wish to be protected from observer-related distractions. This also highlights that observer policies are not universally present in locations were OBUS is performed. Interestingly, not all sonographers surveyed felt that an observer policy was necessary. It is unclear why sonographers older than 50 years had a significantly higher rate of not desiring an observer policy. It could be that older sonographers have more experience in managing groups of people, have confidence asserting any needs they have to complete the scan, or perhaps this may be related to life experiences making them feel that OBUS is a “family” or “group” experience.
Similarly, sonographers working in locations without a recording policy felt that there ought to be a policy in place. Most sonographers who wanted a recording policy performed <5 OBUS per day. This contrasts with the volume of most survey respondents (performing >5 scans per day). Sonographers with low OBUS daily numbers may be performing other types of scans concurrently, perhaps explaining why they were less comfortable working without a formal recording policy.
Sonographers reported that both types of policies were well-respected and adhered to by patients. However, patients were notified of observer and recording policies in different ways which sometimes led to conflict during OBUS. Observer policies were usually communicated to patients at initial scheduling, while recording policies were primarily discussed when the patient was brought back to the examination suite at the time of their appointment. Sonographers discussed concerns about this method of policy notification, suggesting that it could be difficult for them to be the “enforcer” of the policy. The expectation that it is the sonographers’ job to notify the patient of the policy may add stress to the experience of sonographers by starting off their patient interaction with conflict. Patients and families, unhappy that they cannot record during the sonogram, may perceive the visit negatively and lodge complaints. Management of patient expectations prior to the visit could be a way to counterbalance potential negative interaction.
The findings of this study display both similarities with and differences from the results of Najafzadeh et al. 11 and Woodrow et al. 12 Similar to the Australian sonographers, sonographers in our study desired policies to limit distractions. In addition, more sonographers in the Australian study reported observer policies than sonographers in our study. 12 However, sonographers in this study perceived higher adherence to policies than sonographers in the Australian study. These findings may reflect cultural, societal, and health care infrastructure differences between the United States and Australia.
A confounding and unexpected variable was the timing of the survey and the onset of the COVID-19 pandemic. The suspicion was that there were many sonographers working reduced hours during the early weeks of the COVID-19 pandemic. This may explain the resulting response rate being lower than was expected. During this unprecedented time, many of the distractions assessed were limited by the safety measures undertaken to mitigate viral spread. For instance, for limited periods of time in our practice, no observers could accompany patients. Conversely, our recording policy was relaxed to allow patients to use FaceTime and similar video-chat software so that partners were able to virtually attend the OBUS. These COVID-19 era restrictions may have offered sonographers respite from some of the “business as usual” distractions. Changes have been made in most clinics and hospital settings to limit not only observers but also staff and number of patient visits. 16 One clinic in a remote part of Canada even trialed the use of a robotic ultrasound scanner to provide OBUS in a community isolated due to an outbreak of COVID-19. 17 While the measures are likely to be temporary, one cannot help but consider the possibility of some of the restrictions forever changing OBUS.
This survey was the first to our knowledge to be distributed to a large sonographer population in the United States. In addition, the number of respondents in our study was greater than that in other studies of obstetric sonographers.10–12,18 Finally, the anonymity of this survey may have made it more attractive to sonographers, as research has suggested that individuals are likely to be more forthcoming in anonymized surveys. 19
As with all online surveys, this study is limited by the self-identification of the participants. It is also unclear how many e-mails did not reach their intended recipients due to stale e-mail addresses or e-mails ending up in spam or junk folders (approximately 6116 e-mail links were not opened). Around 30% of recipients who opened the e-mail link went on to start the survey. Likewise, 24% of the surveys received were either ineligible for inclusion or were incomplete (Figure 1). Response bias is also a concern, as perhaps only individuals who felt strongly about the topic responded to the survey. In addition, the ability to do additional analyses related to job dissatisfaction and distractions was limited by the desire to balance data gathering with the length of the survey and time needed for completion.
This research highlights the need for further studies evaluating policies to mitigate distractions during OBUS. One area of interest is why there were more recording policies than observer policies in practices. Perhaps this is due to medico-legal issues, which for-profit centers are keen to deal with preemptively. 20 Another issue which surfaced was the difference between the ways that patients were informed of policies. In addition, further research into the sonographer’s role in the enforcement of policies and effect on sonographer job satisfaction could offer insight into not only the importance of a policy but also best practices for the writing and implementation of an effective policy.
Despite the limitations of this study, it highlights an important and much-needed dialogue about mitigating distractions for quality improvement in OBUS. These types of conversations which have been overheard in clinics, at conferences, and on blog posts 10 are just starting to be formally addressed through our study. Sonographers’ perceptions of the need for both observer and recording policies suggest that practice managers should consider developing policies to create a less distraction-filled environment for OBUS. As sonographers are highly skilled team members, job dissatisfaction and possible attrition is detrimental to the clinical team. Other stakeholders (patients, doctors, and other clinical staff) could also be surveyed to aid in developing standards for number and type of observers and the permissibility of recording during OBUS. In this way, patients and providers, along with sonographers, would be able to express common goals for OBUS. Specifics of what constitutes an effective policy should be examined as well as modes for notifying patients regarding expectations. Further examination of data collected from this survey is being undertaken to develop a “distractibility scale” of identified common distractions present in OBUS as another step toward mitigating these distractions.
Conclusion
Most survey respondents had concerns about distractions in OBUS. The majority of sonographers surveyed desired observer and recording policies and generally agreed with such policies when they were in place. However, sonographers had concerns regarding the stringency of, modes of notification for, and patient adherence to policies. Further research is needed to help develop effective policies and create standardized methods of policy dissemination to limit distractions in OBUS.
Footnotes
Acknowledgements
Table 1 was created by Taylor L. Lendrum, MD, MPH.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.