
Abstract
Objective:
To assess if distractions alter sonographers’ perceptions of an obstetric sonogram’s (OBS) quality and whether clinic policies mitigate this association.
Materials and Methods:
Members of the Society of Diagnostic Medical Sonography were surveyed regarding demographics, perceived distractions during OBS, clinic observer and/or recording policies, plus perceptions of OBS quality concerns. Distraction and OBS quality scores were calculated. Chi-squared tests were used for bivariate analysis. Logistic regression identified independent predictors of OBS quality concerns.
Results:
There were 805 surveys completed. Many respondents (68%) found more than 75% of behaviors distracting, which was associated with increased reports of OBS quality concerns (adjusted odds ratio [aOR] = 3.63, 95% confidence interval [CI]: 2.55, 5.15), despite respondents’ demographics or clinic policies. More distracting behaviors (79%, P < .01) and quality concerns (40%, P = .04) were noted by sonographers who wanted, but did not have, recording policies at their clinic. Increased quality concerns correlated with disagreement concerning current recording policies (aOR = 2.89, 95% CI: 1.11, 8.00) and desired but absent observer policy (aOR = 2.24, 95% CI: 1.09, 4.59), regardless of respondent demographics or distraction score.
Conclusion:
Increased distraction scores are associated with more sonographer reports of OBS quality concerns. The lack of desired policies was associated with increased distractions and quality concerns. Further work is needed to understand the relationship between clinic policies, perceived distraction, and OBS quality.
Medical errors have been shown to cause financial, emotional, and physical harm to hospital systems, healthcare workers, and patients. 1 Estimates, made in 2016, indicated medical errors are the third leading cause of death, in the United States, and caused approximately 400,000 deaths per year. 2 Distractions, including auditory, visual, and mental interruptions from patients and their families, during the administration of healthcare services are known to contribute to the occurrence of medical errors, in a variety of healthcare settings.3–5 Limited research has been done to assess the impact of distractions on the quality of obstetric sonography (OBS).
The experience of obstetric sonographers differs from that of practitioners of other imaging modalities where there are specific rules about observers and the use of recording devices. 6 Non-patient observers are often explicitly prohibited during magnetic resonance imaging (MRI), radiology, and computed tomography (CT) procedures, and technologists themselves cannot be in the room with the patient, while using the equipment. Mobile phone use is discouraged, if not prohibited, near most MRI, radiology, and CT equipment in clinics and hospitals. 7 Furthermore, with many specialties of sonography, guests are not encouraged and discussion, about the recorded images, is kept to a minimum. 8 However, no restrictions exist during OBS. Interruptions and distractions are commonplace in the OBS examination room, creating a loud, chaotic, and a possibly disruptive work environment for sonographers. The implementation of policies to reduce the use of electronic devices and limit the number of people present during the administration of healthcare services, have been shown to reduce the incidence of medical errors. 4 To determine if there is research on policies to limit observers and recordings during OBS, a search was conducted of PubMED and Google Scholar using the keywords “ultrasound and recording,” “ultrasound and observer,” and “ultrasound and visitor.” A blog post from American Institute of Ultrasound in Medicine (AIUM) 9 and a 2019 study from Australia and New Zealand 10 were the only publications found. In addition, AIUM guidelines yielded minimal results. The blog post on the AIUM website reported a survey assessing the presence of recording policies in OBS, which highlighted the need for institutional policies to limit distractions that may impede image quality. 9 A 2019 study surveying sonographers/sonologists (n = 393) in Australia and New Zealand found that 86.6% believed distractors impact the quality of OBS examinations, but further research was needed to determine which distractions most impede quality. 10
The goal of this cross-sectional survey was to characterize common distractions present during OBS and identify associations between sonographers’ level of distraction and perceived OBS quality concerns. In addition, this study determined if the presence of observer and recording policies, aimed at limiting distractions, mitigated the association between level of distraction and OBS quality concerns.
Materials and Methods
The survey design was adapted from previously published work by Najafzadeh et al. 10 Questions that were irrelevant to practice in the United States were removed. Additional items were added based on clinical experiences within our practice. Prior to use, the survey was reviewed by a convenience sample of obstetric sonographers and Maternal-Fetal Medicine physicians for content and clarity. The final survey contained 78 discrete, Likert scale, and open-ended questions which assessed sonographer demographics, impressions about distractions present during OBS examinations, the presence of observer and/or recording policies at their practice location, the degree of adherence to any policies, and sonographer experiences of OBS quality concerns. To fully complete the survey was estimated to take approximately 5 to 10 minutes. The Research Electronic Data Capture (REDCap) 11 software platform was used to distribute the survey and collect data. The Institutional Review Board approved this research (COMIRB 20-0251). The survey can be accessed https://redcap.link/hct5dmxi. Survey links were emailed to members of the Society of Diagnostic Medical Sonography (SDMS), an organization including sonographers, students, educators, physicians, nurses, and other healthcare providers who are either practicing or have an interest in diagnostic medical sonography. 12 There were approximately 9,641 nonstudent SDMS members practicing OBS, who received the survey, in February 2020. In March 2020, anonymous survey links were emailed through the SDMS listserv of non-student members practicing OBS. A follow-up email was sent approximately 2 weeks later as a reminder to complete the survey.
Respondents were asked to rate how distracting they found 30 behaviors in three categories: (a) child behaviors (9 items), (b) patient behaviors (12 items), and (c) observer behaviors (9 items). Respondents could rate each behavior on a 5-point Likert-type scale from “very distracting” to “not at all distracting.” Responses were then dichotomized as “distracting” (very, moderately, or slightly distracting) versus “not distracting” (neutral or not distracting at all). The percent of behaviors respondents rated as distracting, as well as the percent for each of the three categories (child, patient, and observer behaviors), were computed. These percentages were then dichotomized as ≥76% termed “more behaviors distracting” versus <76% termed “less behaviors distracting.”
Additional questions pertained to practice policies and sonographer experiences of OBS quality concerns. Respondents were asked yes/no questions concerning the presence or absence of observer and recording policies at their practice, their agreement/disagreement with policies, or the desire for policies if none were in place at their practice. Questions about OBS quality, defined as how frequently the respondent felt negative outcomes occurred during an examination, were assessed through a 5-point Likert-type scale (1 = Often, 5 = Never). Likert-type scale responses were collapsed into two groups: (a) quality concerns present (often/very frequently/sometimes) and (b) quality concerns absent (never/infrequently). Respondents were again given a score to indicate the percentage of OBS quality concerns they had experienced. These percentages were then dichotomized as ≥76% termed “experienced more quality concerns” versus <76% termed “experienced less quality concerns.”
Chi-squared analyses were performed to examine relationships between level of distraction, presence of observer and/or recording policies, and experienced quality concerns. Logistic regression examined the relationship between the occurrence of quality concerns, presence of practice policies, level of distraction, and sonographer demographics. To identify independent predictors of quality concerns, we used logistic regression models that included any variables that were significant in bivariate analyses (P < .05), level of distraction, and the presence of policies.
Results
Survey responses were collected electronically from March 3, 2020, to April 3, 2020. Of the 9,641 OBS practicing SDMS members who were emailed the survey, 3,525 clicked on the survey link, and 805 responses were eligible for analysis (see Figure 1).
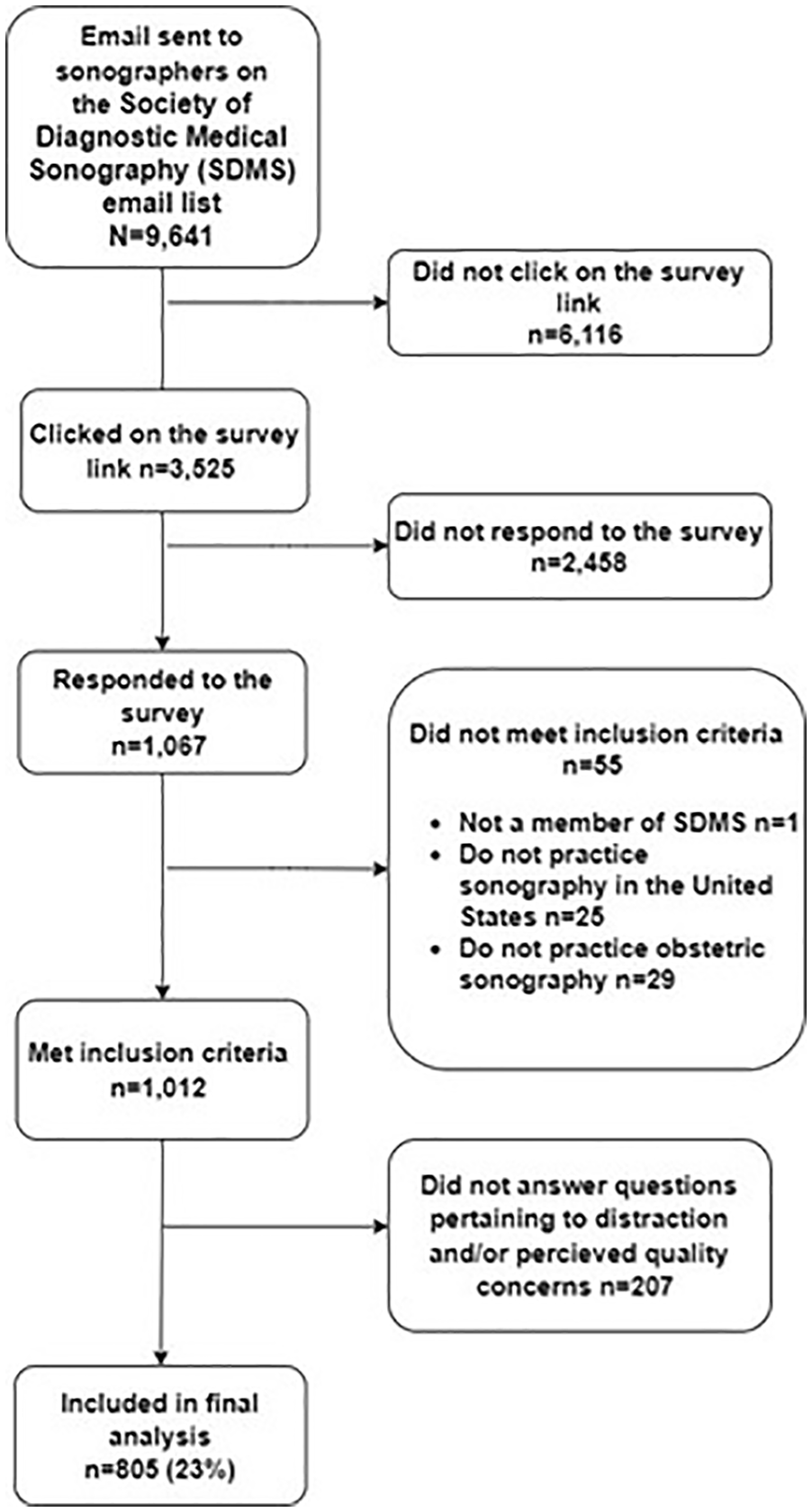
The flow chart for the study population included in data analysis.
Most survey respondents were female (94%) with a median age of 49 years (see Table 1). About half of respondents reported having dependents. The median years of experience was 20 years, with 74% of respondents having greater than 10 years of experience. Most respondents did not have an advanced degree (i.e. master’s degree, graduate degree, medical degree, or PhD) (86%), practiced in suburban settings (45%), reported performing between more than four OBS per day (56%), and performed OBS more than 3 days per week (63%) (see Table 1).
The Demographic Characteristics of the Study Population.
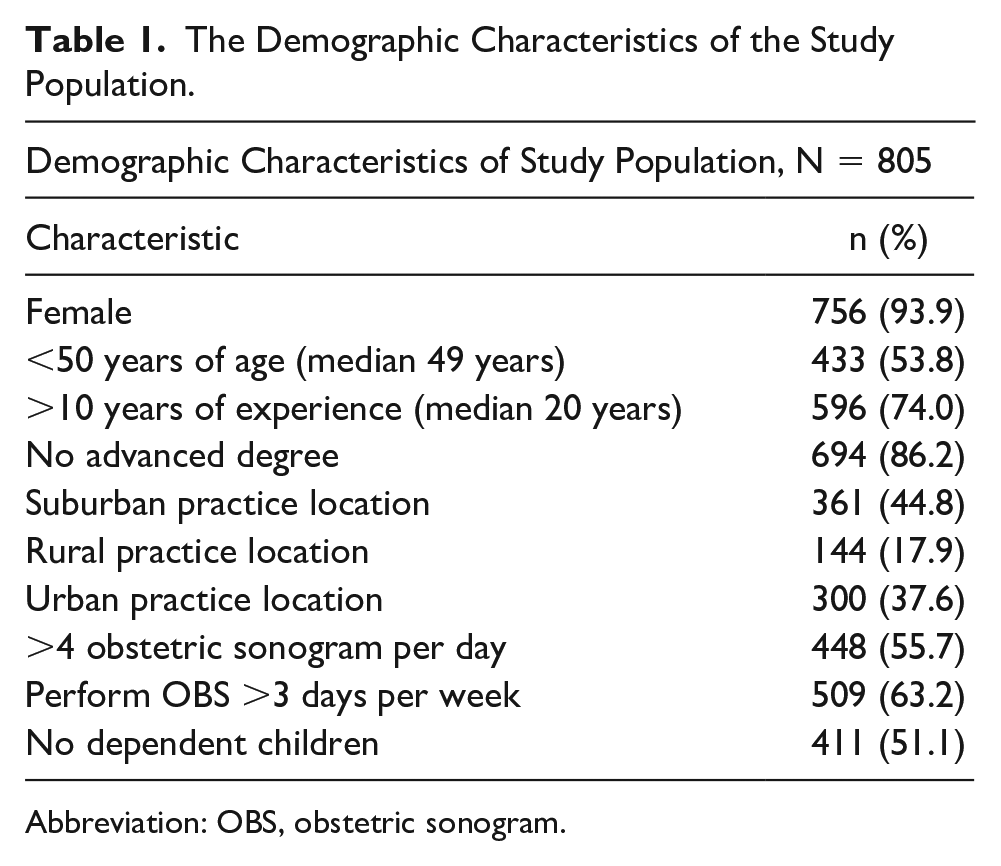
Abbreviation: OBS, obstetric sonogram.
Most respondents found observer (84%) and child (62%) behaviors distracting. However, many respondents (53%) found fewer patient behaviors distracting. Most respondents (68%) found more behaviors, among all behavior groups, distracting (see Figure 2).
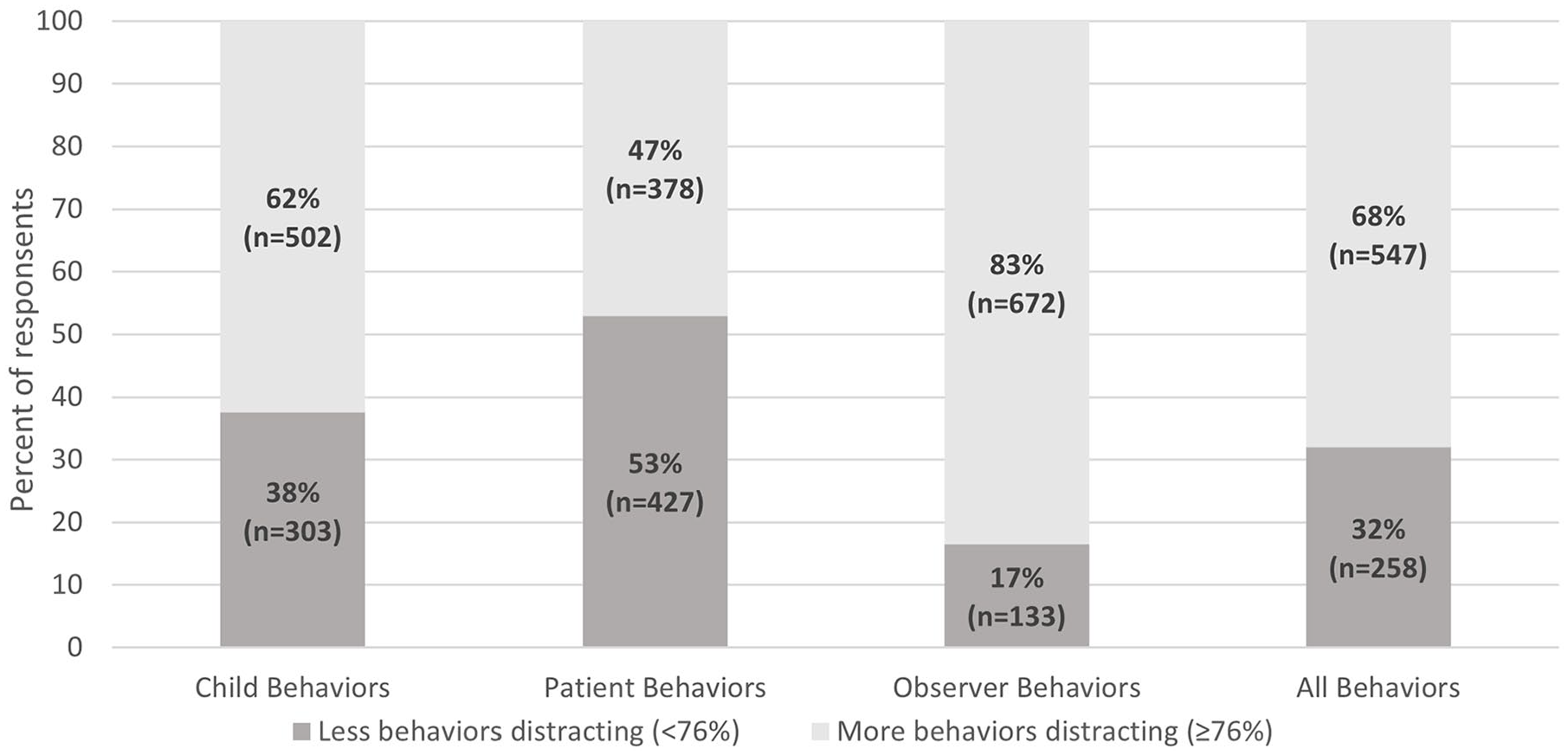
The percent of respondents reporting less or more distractions, by behavioral group.
Most respondents who found less behaviors distracting had more than10 years of experience (80% vs. 72%; p=0.02) and practiced in a suburban setting compared to urban or rural settings (45% vs. 32% vs. 22%; P = .03). Among respondents who found more behaviors distracting, most (57% vs. 48%; P = .02) were less than 50 years of age (see Table 2).
The Study Respondent’s Characteristics by Level of Distraction (N = 805).
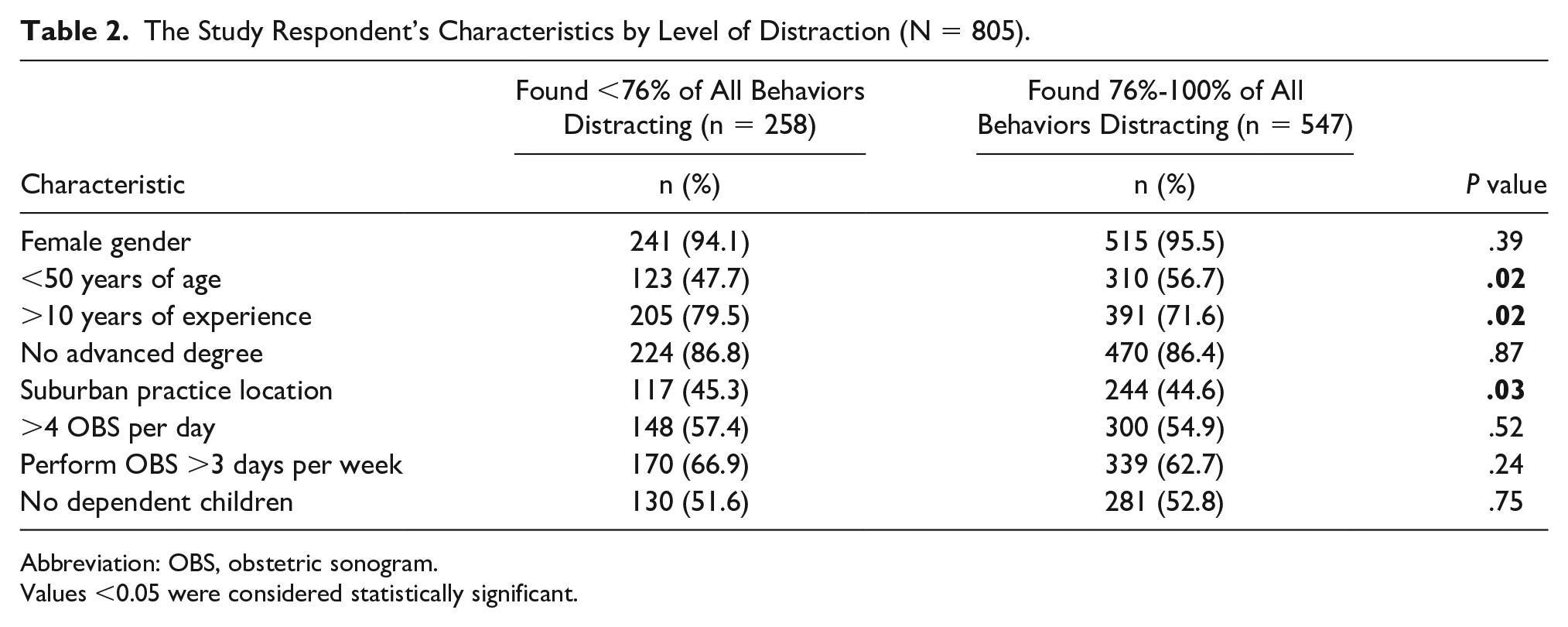
Abbreviation: OBS, obstetric sonogram.
Values <0.05 were considered statistically significant.
Observer Policy
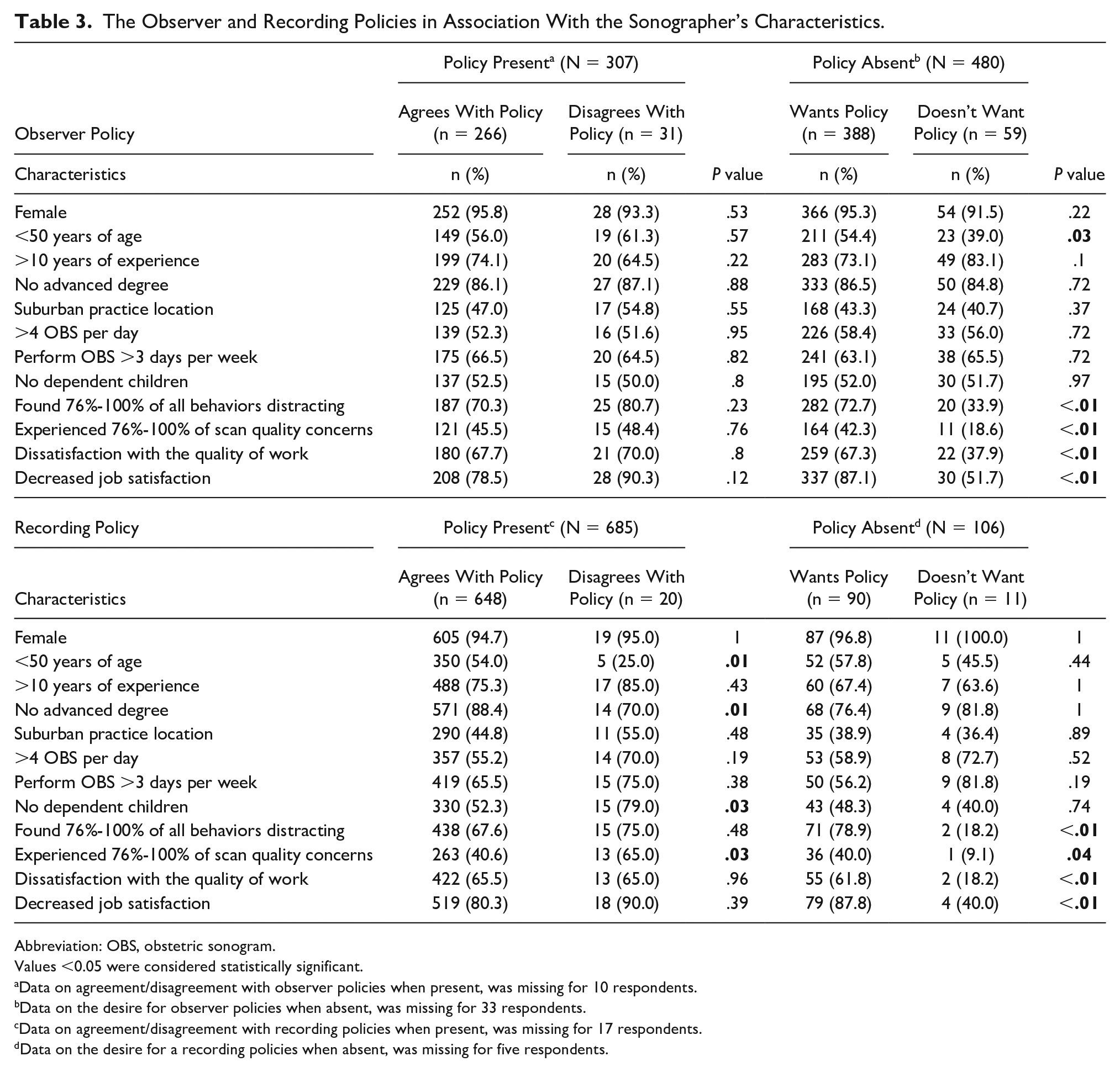
Thirty-eight percent of respondents reported there was an observer policy, at their practice, limiting the number and types of individuals allowed to accompany patients, during an OBS. Among respondents with an observer policy in place at their practice, 87% reported agreement with the policy. Agreement with current observer policy was not associated with distraction score quartile (P = .23) or percentage of experienced OBS quality concerns (P = .76). Most respondents (81%) who did not have an observer policy at their practice, desired one. Most sonographers who desired an observer policy found more behaviors distracting (73% vs. 34%, P < .01), experienced more OBS quality concerns (42% vs. 19%; P < .01), reported dissatisfaction with the quality of their work (67% vs. 38%; P < .01), and indicated decreased job satisfaction (87% vs. 52%; P < .01) (see Table 3).
The Observer and Recording Policies in Association With the Sonographer’s Characteristics.
Abbreviation: OBS, obstetric sonogram.
Values <0.05 were considered statistically significant.
Data on agreement/disagreement with observer policies when present, was missing for 10 respondents.
Data on the desire for observer policies when absent, was missing for 33 respondents.
Data on agreement/disagreement with recording policies when present, was missing for 17 respondents.
Data on the desire for a recording policies when absent, was missing for five respondents.
Eighty-five percent of respondents reported there was a recording policy in place at their practice. Most sonographers (95%) who practiced at a location with a recording policy agreed with the current policy. Sixty-five percent of sonographers who disagreed with the recording policy experienced many OBS quality concerns (P = .03). Agreement with current recording policies was not associated with respondents’ distraction score quartile (P = .48). Most respondents (85%) who did not have a recording policy, desired one. The majority of respondents who desired a recording policy when one was absent, found more behaviors distracting (79% vs. 18%; P < .01), experienced more OBS quality concerns (40% vs. 9%; P = .04), reported decreased quality of their work (62% vs. 18%; P < .01), and indicated decreased job satisfaction (88% vs. 40%; P < .01) (Table 3).
Quality Concerns
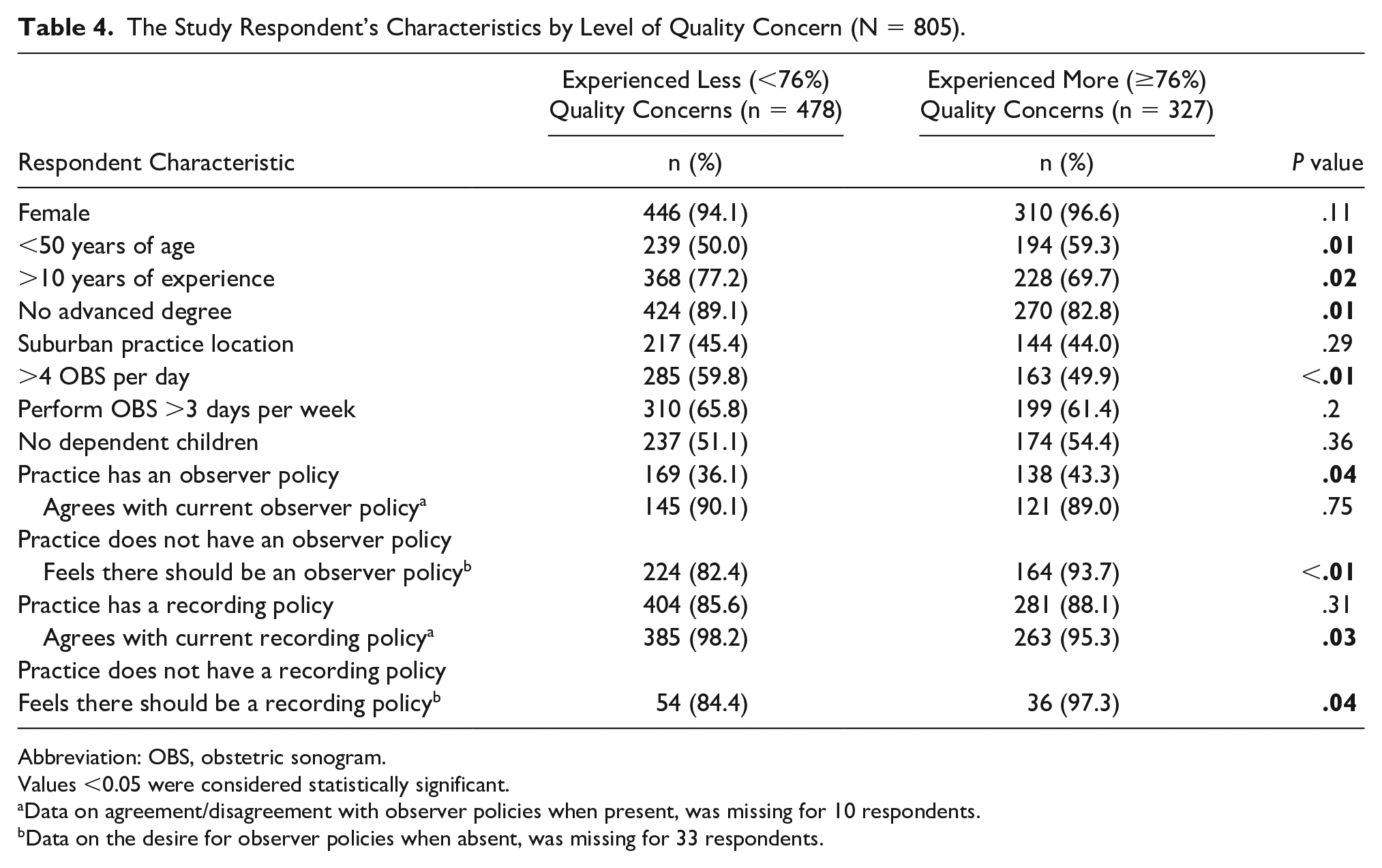
The most reported OBS quality concerns were incomplete systemic scans (78%), poor patient communication (77%), and poor patient experience (74%). Most respondents (59%) reported experiencing less OBS quality concerns. Respondents, who reported experiencing less-quality concerns, were more likely to have greater than a decade of experience (77% vs. 70%; p = .02) and more likely to perform more than 4 OBS per day (60% vs. 50%; P < .01), yet they were less likely to have an advanced degree (89% vs. 83%; p = .01). Respondents reporting more quality concerns were more likely to be less than 50 years old (59% vs. 50%; P = .01) (see Table 4).
The Study Respondent’s Characteristics by Level of Quality Concern (N = 805).
Abbreviation: OBS, obstetric sonogram.
Values <0.05 were considered statistically significant.
Data on agreement/disagreement with observer policies when present, was missing for 10 respondents.
Data on the desire for observer policies when absent, was missing for 33 respondents.
When controlling for respondent’s age, years of experience, practice setting, and distraction quartile, the presence of, agreement with, and desire for policies were compared to respondents’ reports of “less” vs. “more” quality concerns. The desire for an observer policy when one was absent significantly increased reports of quality concerns (aOR=2.24, 95% 1.09, 4.59). Disagreement with current recording policies significantly increased reports of quality concerns (aOR=2.89, 95% CI 1.11, 8.00).
Less quality concerns were reported by sonographers who did not have an advanced degree, had greater than 10 years of experience, and performed more than 4 OBS scans per day. However, age less than 50 was associated with reporting more quality concerns. Sonographers who reported finding more behaviors distracting, particularly behaviors associated with children and observers, experienced more quality concerns. Agreement with current observer policies was not associated with distraction score quartile or quality concern quartile. Still the desire for an observer policy when one was absent was associated with finding more behaviors distracting and leading to increased quality concerns. Similar findings were seen with recording policies; agreeing with the current recording policy was associated with having less quality concerns while a desire for a recording policy when there was none, was associated with finding more behaviors distracting and having more quality concerns.
Discussion
There is limited research, particularly in the United States, assessing the relationship between practice policies, distractions present during the administration of an OBS, and the combined effects on exam quality. This data suggest higher levels of distraction, particularly related to child and observer behaviors, being associated with an increase in reported OBS quality concerns. Unfortunately, respondents indicated many behaviors distracting overall (68%) and by behavior group (83% observer behaviors, 62% child behaviors, and 46% patient behaviors). Given this high prevalence of distractions, it has been posited that sonographer perceived OBS quality concerns may be mitigated by limiting distractions during the exam, particularly those caused by observers and children.
While the presence of observer and recording policies was not significantly associated with the distraction score quartile or reports of OBS quality concerns, finding more behaviors distracting and experiences of many quality concerns were reported by sonographers who wanted, but did not have, recording or observer policies at their practice. Moreover, agreement with present recording policies was associated with reporting fewer quality concerns. The lack of a linear association between presence of policy and distraction score quartiles may be partially related to the findings that policies are variably communicated to patients and enforcement is also varied. 13 Furthermore, some of the quality concerns may be related to sentiments expressed in the freeform comments regarding medico-legal, privacy concerns and handling of anomalies in situations where no policy is present. 13
In this study, having more than 10 years of experience, performing on average more than 4 OBS per day, and not having an advanced degree, reduced quality concerns, while being less than 50 years of age was associated with experiencing many quality concerns. These findings are usually consistent with the general tenant that increased patient volumes and experience improves quality. 14 It is unclear why not having an advanced degree reduced quality concerns. However, it is possible that sonographers without advanced degrees may not recognize the consequences of distractions in the exam room.
In November 2017, the AIUM reported, in an organizational communication, the results of a survey which assessed the presence of recording policies in OBS. 9 While not published in a peer-reviewed scientific journal, the results of the survey highlighted a need for an in-depth analysis of practice policies, distractions, and the effects of both on sonographer performance. Previous research on this topic conducted in Australia and New Zealand in 2019 determined that distractions present during the administration of OBS impacted image quality, but further research was needed to determine which distractions most impeded quality. 10 In addition, for Najafzadeh et al the preceding information did not address the relationship between presence or absence of observer and recording policy on both sonographer distractibility and OBS quality. As the structure of the healthcare system in the United States differs from the health care system in Australia and New Zealand, sonographer work environments and processes are thus likely different. A recent publication by Woodrow et al 15 discussed the need for policies to minimize distractors during OBS, but the generalizability of the study is limited by the sample size and practice location.
This study suggests sonographer-endorsed policies may help mitigate the effect of patient/observer level of distractions on OBS quality. A prospective study with a policy designed and supported by sonographers looking at both subjective and objective concerns about quality (such as examination time, percentage of OBS with complete visualization of all anatomic structures, and missed anomalies) could better inform how policies limiting distractors may improve quality. Any study looking at policy should also evaluate at how patients/families are notified of the policies and how they are enforced, since this was a concern previously reported. 13 Furthermore, patient/family satisfaction could be impacted if a policy is viewed as too restrictive by the patient or family, which may have unintended consequences for engagement in care and the relationship with the healthcare system. Patient/family perception of how their behavior impacts the quality of the OBS will be important to monitor.
This study was endorsed by an internationally respected organization of sonographers (SDMS) and was sent through their listserv to 9,641 SDMS members practicing OBS in the United States. The number of our respondents was greater than other studies of obstetric sonographers.9,10,15,16 The anonymity of this survey may have made it more attractive to sonographers, as research has suggested that individuals are likely to be more forthcoming in anonymized surveys.17,18
Limitations
There were some limitations to this work which included the possibility of volunteer bias given that the survey was completed only by those interested, after the initial email. This may have excluded a specific subset of sonographers. To ensure survey responses were anonymous, SDMS members were emailed a link to the REDCap. By clicking on the survey link, it automatically created a survey event in REDCap for the respondent. There is the possibility respondents clicked on the survey link multiple times creating multiple survey entries in REDCap, though the authors consider this unlikely as those that wished to stop and start the survey were provided a REDCap survey return code. Those that did not use the return code to complete unfinished surveys may have started a new survey leaving the previous survey incomplete. These incomplete survey responses would have been excluded (see Figure 1). In addition, survey questions could have been interpreted differently across participants or differently than was intended by the surveyors. Because the survey was adapted from previous work done in Australia and New Zealand where there are health care practice differences comparatively to the United States, the design of the survey may have also been biased, resulting in leading questions regarding distractors.
The timing of the survey and the onset of the COVID-19 pandemic may be a confounding factor in the results. It is suspected that there were many sonographers working reduced hours during the early weeks of the COVID-19 pandemic, as a result, the response rate was lower. During this unprecedented time, many of the distractions assessed were limited by the safety measures undertaken to mitigate viral spread. Changes have been made in most clinics and hospital settings to limit not only observers but also staff and number of patient visits. COVID-19 pandemic restrictions could have offered sonographers respite from common distractions.
Conclusion
The desire for practice observer and recording policies when absent was associated with sonographers finding more behaviors distracting and reporting more OBS quality concerns. The desire for an observer policy when one was absent and disagreement with recording policies when one was present were associated with increased reports of OBS quality concerns among sonographers. This study suggests that sonographer-endorsed policies may help mitigate the effect of distractions on OBS quality.
Footnotes
Acknowledgements
The authors thank Dr Heather Aldrich and Dr Emily Su for their help with manuscript preparation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
We did receive IRB approval for this project. The study was exempt from full-review and was approved by the University of Colorado IRB (COMIRB # 20-0251).
Informed Consent
Informed consent was not sought for the present study because all case data was de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).
Animal Welfare
Guidelines for humane animal treatment did not apply to the study.
Trial Registration
Not applicable.
Key Takeaways
In practices without observer or recording policies, sonographers who desired policies found more behaviors distracting and experienced greater obstetrical ultrasound quality concerns than did sonographers who did not desire policies.
Agreement with current recording policies resulted in fewer obstetrical ultrasound quality concerns.
Additional years of experience and performing more frequent obstetrical ultrasounds in a day reduced quality concerns related to distractors.
Adoption of observer and recording policies aimed at reducing distraction could improve the quality of obstetrical ultrasounds.