
Abstract
Body mass index is an important indicator in primary care as a measure of a specific health care outcome. As such, it can provide a quantitative basis for clinicians to achieve improvement in care and the process by which patient care is delivered. The potential impact of cardiac sonographic screening on body mass index in disadvantaged primary care patients is unknown. Changes in body mass index (BMI), blood pressure, and low density lipoprotein cholesterol (LDL-C) levels in patients who had cardiac sonographic screening were compared to changes in a control group of similar patients treated in a clinic where cardiac sonographic screening was not available. Control patients gained weight (BMI 27.8 at baseline vs. 28.3 at follow-up), while cardiac screening patients maintained weight (BMI 27.9 at baseline vs. 27.8 at follow-up, P < .05). In overweight patients those who had cardiac screening experienced better outcomes in the quality indicator BMI than control patients, yielding a statistically significant result for some subgroups of patients. Additional effort should be directed toward refining the motivational impact of cardiac sonographic screening. It appears in this particular study that cardiac screening in a community health center was associated with better control of BMI. Such screening may have a significant impact on motivating patients to take a greater interest in personal health maintenance.
Introduction
Quality indicators commonly used in primary care clinics today include biomarkers such as cholesterol levels, blood pressure, and body mass index. 1 A quality indicator is an assessment that strives to measure a particular health care outcome, and it can provide a quantitative basis for clinicians to achieve improvement in care and in turn improve the process by which patient care is delivered. 2 The aforementioned indicators are of obvious relevance to the management of patients who have heart disease, diabetes, hypertension, or metabolic syndrome. Implementation of the “medical home” concept, which envisions the primary care provider as working in partnership with patients to change lifestyle and manage chronic disease, relies heavily on indicators such as these. The medical home concept places a high priority on patient-centered care and requires patient involvement and recognition of patient needs and preferences by all involved health care providers.3,4
One could argue that body mass index (BMI) in particular is a significant biomarker that stands out as an important quality indicator. While high blood pressure and heart disease do not cause obesity, obesity certainly can exacerbate hypertension and heart disease. Although many people find it difficult to change, controlling BMI is an important goal for many patients. This article reports the results of a study to determine whether a cardiac sonographic screening service could in some fashion contribute to a lower BMI and improve other quality indicators of cardiovascular disease. This study was based on the hypothesis that this intervention would enhance these patients’ interest in taking more of an active role in their own health and wellness.
Methods
A retrospective review was carried out of patients at a community health center who received echocardiograms from 2008 through 2010, comprising the interventional group. To reduce the potential confounding effects of variations in insurance coverage and income, patients served in another community health center of similar socioeconomic status, but without access to cardiac sonographic screening, provided a control group. Institutional review boards for the clinics and Walden University approved the study prior to its initiation. All patients met the same inclusion criteria, including risk for cardiovascular events. Medical records were reviewed retrospectively at both clinics: the inclusion criteria for evaluation were patients who had risk factors for potentially developing cardiovascular disease (CVD), such as hypertension, elevated cholesterol levels, and/or diabetes.
There was no activity screen of the patients, the patients were all ambulatory, and CVD conditions such as heart failure were not a criteria utilized for excluding patients from this study. The covariates utilized in this research study were ethnicity (African American, Asian American, East Indian, Hispanic, and Caucasian), gender, and age. Since there were so few participants (N = 6) who were either East Indian or Asian American, these individuals were not mathematically figured into the overall statistical data analysis for this study. Patients had to have been seen at least three times during the three-year course of this retrospective study, involving intervals of baseline, 6 months, and 18 months, or they were excluded from this study.
The clinicians performing the screening were technical echocardiography students mentored by one of the authors, a credentialed clinical instructor (RHD, Registered Diagnostic Cardiac Sonographer [RDCS]). Their clinical rotation served as a service learning experience for the student sonographers and introduced the students to health care at free clinics in an inner-city environment. All studies were performed on a Vivid e laptop cardiovascular ultrasound system using a 1.5 to 3.6 MHz phased array probe (General Electric, Milwaukee, Wisconsin). The echocardiograms were ordered by the clinic physicians and/or the residents in training whom they supervised, and they were interpreted by cardiology fellows at a local teaching hospital.
The echocardiogram consisted of a standard study following a fixed protocol and performed with routine measurements and evaluation of ventricular wall motion and cardiac hemodynamics. The findings of the echocardiogram, whether they were normal or abnormal, had no bearing whatsoever on this study, and no repeat or follow-up studies were considered as part of this study.
BMI (defined as weight in pounds divided by the height in inches squared and multiplied by the constant 703) was computed from information extracted from patient medical records. Data for low density lipoprotein cholesterol (LDL-C), systolic blood pressure (SBP), and diastolic blood pressure (DBP) also were extracted. The outcome levels for each quality indicator measured as a biomarker were computed as the average of the scores 6 to 18 months after baseline data. Baseline levels were subtracted from outcome levels to compute changes in biomarkers. The difference in the change scores was compared for the echo group and the comparison group. Subgroups of patients were analyzed in a search for special cause variation.
Sample size calculations were made using openepi.com software offered as a professional consideration by the Centers for Disease Control and Prevention. Calculations were based on a two-tailed test using the generally accepted alpha level of α = .05, a beta level of β = .20, and a power estimate of 0.80. The power for evaluating two means was calculated with a two-sided confidence interval of 95%. Consequently, for a population of 1500 at Clinic B, a confidence interval was calculated to be 9.09, yielding a sample size of 108 in the experimental group (Clinic B) and 216 patients in the control group (Clinic A).
Data were analyzed using the difference in the difference (DID) approach, where the differences between baseline and outcome were computed by subtraction, resulting in a comparison between the difference between the two groups or clinics. This technique measures the variation induced by a particular intervention (in this case, cardiac sonographic screening) at a given period in time. The DID represents the difference between the pre- and postvalues, within subjects of the intervention and control groups. 5
Results
The majority of the participants in the study were female (57%), with the same percentage in both groups. The female population at Clinic A was 90% Hispanic, with just 7% Caucasian and 3% African American. Females at Clinic B were 68% African American, with 15% Hispanic and 16% Caucasian.
For the experimental group of 108 patients and the 216 patients comprising the comparison group, participants ranged in age from 18 to 76 years old (Figures 1 and 2). The majority of patients in the control group (Figure 1) were aged 18 to 47 (57%), and most were Hispanic (85%). Most of the patients in the echocardiography group ranged in age from 48 to 76 years (69%), and most were African American (72%) (Figure 2).
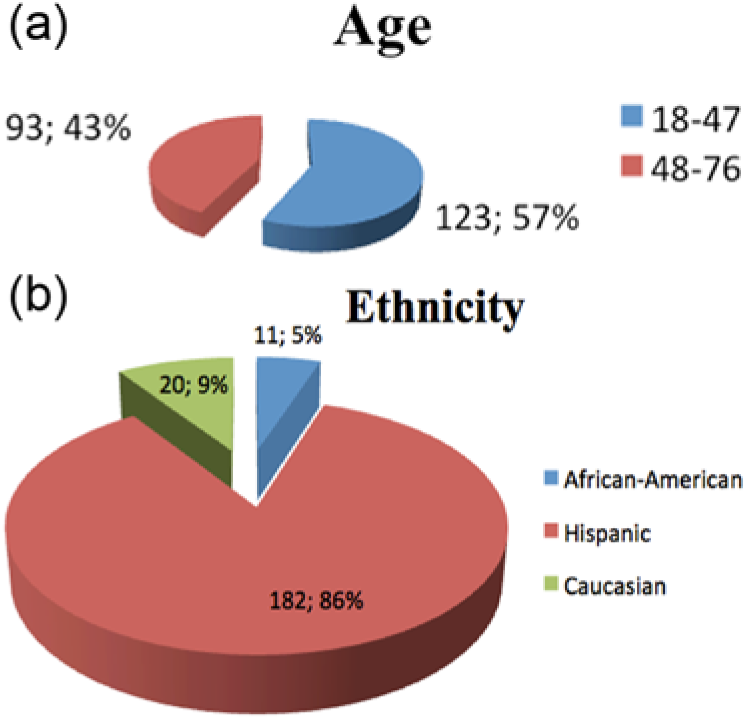
Control patient demographics: 216 patients; 57% female. (a) Age distribution. (b) Ethnicity.
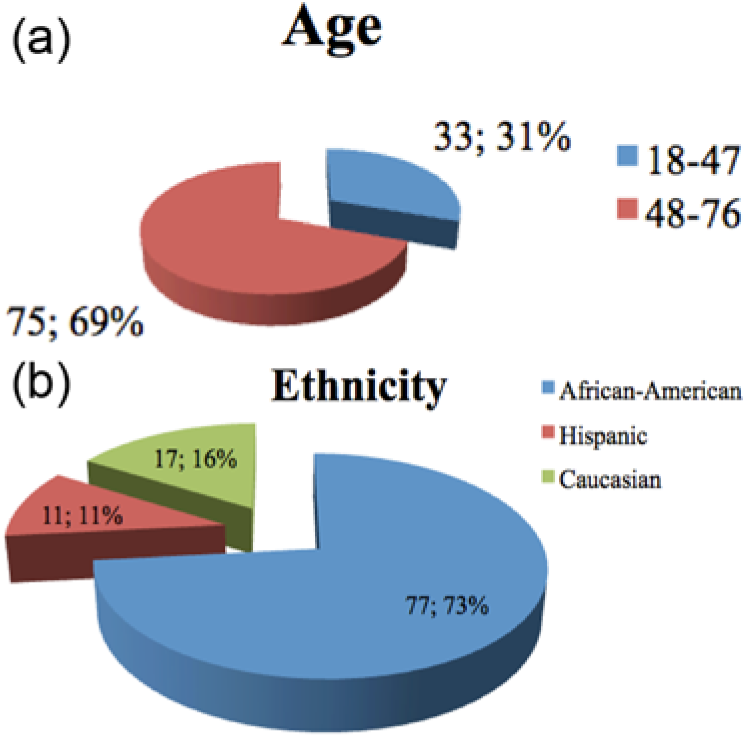
Experimental (cardiac screening) patient demographics: 108 patients; 57% female. (a) Age distribution. (b) Ethnicity.
Figure 3 shows the mean changes of the recorded variables, unadjusted for patient characteristics. In the echo group, mean changes in LDL-C, SBP, DBP, and BMI all trended in a favorable direction and were −14.57 mg/dL (P < .005), −4.53 mmHg (P < .004), −3.25 mmHg (P < .001), and −0.39 (P < .02), respectively. Changes in the comparison group were smaller and not statistically significant. The changes also were not consistently negative; the overall change in DBP and BMI in this group were positive, as shown in the figure. The figure indicates that improvements favor the echo group, but those improvements are small.
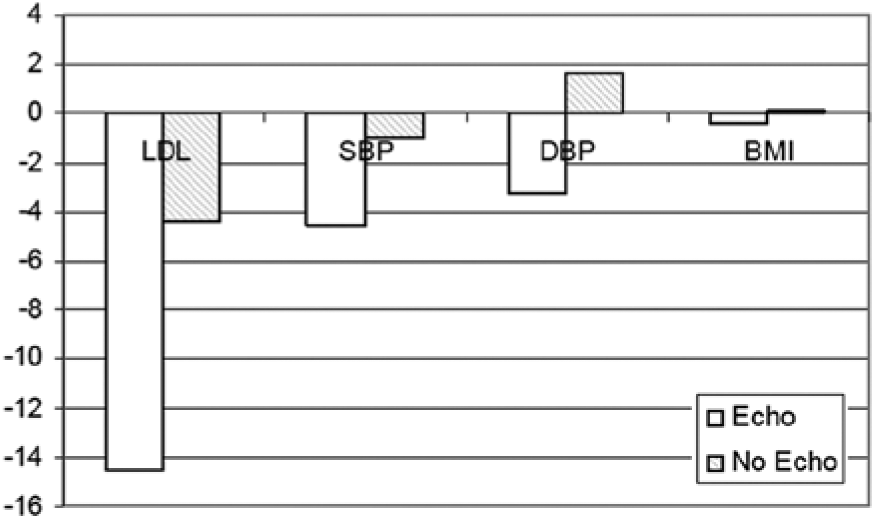
Changes in biomarkers for patients in the experimental (cardiac screening) group versus the control group. LDL, low density lipoprotein cholesterol; SBP, systolic blood pressure; DBP, diastolic blood pressure; BMI, body mass index.
The effect of screening on changes in biomarkers was significant in some subgroups of patients and but not in others. The mean change in BMI for Hispanic men in the experimental group was −0.56 (P < .02). For Hispanic women it was −1.45 (P < .02), and for Caucasian women it was −0.36 (P < .02). Caucasian men who had echocardiograms reduced their LDL-C levels by a mean of −7.86 (P = .04). Diastolic blood pressure was reduced for Hispanic women by −0.44 mmHg (P = .01) and for African American men by −1.22 mmHg (P =.03).
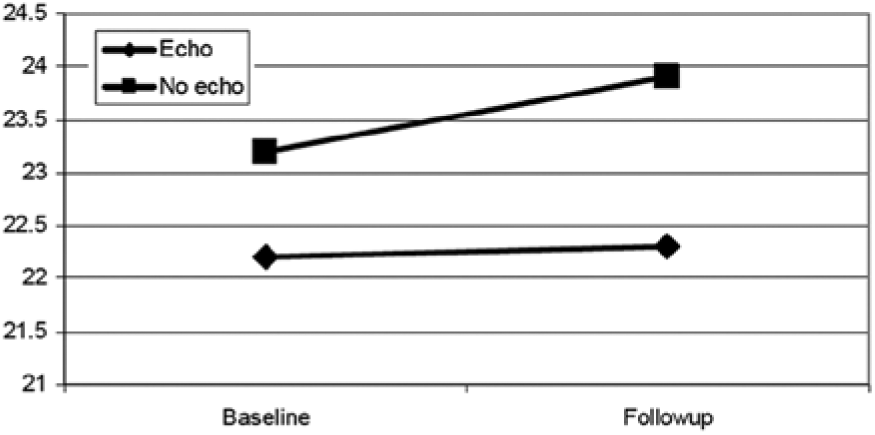
Changes in BMI were further analyzed by subdividing the cases into three groups: normal weight at baseline (BMI < 25), overweight at baseline (BMI 25–30), and obese at baseline (BMI > 30) (Figures 4, 5, and 6). Among normal weight patients, both groups gained a minimal amount of weight during the course of the study, with the echocardiography group experiencing a mean increase in BMI of 0.7, not significantly different from the increase noted in the control group of 1.07 (Figure 4). Similarly, no significant differences were seen in the slightly diminished BMI in the obese patients of both groups (Figure 5). However, among overweight patients (Figure 6), those who received the screening experienced significantly more improvement than control patients. Control patients gained weight (BMI 27.8 at baseline vs. 28.3 at follow-up), while screening patients maintained weight (BMI 27.9 at baseline vs. 27.8 at follow-up). This difference, though small, was statistically significant (P < .05).
Change in body mass index (BMI) in patients of normal weight at baseline (no significant difference).
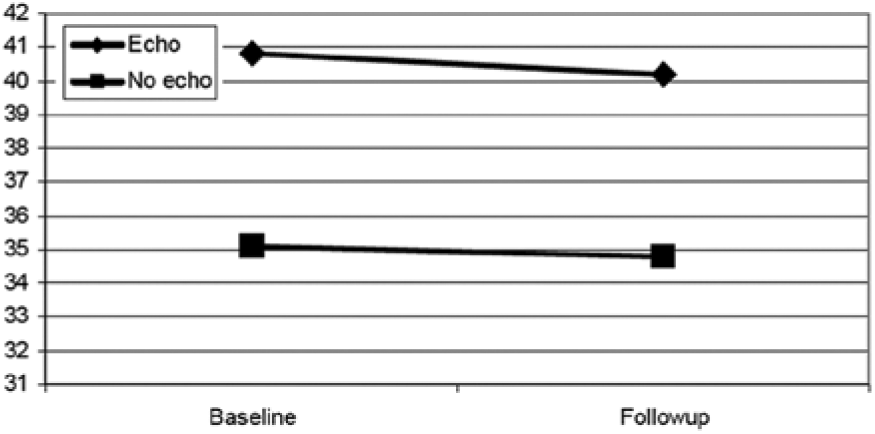
Change in body mass index (BMI) in patients noted to be obese at baseline (no significant difference).
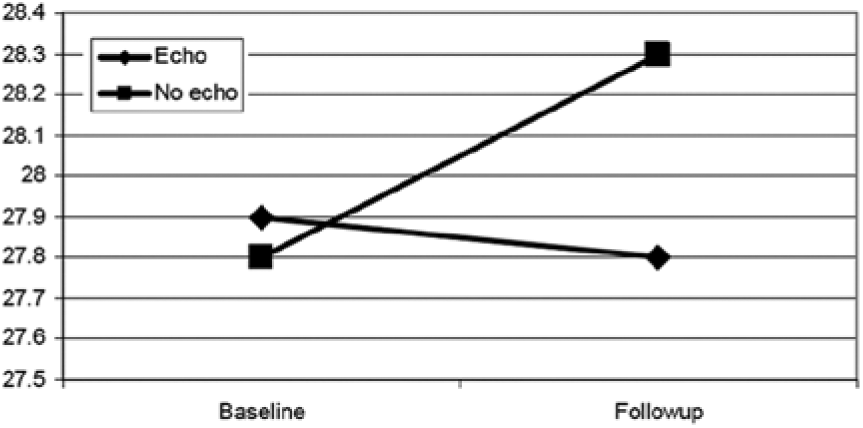
Change in body mass index (BMI) in patients noted to be overweight at baseline (P < .05).
Discussion
It has been predicted that by the year 2020, 35% of all deaths in developing countries will be caused by CVD. 6 According to the American Heart Association, several clinical and statistical research studies have examined a variety of factors that exacerbate the risk of CVD that cannot be altered, including the risk factors of age, gender, and heredity. The most significant modifiable risk factors are tobacco use, elevated serum cholesterol, high blood pressure, physical inactivity, obesity, and control of diabetes mellitus. More recently, quality indicators in the form of biomarkers have become widely applied CVD diagnostics. 7
The echocardiogram performed in this study was a routine cardiac ultrasound with standard protocol measurements. These echocardiograms were no different from studies routinely performed in hospitals and clinics throughout the United States. The studies were conducted by students and volunteer cardiac sonographers and were offered free of charge. No comparisons for the cost or efficacy of a self-help intervention were explored because it was not part of the study design or purpose. Self-help programs can offer some dramatic results; however, those benefits tend to be limited in scope and application. 8 The investigators in this study hypothesized that the results of the cardiac sonogram would provide a powerful motivational tool that might lead to changes in lifestyle.
The literature was searched for the use of cardiac ultrasound screening interventions given in conjunction with CVD biomarker assessment as part of a standard primary care evaluation. The health belief model (HBM) and the model’s applications to health behavior and health promotion have shown superb relevance in utilization of its constructs to transform this information into effective health endorsement practices. 9 The HBM was initiated by investigators at the United States Public Health Service in the 1950s. The main catalyst of the theory was inspired by a study of why people pursued x-ray examinations for the lung condition tuberculosis. The model attempted to interpret and predict a specific health-related behavior from given patterns of belief regarding the recommended health behavior and the health issues that the behavior was intended to prevent or control. 9 These investigators theorized that four conditions potentially predict a health-related behavior:
An individual has the belief that their health is in peril. If that person is seeking a screening test such as a cardiac sonogram assessing for CVD even when they are not experiencing any significant symptoms, that person must believe down deep that they are potentially susceptible.
The individual perceives that this prospective condition or disease is serious and that they could experience some degree of discomfort, lose time from work, or even potentially face some economic hardships or other problems.
The individual perceives the benefits of the given treatment to outweigh the annoyance of cooperating with the options that have been presented.
The individual receives a call to take action that makes their involvement in the process more tangible, necessitating that they need to take action.
This theory substitutes a belief in susceptibility to a disease or health condition such as CVD, recognizing that an individual could have a disease and not be aware of it, as the most significant belief explaining the rationale for people to seek screening examinations. The HBM today functions as a significant contributor to the design and implementation of public health interventions. 10 This knowledge can provide a useful framework for creating CVD prevention strategies for indigent diagnostics.
The HBM has been widely used in health behavior and health promotion interventions and provides a constructive framework for developing HBM CVD prevention skills for indigent diagnostics. According to Glanz et al., 11 the HBM is appropriate for designing health education and health intervention behavior programs such as this proposed plan. This theory of health behavior describes how people obtain and sustain certain behavioral models and can also be applied to provide the foundation for intervention strategies. The literature looks at how primary prevention strategies assist in decreasing CVD through educational means; however, it has not examined the effectiveness of CVD biomarker enhancement augmented by cardiac ultrasound strategies. There has been a great deal of research evaluating individual behavior from the perspective of the HBM, and it was the intention of this study to further confirm the effectiveness of this approach. 12
The scope of this screening looked at the role that echocardiography students would play in the delivery of cardiovascular health care services to an underserved population. This type of screening could serve as a model for replication by similar technical schools to enhance delivery of cardiac diagnostic services to an uninsured population. The echocardiogram screening involved a standard scanning protocol (2D, M-Mode, color Doppler, pulsed-wave Doppler, and continuous-wave Doppler) along with the standard dimensional measurements and calculations. The studies were interpreted within one week by a cardiology fellow (mentored by a board certified cardiologist) at a local teaching hospital, and the results were placed into the patient’s clinic chart for evaluation and treatment by their ordering physicians. The actual echocardiogram results were not evaluated as a part of this study; however, the interpreted results could have altered the course of treatment.
BMI is an important quality indicator in primary care. The BMI provides a simple numeric measure of a person’s degree of adipose tissue, allowing health professionals to talk about overweight and underweight issues objectively with their patients. Weight is an integral part of this variable; however, height is a relative constant for each adult and was a nonchanging variable in this study. It is generally accepted that a BMI of less than 25 is considered to indicate a healthy weight. A BMI that is less than 18.5 is considered underweight, and a BMI between 25 and 29.9 is considered overweight. A BMI calculated to be 30 or higher indicates that the individual is obese. 13 Everyday clinical application of BMI can assist clinicians in monitoring weight gain and limiting the untoward physical effects of obesity. It appears to have a practical application for evaluating the effectiveness of offered allied health services. 14
BMI emerged in this study as a possible quality indicator in some patient groups as a measure of the effectiveness of cardiac sonographic screening. Cultural differences between Hispanic and African American patients might have been at work in this study. Analysis of gender, racial, and ethnic subgroups revealed some effects, but these remained small. Change in BMI was more strongly related to the BMI level at baseline. Patients in the control group who were overweight at baseline tended to gain weight over the time period of the study.
In contrast, patients in the echocardiography screening group maintained weight. The differences in absolute terms were not large, but if the screening can be a factor to help prevent weight gain in overweight patients, then perhaps an effort should be made to fine-tune the intervention so that it is more powerful.
A discouragingly limited set of options are available to primary care providers concerned about BMI in their patients.15–17 Patients can be referred to commercial weight loss programs, some of which may be expensive and beyond the means of most patients in a community health center setting, and the results may be disappointing. Self-help programs are available, but dramatic benefits are exceptions rather than the rule. Meal substitutes can be effective for some patients. 18 Clinical interventions range from intensive psychosocial programs to motivational interviewing, but none can be described as highly effective. 19 Given magnitude of the obesity epidemic, the dangers associated with it, and the limitations of the treatments available, the potential benefits of even weak and uncertain interventions merit further investigation.20,21
Conclusion
BMI has become an important quality indicator for patients with a variety of chronic diseases treated in primary care clinics. Cardiac sonographic screening in community health centers appears to reduce BMI by a small but significant degree in some groups of patients. Refinements of the intervention should be considered and investigated since they may enhance its impact on patient motivation to take a greater interest in their personal health and wellness.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.