
Abstract
Objective:
Focused assessment with sonography for trauma (FAST) is a widely used imaging technique for the diagnosis of blunt abdominal trauma and has its limitations and advantages. A meta-analysis was completed to evaluate the reliability of FAST, in the diagnosis of blunt torso trauma.
Materials and Methods:
A search was completed with Google Scholar, PubMed, National Center for Biotechnology Information (NCBI), MEDLINE, and Medscape databases, from 1993 up to 2020. Eligible studies were included for information about FAST examination of abdominal trauma. The animal research was excluded from this review process. The eligible studies were first categorized and then data analysis was performed, according to specific pathologic conditions. This literature review retrieved studies’ sample size, application, sensitivity, and a specificity of diagnosis using FAST for abdominal trauma.
Results:
In total, 100 articles were identified through the database search. Besides, five articles were identified through other sources. Then, screening was performed, and as such, 46 published studies were included that had a qualitative synthesis.
Conclusion:
FAST has a high sensitivity and specificity in the diagnosis of blunt abdominal trauma. However, a large range of sensitivity and specificity of FAST in the evaluation of torso trauma reveal that sonography is operator, technique, and equipment dependent.
Keywords
Trauma is the most common cause of death among youth and adults, specifically aged 1–45 years. 1 Generally, body trauma has been an increasingly health care issue problem and is attributed to extensive transportation and the rapid increase in population growth. 2 The annual incidence of torso trauma is more than five million, resulting in more than 500 000 operations and 50 000 deaths. 3 Trauma deaths result, on average, in 40 years of life lost and 18 years of productive life lost. 3 Abdominal trauma is present in 7%–10% of all trauma victims. 4 Abdominal injuries require surgery in about 25% of cases, and 85% of abdominal traumas are of blunt character. 5 The presence of blunt abdominal trauma (BAT) along with other injuries poses a difficulty in diagnosis and can account for higher mortality and morbidity. The most common causes of BAT are road traffic accidents followed by pedestrian accidents, abdominal blows, and fall from heights. 5 BAT is very common, and the prevalence of associated intra-abdominal injury has been reported to be as high as 12%–15%. 6 The mechanisms resulting in BAT have been reported as motor vehicle collision (73%), motorcycle collision (7%), auto-pedestrian collision (6%), and falls (6%). 6 In approximate order of frequency, the most commonly injured abdominal organs and structures are the spleen, liver, kidneys, small bowel and/or mesentery, bladder, colon and/or rectum, diaphragm, pancreas, and major vessels. 7 Sonography is a simple, portable, repeatable diagnostic test that involves no radiation and can be completed quickly at the patient’s bedside. 8 In infancy, BAT is a prevalent clinical event. An accurate evaluation needs a thorough understanding of the injury pattern and the child’s reaction. Repeated examinations of the patient have the chance to produce superior clinical judgment, in a more comfortable setting.
The focused assessment with sonography for trauma (FAST) evaluates the presence of free fluid, around the heart and three areas of the abdominal-pelvic cavity. Most traumatic deaths occur early and are due to injuries in the airway, brain, or thoracoabdominal cavity. FAST has become a standard adjunct to the secondary survey in trauma resuscitation and, in many institutions. In some facilities, FAST has replaced diagnostic peritoneal lavage. 9 FAST is a goal-directed diagnostic study that determines whether intraperitoneal fluid is present. It is a safe and quick diagnostic tool that can be learned easily. It is of great value for those patients who are hemodynamically unstable and who cannot be shifted to computed tomography (CT) suite. The great value of FAST lies in its high sensitivity for detecting intraperitoneal fluid which accumulates in independent areas around the liver, spleen, and pouch of Douglas. This sensitivity may reach up to 100%. 10 In FAST, the following spaces are evaluated for the sole purpose of detecting hemorrhage: pericardium, hepatorenal fossa, left subphrenic space, right and left paracolic gutters, and the pouch of Douglas. 7 The reported sensitivity of FAST has been wide ranging. The diagnostic accuracy of FAST, in children, is particularly different, compared with adults. 11 The FAST technique can be extremely specific but insensitive in pediatric patients, in detecting free intraperitoneal fluid. Combining FAST and a physical examination can add importance to BAT compared with FAST technique alone. 12 Surgeons, radiologists, doctors, and trainees usually perform the FAST technique after extensive training, which includes lectures and practical experience; however, a lack of a structured curriculum exists. Competency-based evaluation of FAST, during training, can be challenging. 13 Sonographic quality and skills have been suggested as part of the FAST training validation, as this can assist in discriminating between a novice and an expert. 14 It has been shown that extending FAST training with nurses will significantly improve their abilities in the emergency department. Following a 1-day lecture, hands-on sessions, and completing more than 25 FAST examinations, participants demonstrated 84.4% awareness, 98.4% specificity, 94.2% positive predictive values (PPVs), and 95.3% negative predictive values (NPVs). 15 There are few limitations with the FAST technique, which include the inability of visualizing the left upper quadrant of the abdomen, as it requires more effort and expertise to visualize. 16 The FAST technique also gives poor picture gain, suboptimal depth, and reverse orientation of the transducer which are often reduced with repeated tests, reflecting perhaps more operator experience. The equilibrium between sensitivity and specificity is another challenge of performing FAST. 17 Both false-positive and false-negative tests could lead to unfavorable diagnostic results which could cascade into an unnecessary surgery. Health care providers should conduct FAST with caution to prevent a false-positive result. Another drawback of the FAST technique is the limited identification of retroperitoneal and small amounts of intraperitoneal fluids. 18 Moreover, emergency FAST (E-FAST) may ignore pneumothorax, especially in regions surrounding lung apices and bases, which accounts for two-thirds of false-negative testing. 19
Blunt torso trauma leads to thousands of admissions each year, leading to high expenses for the health care system. 19 While the real injury is managed by the health care team, the prevention of such accidents is also the focus. Not only are nurses accountable for tracking these patients, they also have a significant role to play in patient education. 20 The public continues to need training and reminders to wear a car seat belt, to avoid BAT. In addition, the public should be constantly reminded about the implications of driving while intoxicated or with sensory impairment. 21 The results of BAT have been enhanced over time. The results are good for patients with minor blunt trauma, but for those suffering from various organ injuries, in-hospital mortality can differ from 3% to 10%. The ready accessibility of CT also enabled physicians to monitor patients carefully, without unnecessary surgery. 22 The implementation of CT and sonography has made significant progress in the treatment of trauma. Although ultrasound equipment systems have enhanced resolution, 50% of acute abdominal wounds are missed. For more specificity, CT was used in blunt trauma. Sonography is mostly considered the best option in the case of an initial assessment of the blunt abdominal injury. However, sonography is favored for those positive and negative diagnostic patients to assess further organ damage. 23
Materials and Methods
This meta-analysis was conducted to look for the reliability of the FAST technique, in the evaluation of blunt torso trauma. All the studies that were included had information regarding the use of FAST technique. However, the studies related to animals were excluded during this review process. A search was completed with Google Scholar, PubMed, National Center for Biotechnology Information (NCBI), MEDLINE, and Medscape databases, from 1993 up to 2020. The key search terms used were reliability; FAST; ultrasound; trauma, abdominal injuries; sensitivity; and specificity. The reviewer independently screened the titles and abstracts of the relevant articles and full-text downloads to determine whether inclusion or exclusion criteria were met. Any disagreement was resolved through a consensus. Studies were eligible if they included information about FAST examination in the abdominal trauma. The research which was performed with animals was excluded from this review process. The eligible studies were first categorized, and then, analysis of the data was performed according to specific pathologic condition. This literature review retrieved studies’ sample size, application, sensitivity, and specificity of the ultrasound in the diagnosis of abdominal trauma. From all the data retrieved, descriptive statistics were gathered for analysis. A table was created, with predefined subgroups, for all variables included in the study (Table 2). The variables included were as follows: year of the study, the first author of the research article, country, sensitivity, specificity, sample size, disease, and journal name. The studies were included if complete information was provided for all the variables in a human study. The studies were excluded if incomplete information was given about the variables of the study.
Results
In total, 100 articles were identified through the database search. Besides, five articles were identified through other sources. Then, screening was performed, and ten articles were removed due to duplication. Further screening was performed for 95 articles, and 20 articles were excluded due to insufficient information. Sixty-five full-text articles were assessed for eligibility. There were 21 full-text articles excluded due to research performed on animals, and this study was determined as a review of only human studies. Forty-six studies were included that had a qualitative synthesis. I also included 46 quantitative syntheses (meta-analysis). The flow diagram depicts the flow of information through the different phases of a systematic review. It maps out the number of records identified, included and excluded, and the reasons for exclusions (see Figure 1).
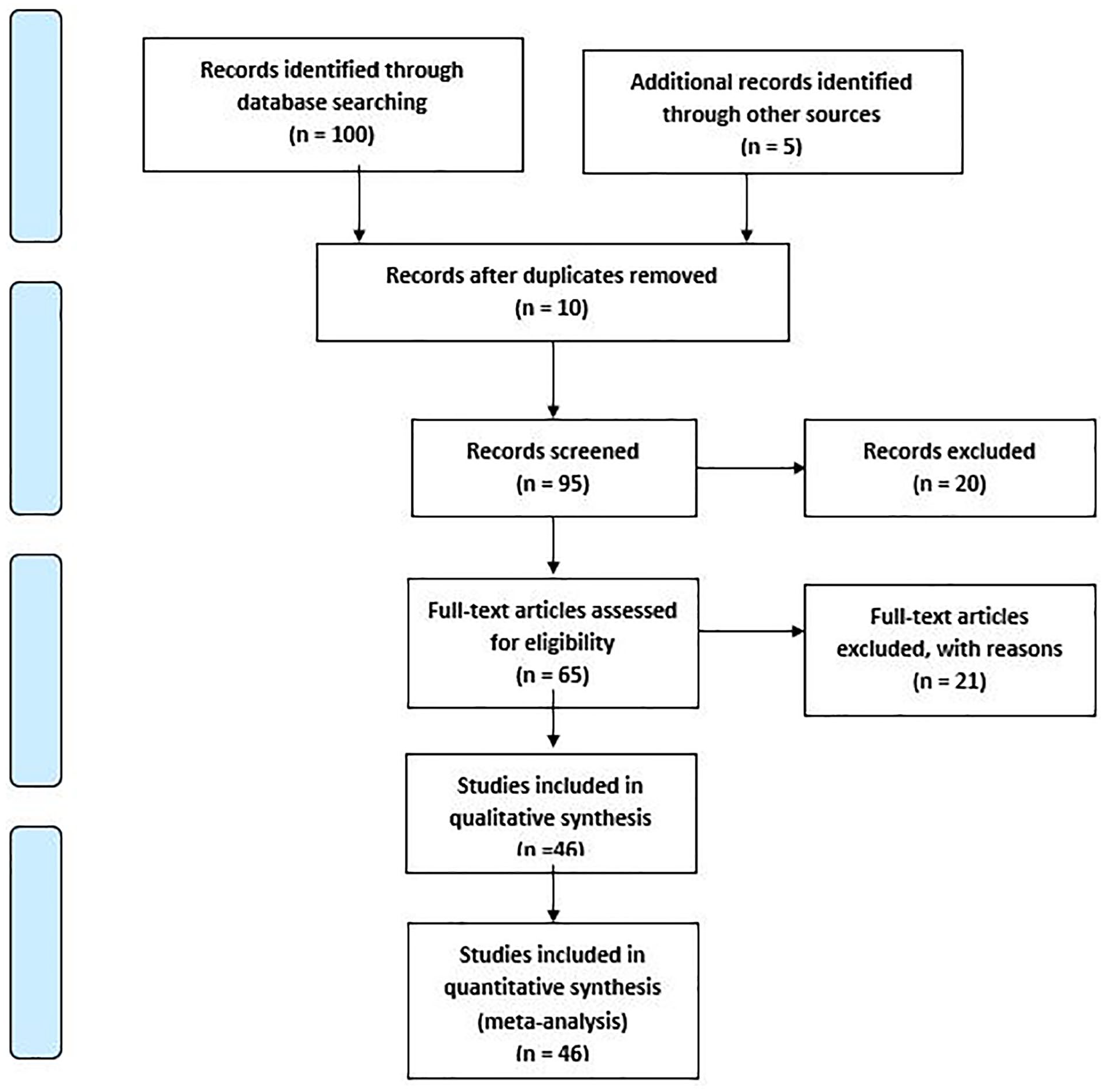
PRISMA 2009 flow diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
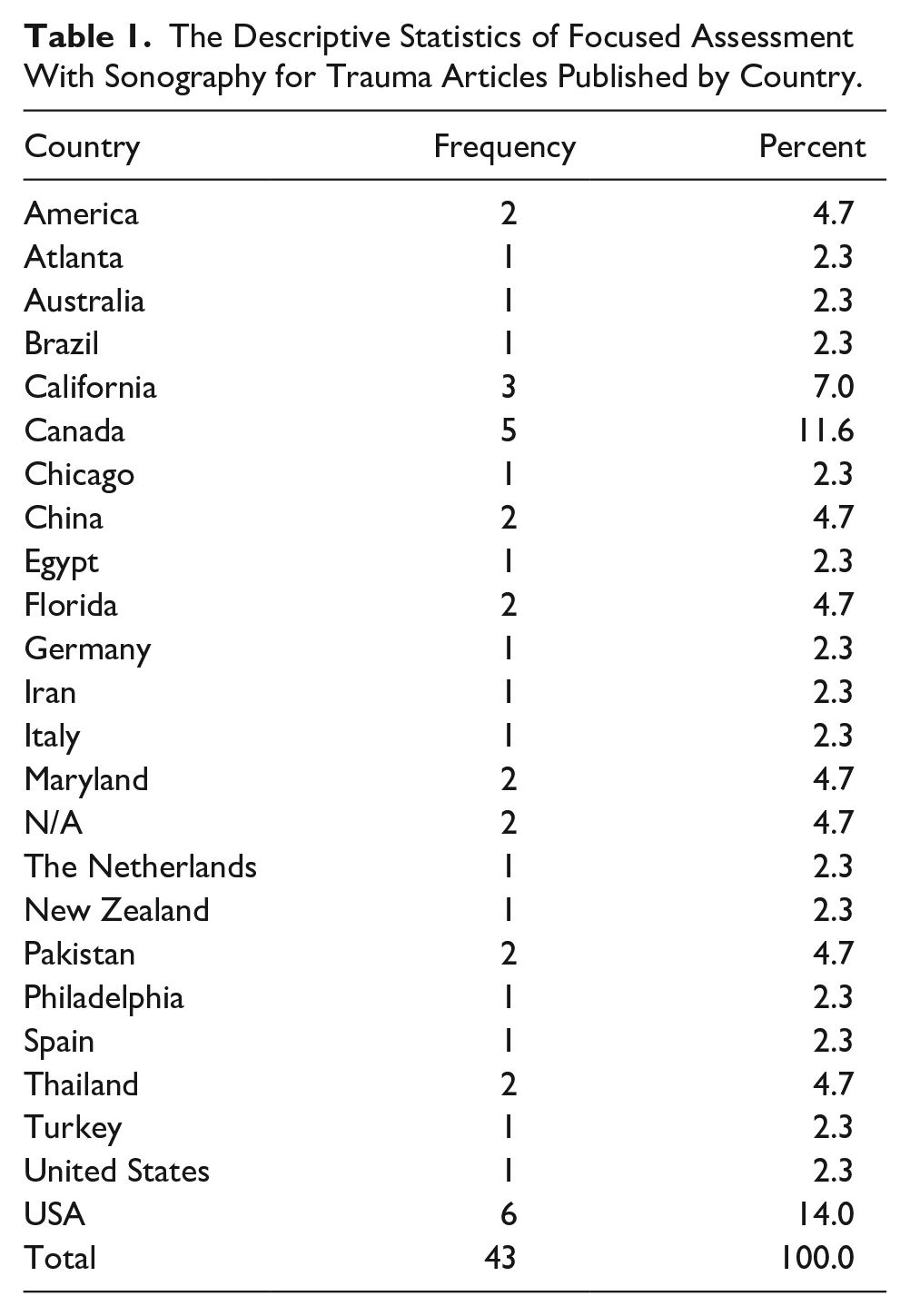
Based on this review, most of the research, performed on gouty arthritis, was conducted in the United States, and that was based on six articles included from the literature search. The remaining articles originated from Canada (N = 5), California (N = 3), America, China, Florida, Maryland, Pakistan, and Thailand (N = 2); in two articles, country was not mentioned, Atlanta, Australia, Brazil, Chicago, Egypt, Germany, Iran, Italy, the Netherlands, New Zealand, Philadelphia, Spain, Turkey, and the United States (N = 1) (Table 1, Figure 2).
The Descriptive Statistics of Focused Assessment With Sonography for Trauma Articles Published by Country.
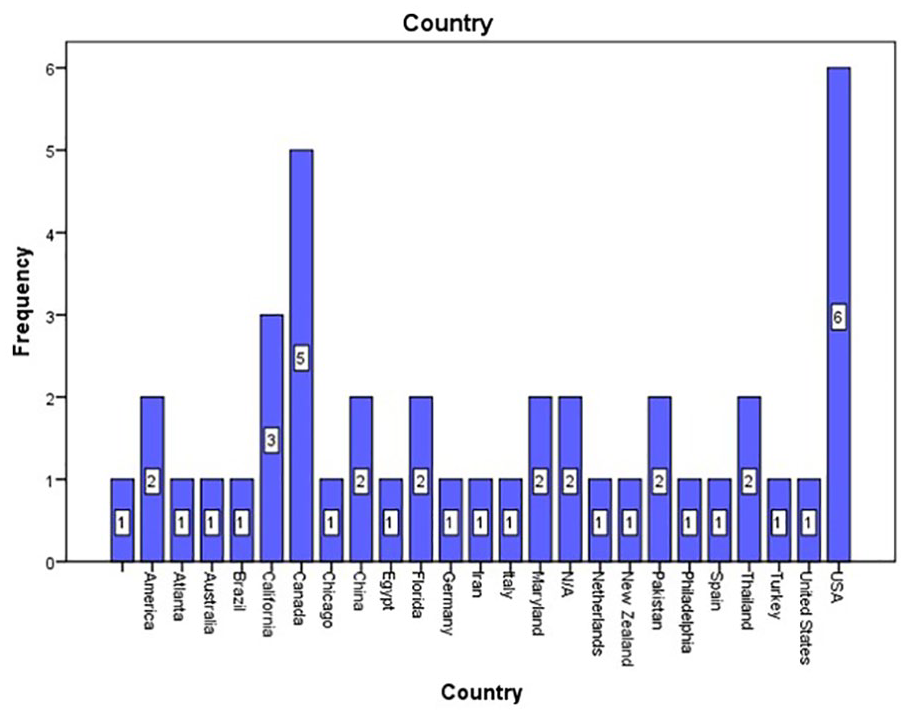
The countries where studies on focused assessment with sonography for trauma were completed.
The minimum sample size was 22 and the maximum sample size was 24 350 in the included articles. The duration of the articles that were included in this literature review was from 1993 to 2020. All patients affected by trauma were included in this research, including the adult and pediatric population both, who were all examined with the FAST technique (see Table 2).
The Variables That Were Pulled From the Systematic Review of the Literature.
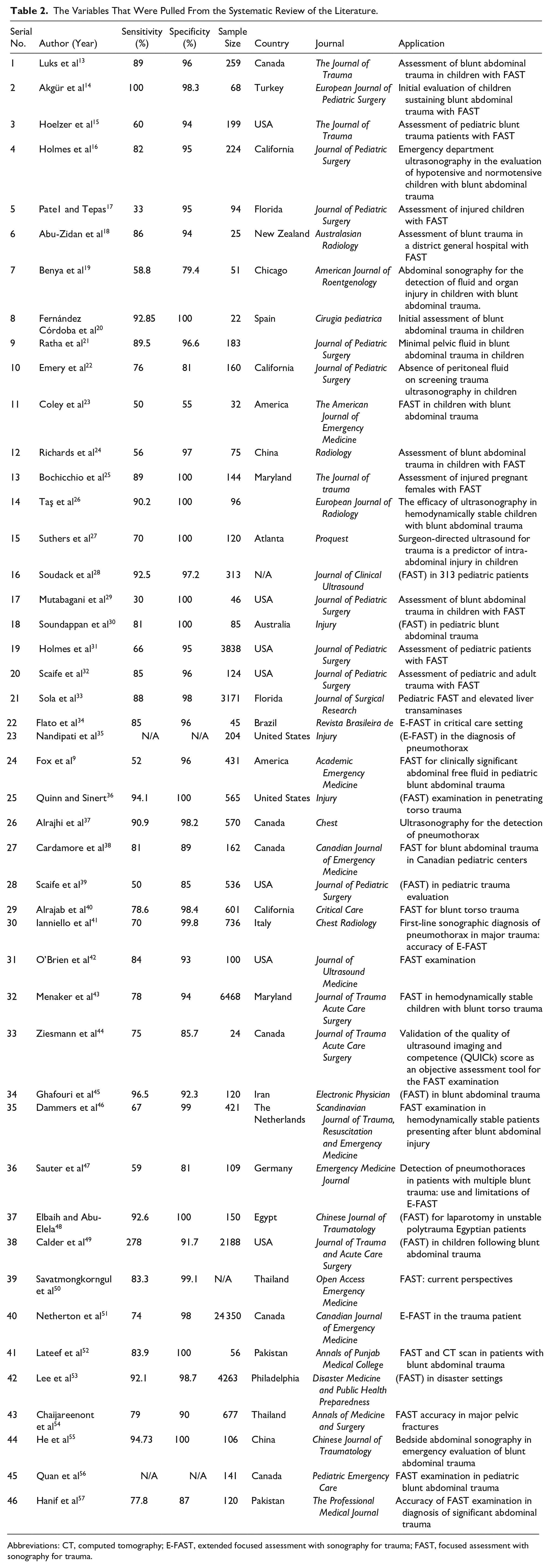
Abbreviations: CT, computed tomography; E-FAST, extended focused assessment with sonography for trauma; FAST, focused assessment with sonography for trauma.
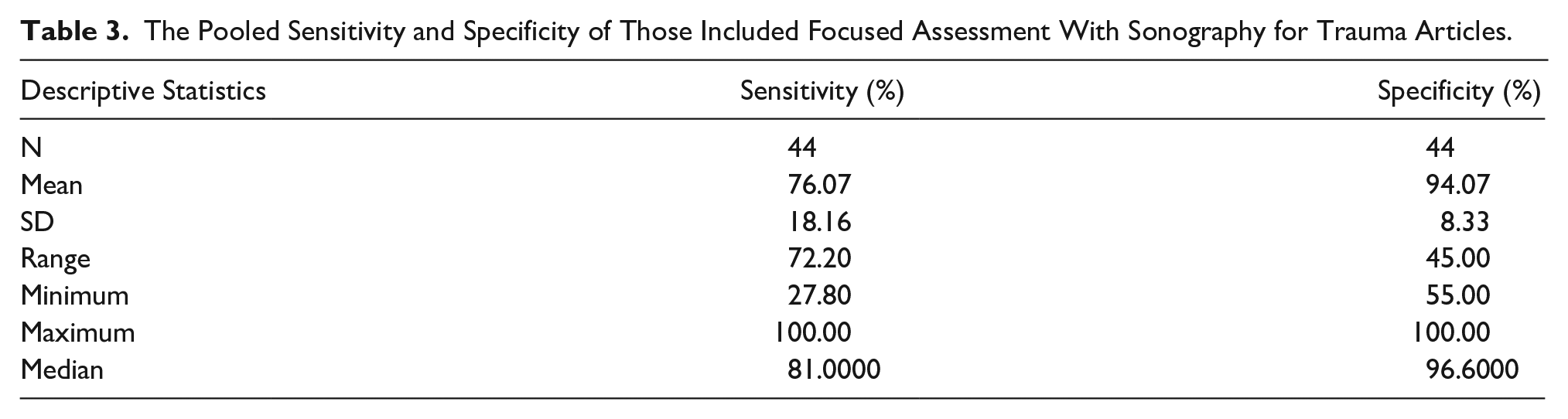
A total 46 studies were included in this review, and of these, only two studies did provide sensitivity and specificity. The mean sensitivity was 76.07% ± 18.16 SD with a range of 27%–100%, while the mean specificity was 94.07% ± 8.33 SD with a range of 55%–100% (Table 3).
The Pooled Sensitivity and Specificity of Those Included Focused Assessment With Sonography for Trauma Articles.
A forest plot was made to show the sensitivity and specificity of the included articles, and the pooled sensitivity and specificity are shown in Figure 3.
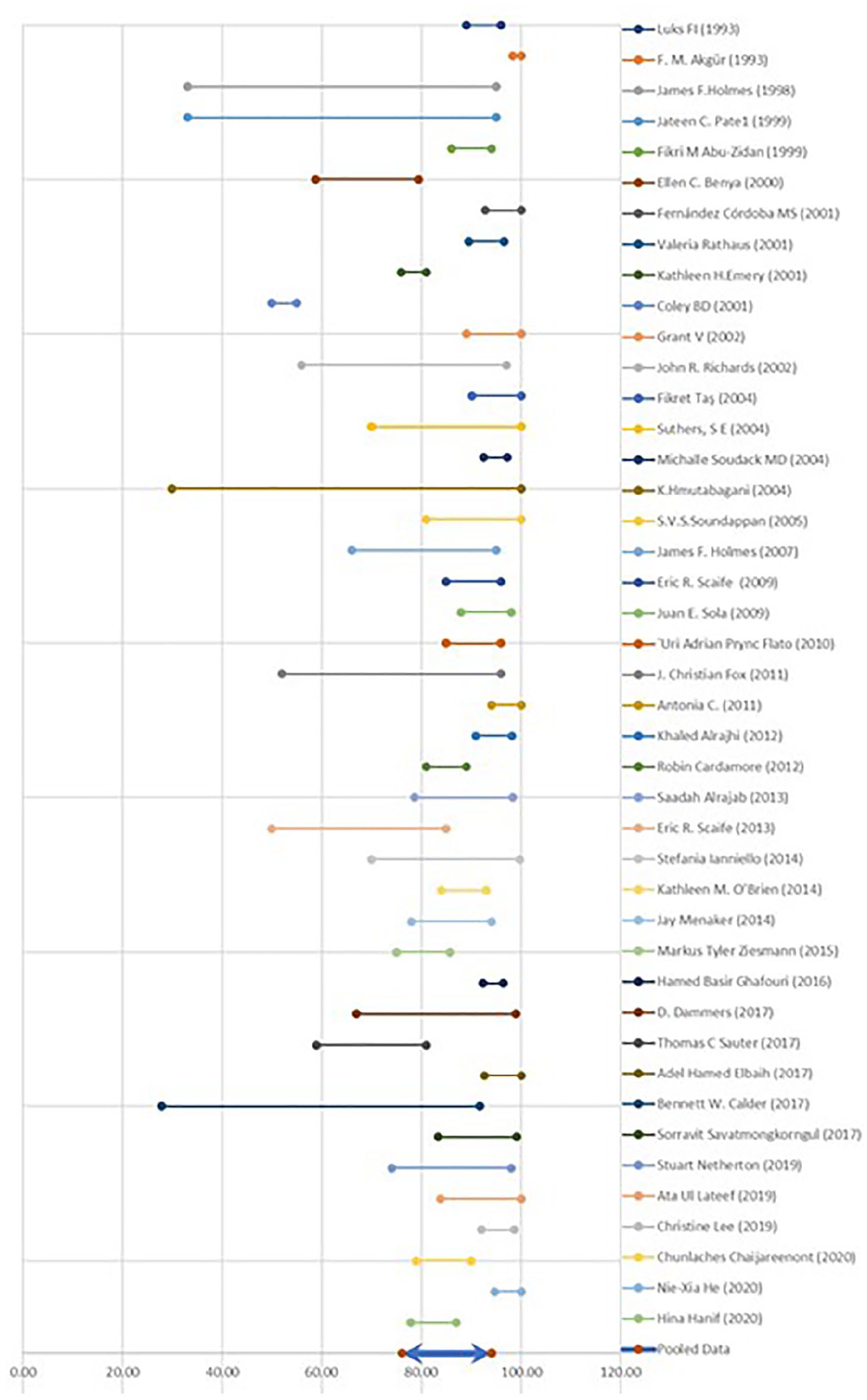
Forest plot.
Discussion
Abdominal traumas have been increasingly encountered as a health issue due to the extensive mobility of the population and its rapid pace of growth. 2 Trauma deaths result, on average, in 40 years of life lost and 18 years of productive life lost. 3 To determine the accuracy of the E-FAST technique, for torso trauma, a 2014 study was conducted. One hundred ninety-seven participants were recruited with a mean age of 27 years and standard deviation of 11 years. The overall ratio of male and female participants was 5:1. According to this ratio, it was observed that men are developing torso trauma more than 5 times compared with women. The ratio is considered more prevalent in men, as it is assumed that men are primary drivers compared with women. The specificity of E-FAST was 97%, sensitivity was 100%, NPV was 100%, and PPV was 87%. The completion time of an E-FAST examination was 5 minutes on average. 24
While pooling the results of all the 44 studies, the mean sensitivity was 76.07% ranging from 27% to 100%, while the specificity was 94.07% ranging from 55% to 100%. In simple words, it means that the patients whose ultrasound reports exclude the presence of torso trauma will have 94.07% accurate result. However, the positive declaration of torso trauma with ultrasound is 76.07% accurate, while the rest of the 23.93% could be missed. The missing of the torso trauma could be caused by multiple reasons. Because the sonographic appearance of blood is temporal and technique dependent, if there is fresh blood, that could appear slightly echogenic. And the differentiation of echogenic blood from the surrounding soft tissues is a bit tough and experience based. In emergency department, no more time could be given to patients to differentiate it. Although, this time consuming and sometimes series examinations are needed to diagnose it accurately. 25
The large range of sensitivity and specificity revealed that ultrasound is the operator-dependent quality of the machine in use. It is therefore needed for the operator to have in-depth knowledge of ultrasound machine operation (knobology) and various sonographic presentations of various diseases. However, free and fair accreditation bodies are needed for the prudent use of ultrasound, all around the world. All the sonologists are needed to be accredited with these organizations. 26 To know the accreditation status of sonologists, currently working in the sonology department, a national survey was performed through a literature review. According to the survey, admins of the sonology departments and accreditation of the ultrasound centers were intereogated. 27 The survey results showed that 12% of the sonologists had no sonography-related credentials. The primary age range of this group was less than 34 years. About 64% had a 2-year degree in allied health education program other than ultrasound. However, 42% of the sonography laboratories were not accredited. 11 To obtain the accreditation, credentialing, and quality improvement, a literature review was conducted. In the field of sonography, a few accreditation organizations and scarce credentials of sonologists were seen. Although, it is well established and known that the quality of examination and resultant diagnosis is based on the sonologist (operator dependent). Nineteen research studies on accreditation, credentialing, and quality improvement were included in a review. 28 A huge difference in facilitating accreditation status based on sonography specialty and geographical area. Positive correlation between improvement in the sonographic imaging and accreditations was seen. It was concluded that accreditation is the soul of best fruitful sonography. The main concern of a number of articles was about the unsatisfactory quality of ultrasound performed in nonaccredited centers by unaccredited personals. If accreditation, and guidelines and accreditation examinations are implemented nationwide in medical diagnosis, it may lead to increased quality within the field. 12
Apart from that, continuous medical education is especially important in this fast growing department. Every day, some new innovations, modifications, and advances are being introduced in the ultrasound modalities. It is difficult for a conventional sonologist to operate latest state-of-the-art ultrasound machines. 29 A review of the literature was performed in 2010 to look for the importance of continuous medical education for the physician working in the outreach rural areas. However, robust evidence demands for the need of continuous medical education of physicians serving in rural areas 30 to promote advanced procedural skills training and other skill-improving areas such as uses of different machines like ultrasound in medicine. Distant learning system had been supposed to be helpful in the process of improving access to continuous medical education. 31 The effect of continuous medical education is evident in supporting for the best health delivery system. 13 To know the effect and importance of continuing medical education for smooth health delivery system, a study was conducted. A questionnaire included basic questions regarding basic information that was filled by 160 participants in the class of continuing medical education. It was concluded that continuing medical education is very important for the professional of ultrasound in medicine to improve their career in the field. 14
Owing to the immense development in ultrasound modalities, no longer, ultrasound remains an office-based instrument; rather, it is now a vast field and isolated specialty as sonology. It is a deeming need of the day to deal sonology as an independent speciality. 32 Apparently, it looks difficult for individuals to well-equip themselves with the knowledge of sonology along with other radiation-based modalities. To look for the interest of students in ultrasound education in medical schools, a literature review was conducted. 33 It was seen that the interest of students in ultrasound has increased dramatically in recent years. It was seen that students had learnt ultrasound well and had embraced it as an important component of their education and future practice of medicine. An international consensus conference on ultrasound education is recommended to help define the essential elements of ultrasound education globally to ensure ultrasound is taught and ultimately practiced to its full potential. 34 Ultrasound has the potential to fundamentally change how we teach and practice medicine to the benefit of learners and patients across the globe. 15 Ultrasound waves are used in sonology to depict body structures, while radiology is an electromagnetic radiation–based modality. 16 There is a great deal of difference between the ultrasound image and the image generated by radiation. Gases in the body appear bright echogenic in ultrasound images, while black in the radiation-based images. 17
Conclusion
Besides, different ultrasound equipment systems yield different diagnostic results. Conversely, with the advent of time, the quality of ultrasound machines is being degraded. 35 Comparatively, there is a significant difference between conventional older ultrasound equipment systems and more modern machines. In the developing world, physicians are either working with their conventional machines or importing older units, as well as refurbished machines, from developed countries. 9 There is a great deal of difference between old conventional ultrasound imaging device and modern ultrasound unit. The conventional ultrasound devices were larger and awkward; moreover, initially, there was only gray-scale imaging facility in them. 36 However, with continuous refinement made, it is one of the most important and valuable devices in medical imaging. 18 The older devices were undoubtedly relatively low paced, but the pooling of data regarding reliability of the FAST technique revealed that the studies conducted while using those conventional modalities had very worse results. 37 Modern modalities, on the other hand, are equipped with high-resolution transducers, 3D and 4D imaging, and elastography, as well as some algorithm-based software, which have made it important in medical imaging, and the medical profession today seems lacking without it. 19 The current review proved that the reliability of the FAST technique has dramatically improved with innovations in ultrasound equipment systems. 38 It was concluded that the FAST technique has high sensitivity and specificity in the diagnosis of BAT. 39 However, a large range of sensitivity and specificity of the FAST technique, in the evaluation of torso trauma, reveal that sonography is operator, technique, and equipment dependent. 40 So, to overcome these limitations, operator training and education should be improved as well as the use of modern ultrasound equipment systems is needed, to properly evaluate disease. Additional research on the use of the FAST technique for torso trauma, while using modern ultrasound equipment systems, is needed. 41
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.