
Abstract
Background:
Ultrasound training is an essential part of residency programs during emergency medicine rotations for first-year trainees (postgraduate year 1). The Focused Assessment with Sonography for Trauma examination used to assess for internal bleeding in trauma patients is one of the essential skills postgraduate year 1 residents must acquire during the emergency medicine rotation.
Method:
A prospective, longitudinal, observational study of postgraduate year 1 residents during a 2-month long emergency medicine rotation conducted from 1 April 2019 to 31 May 2021. The primary outcome was the mean difference between the hands-on Focused Assessment with Sonography for Trauma examination scores of the first week of the emergency medicine rotation and the same hands-on Focused Assessment with Sonography for Trauma examination scores of the last week of the emergency medicine rotation. All postgraduate year 1 residents had open access to the ultrasound machine to practice examining on other postgraduate year 1 residents or could use it on real patients under supervision of emergency medicine physicians.
Result:
A total of 91 postgraduate year 1 residents (65 male and 26 female) were recruited and submitted to the hands-on Focused Assessment with Sonography for Trauma test in both the first and last weeks of the rotation. The mean test score for the postgraduate year 1 residents in the first week was 7.81 (standard deviation = 2.11). The mean test score in the last week was 16.17 (standard deviation = 2.60). The primary outcome of this study was the score difference between the first and last weeks (mean = 8.35, 95% confidence interval = 7.73 to 8.94, p < 0.001, paired t-test).
Conclusion:
Hands-on practical Focused Assessment with Sonography for Trauma training for postgraduate year 1 residents during emergency medicine rotations significantly improved their Focused Assessment with Sonography for Trauma test scores.
Keywords
Background
Ultrasound training is an essential part of residency programs during emergency medicine (EM) rotations for first-year trainees (postgraduate year 1 (PGY1)). 1 The Focused Assessment with Sonography for Trauma (FAST) examination used to assess for internal bleeding in trauma patients is one of the essential skills all PGY1 residents must learn during their EM rotation due to its relative rapidity and noninvasiveness.2,3
Although FAST training should be a component of the medical school curriculum, 4 the majority of PGY1 residents do not receive formal training in ultrasound examinations. In Japan, all physicians are mandated to complete 2 years of accredited postgraduate clinical training since 2004 with rotations in major clinical specialties, including EM, internal medicine, pediatrics, surgery, and community-based practice. 5 The duration of the EM rotation is set at the discretion of each hospital. The EM rotation of our institution is 2 months, and is mandatory for PGY1 residents.
There are multiple factors that may influence a resident’s opportunity to gain experience with FAST training in real-time emergency department (ED) setting, including seasonal patient volume fluctuation, the actual pace of emergent care, and the number of PGY1 residents in a given rotation. Given these barriers, it is not uncommon for PGY1 residents to complete an EM rotation without acquiring adequate experience with real patients. Therefore, we offered PGY1 residents unlimited opportunity to use the ultrasound machine during their rotation for practice purpose. The EM rotation provides an excellent opportunity for FAST training.6,7 The purpose of this study was to assess the effectiveness of live patient-based FAST training for PGY1 residents within an established EM rotation.
Methods
A prospective, longitudinal, observational study of PGY1 residents during EM rotations conducted from 1 April 2019 to 31 May 2021 (fiscal year 2019–2020) was performed. Each rotation lasted 2 months. The first hands-on FAST examination was administered without prior lectures, so that PGY1 residents would perform the FAST using the skill and knowledge they had learned in medical school. After the first test, all participating PGY1 residents were given a standardized list of key assessment parameters both verbally and instructed interactively to ensure consistency in the teaching points in the first week of the rotation. Although simulation-based training showed better performance than training without simulation in diagnostic ultrasound scanning on real patients, 8 PGY1 residents used the ultrasound machine for real patients only.
The ultrasound machine used in the emergency room was a GE LOGIQ E9 XDclear 2.0 ultrasound machine (GE Healthcare, Wauwatosa, WI, USA), and the PGY1 residents could use the machine on real patients under the supervision of attending EM physicians or on other PGY1 residents freely without supervision. Supervised FAST exams were interactive in nature that allow immediate feedback. If PGY1 residents had trouble displaying appropriate image or placed probe in inappropriate position or angle, attending EM physician corrected them as error occurred. The instructor recorded all scoring in real time. This study was conducted at an academic university hospital and received approval from the Institutional Review Board (2767) with written, informed consents obtained from all participants.
Participants
The participants were first-year rotating residents (PGY1) (n = 91) in the EM rotation at an academic university hospital during 2019–2020 fiscal year. Table 1 lists the identified specialty of interest at the time of the rotation of the PGY1 residents. They were divided into three groups: (1) Internal Medicine Group, (2) Surgery Group, and (3) Others Group. The Internal Medicine Group included cardiology, gastroenterology, respiratory medicine, nephrology, neurology, hematology, and rheumatology. The Surgery Group included cardiovascular surgery, thoracic surgery, gastroenterological surgery, breast and endocrine surgery, orthopedic surgery, neurosurgery, obstetrics and gynecology, urology, and EM. The Others Group included pediatrics, anesthesiology, ophthalmology, otorhinolaryngology, dermatology, plastic surgery, radiology, and psychiatry.
Demographic characteristics of the postgraduate year 1 residents.
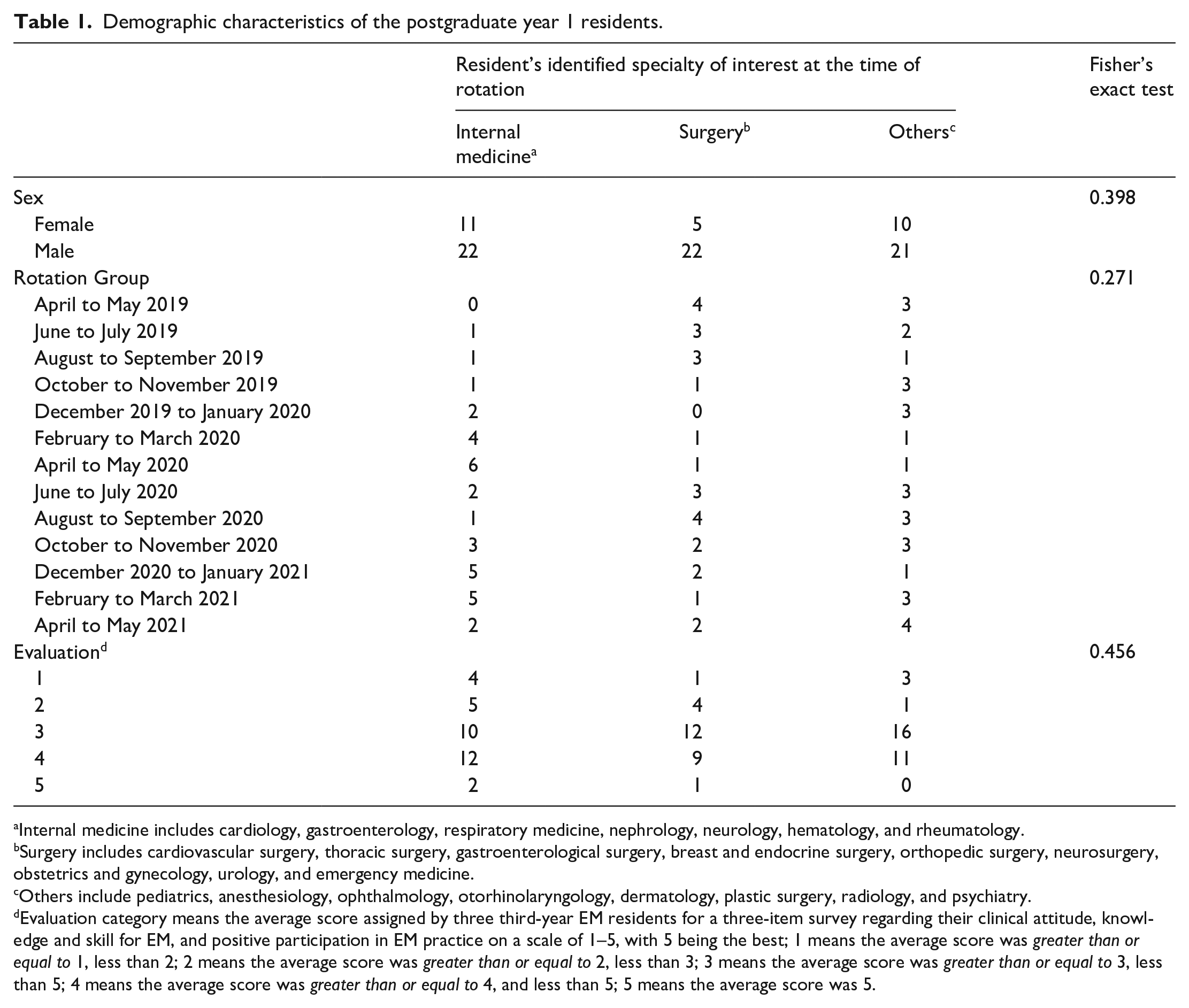
Internal medicine includes cardiology, gastroenterology, respiratory medicine, nephrology, neurology, hematology, and rheumatology.
Surgery includes cardiovascular surgery, thoracic surgery, gastroenterological surgery, breast and endocrine surgery, orthopedic surgery, neurosurgery, obstetrics and gynecology, urology, and emergency medicine.
Others include pediatrics, anesthesiology, ophthalmology, otorhinolaryngology, dermatology, plastic surgery, radiology, and psychiatry.
Evaluation category means the average score assigned by three third-year EM residents for a three-item survey regarding their clinical attitude, knowledge and skill for EM, and positive participation in EM practice on a scale of 1–5, with 5 being the best; 1 means the average score was greater than or equal to 1, less than 2; 2 means the average score was greater than or equal to 2, less than 3; 3 means the average score was greater than or equal to 3, less than 5; 4 means the average score was greater than or equal to 4, and less than 5; 5 means the average score was 5.
To preserve consistency and reproducibility, the simulated patient was the same in both the first and last weeks of the rotation, which reduces the bias due to individual anatomical differences. A healthy human model can provide good interpretation of normal anatomical landmarks, but this model does not provide abnormal findings. 9 A letter of information was provided to PGY1 residents, which included the elements of informed consent.
Assessment
An 18-item, hands-on performance check list (total score = 21) was developed to assess medical students’ skills on the FAST exam (Figure 1). 10 The items and content on the test had been used previously and the copyright holder permitted us to use the score sheet. 10 The test was administered to PGY1 residents individually in the first and last weeks of the EM rotation under the supervision of the principal investigator. The test was conducted individually in a separate room without any cue from the proctor (principal investigator), and other PGY1 residents were not allowed to observe the testing or contact the PGY1 resident that had just completed the test to prevent perceived advantage. During the second FAST performance test at the last week of the rotation, PGY1 residents were asked to recall the total number of hands-on FAST exams each has performed during their EM rotation. Participation by PGY1 residents was voluntary and did not impact their academic status within the program. After finishing 2 months of the EM rotation, each PGY1 resident was assessed by three Third-Year EM residents (PGY3) using a three-item survey to gauge their Clinical Attitude, Knowledge, and Skills for EM, and Positive Participation in EM practice on a scale of 1–5, with 5 being the highest.11,12 Clinical Attitude assessed professionalism, and was evaluated based on PGY1 resident’s regular interaction with the patient, wearing appropriate attire, and showing respect for the patient. Knowledge and Skills were evaluated based on display of medical knowledge and competency of critical skills such as venipuncture during cardiac arrest. And Positive Participation in EM was assessing teamwork attribute as it evaluated not only PGY1’s performance of EM tasks but also participation in other clinical practice such as helping PGY3 residents. 13 The survey results are presented in Tables 1 and 2.

Focused Assessment with Sonography for Trauma score sheet.
Test results and evaluation of the postgraduate year 1 residents.

CI: confidence interval.
Evaluation means that each PGY1 was assessed by three third-year EM residents (PGY3) with a three-item survey regarding their clinical attitude, knowledge, and skill for EM, and positive participation in EM practice on a scale of 1–5, with 5 being the best.
Statistical analysis
The primary outcome was the mean difference between the hands-on FAST examination scores of the first week of the EM rotation and the same hands-on FAST examination scores of the last week of the EM rotation. The subgroup analysis included factors affecting the change in the score using simple and multiple linear regression analyses. The same instructor and simulated patient were used for both hands-on performance tests of the study.
Values were reported as mean values and standard deviation (SD) for continuous variables, and as frequencies with percentages for categorical variables. Fisher’s exact test was used for categorical variables. For the primary analysis, a paired t-test was used to examine differences in the hands-on FAST examination scores between the first week and the last week of the rotation. A subgroup analysis according to the three groups of the Identified Specialty of Interest at the time of the EM rotation of the PGY1 residents was performed, and the differences in the hands-on FAST examination scores were compared among the identified specialties of interest with multiplicity adjustment using Dunnett’s Method. The relative effects of baseline characteristics (Subphrenic Space Identified on the Left Side, Correct Probe Orientation on the Right Side, and the Identified Specialty of Interest) on differences in the hands-on FAST examination scores over the 2 months were examined using a simple and multiple linear regression models. The potential influence by group and number of hands-on FAST examinations performed during EM rotation were also examined using multiple linear regression models.
All tests were two-tailed, with p < 0.05 considered significant. All analyses were performed with STATA (version 16.1; Stata Corp., College Station, TX, USA).
Results
A total of 91 PGY1 residents (65 male and 26 female) were recruited, and 90 residents (64 male and 26 female) completed the hands-on FAST test in both the first and last weeks of the rotation (Table 1). One participant was lost to follow-up due to missing last week FAST test. There were no significant differences in residents’ identified specialties by sex, group, and evaluation (p = 0.398, p = 0.271, and p = 0.456, respectively, Fisher’s exact test; Table 1). All PGY1 residents knew FAST, but the great majority have not performed FAST exam during medical school or before EM rotation, and only two PGY1 residents have performed FAST exam twice prior to joining EM rotation.
The mean test score for the PGY1 residents in the first week was 7.81 (SD = 2.11). The mean test score in the last week was 16.17 (SD = 2.60). The primary outcome of this study was the score difference between the first and last weeks (mean = 8.35, 95% confidence interval (CI) = 7.73 to 8.94, p < 0.001, paired t-test).
The subgroup analysis by Identified Specialty of Interest at the time of the EM rotation showed there was no significant difference among the three groups in the FAST test results at the first week and the last week (Table 2 and Figure 2).

Violin plot of FAST score for each resident’s identified specialty of interest at the time of rotation.
Simple linear regression analysis showed that two items of the first week “Correct Probe Orientation (indicator in cephalad direction) on the Right Side” and “Correct Probe Orientation (indicator in cephalad direction) on the Left Side” were inversely correlated with the primary outcome (beta coefficient (BC) = −2.10, 95% CI = −3.49 to −0.71, p = 0.003 and BC = −1.62, 95% CI = −3.07 to −0.18, p = 0.028, respectively). However, the same items in the last week were not predictive. Simple linear regression analysis also showed that two items in the last week “Splenorenal Recess Identified” and “Subphrenic Space Identified” were positive predictive factors for the primary outcome (BC = 4.12, 95% CI = 2.69 to 5.55, p < 0.001 and BC = 3.07, 95% CI = 1.62 to 4.51, p < 0.001, respectively), but the same items in the first week were not predictive.
Evaluation by PGY3 residents also confirmed positive predictive factor for the primary outcome (BC = 0.85, 95% CI = 0.24 to 1.47, p = 0.007), but the number of hands-on FAST exams performed during EM rotation was not related to the primary outcome (BC = 0.11, 95% CI = −0.03 to 0.25, p = 0.115). The results of multiple linear regression analysis are provided in Table 3. “Correct Probe Orientation (indicator in cephalad direction) on the Right Side” in the first week and “Subphrenic Space Identification” in the last week were good prognostic factors for the primary outcome. Insofar as the timing of EM rotation, with respect to the Lowest Score Group (October to November 2019), the Highest Score Group (February to March 2020) demonstrated significantly higher association with the primary outcome (BC = 3.92, 95% CI = 0.73 to 7.11, p = 0.017); however, the number of hands-on FAST exams performed during EM rotation was not associated with the primary outcome (BC = 0.04, 95% CI = −0.10 to 0.18, p = 0.545).
Results of multiple linear regression analysis.

FAST: Focused Assessment with Sonography for Trauma.
“Subphrenic Space Identified on the Left Side” was performed in the last week. “Correct Probe Orientation (indicator toward head) on the Right Side” was performed in the first week.
Discussion
Hands-on practical FAST training for PGY1 residents improved their FAST test scores significantly during their 2-month long EM rotation. The average score of each rotation group was nearly identical; however, the highest score group achieved significantly higher primary outcome than the lowest group. Paradoxically, the number of hands-on FAST exams performed during EM rotation was not associated with the primary outcome. Some PGY1 residents tried to prepare for the last week performance test even though they had not performed any hands-on FAST exam during EM rotation. To discourage this potential scenario, we emphasized FAST test scores would have no impact on PGY1 residents’ academic status within the program, and participation by PGY1 residents was entirely voluntary. Timing of EM rotation group seemed to affect the FAST test score (Table 3 and Figure 3). The 2-year mandatory postgraduate clinical training traditionally starts in April; thus, February to March groups tended to achieve better scores than the earlier EM rotation groups because those PGY1 residents were more accustomed to practice in the emergency room setting with accrued clinical experience, and could use the ultrasound machine more confidently in February and March (end of academic year). The Identified Specialty of Interest at the time of the rotation by the PGY1 residents might also affect the FAST test score. The PGY1 residents who chose internal medicine as their specialty tended to have slightly better scores than the other two specialty groups, although the difference was not significant. It was not possible to determine the reason why PGY1 residents of the Surgery Group were not superior to the other two groups, even though the surgical residents were expected to learn FAST. 14 One of the reasons might be that our hospital only accepted a small number of trauma patients.

Violin plot of FAST score for each EM rotation group.
Simple and multiple linear regression analysis showed that two items (Correct Probe Orientation (indicator in cephalad direction) on the Right and Left Sides) in the first week were inversely correlated with the primary outcome. PGY1 residents who could perform Correct Probe Orientation (indicator in cephalad direction) bilaterally tended to show high scores in the first week, and, thus, they could not improve their score in the last week. For the same reason, two items (Splenorenal Recess Identification and Subphrenic Space Identification) in the last week were difficult to perform, and these positions were the key for a high score. Thus, some PGY1 residents who could not perform correct probe positioning in the first week could eventually perform both Splenorenal Recess Identification and Subphrenic Space Identification showed higher scores. Multiple linear regression analysis showed that PGY1 residents who failed “Correct Probe Orientation (indicator in cephalad direction) on the Right Side” in the first week, who could perform “Subphrenic Space Identification” in the last week tended to have a higher primary outcome (Table 3). EM physicians should consider that the left side of the patient is more difficult when performing FAST exam for PGY1 residents.
This study has several limitations. First, the Identified Specialty of Interest at the time of EM rotation of the PGY1 residents was divided arbitrarily into three groups. Surgical specialties in our category have more opportunity to see trauma patients in the emergency room, whereas Internal Medicine and Others do not to see trauma patients, and Internal Medicine physicians utilize ultrasound more often in their basic practice; therefore, we believe these classifications were reasonable. Second, the number of PGY1 residents was small, especially the number of female residents; thus, sex was not considered as a predictor of FAST performance. Third, all PGY1 residents had advanced notice they would take the second test in the last week of their rotation; therefore, some residents might have practiced FAST just before the test, which might have affected their scores. Some residents whose second test scores were higher than average failed to perform FAST adequately for real trauma patients after their EM rotation; therefore, additional FAST performance evaluation of PGY1 residents should be implemented after the EM rotation to ascertain their true competency. Fourth, practical training was not standardized and the bias of different approaches of the residents might have contributed to variance. Our goal in this study is to assess the effectiveness of live patient-based unstandardized practical training for PGY1 residents; therefore, this bias was thought to be acceptable. Fifth, this study was an observational study in design; therefore, sample size was not calculated. Finally, recall bias of accurate total number of hands-on FAST exam was inevitable. Hence, we asked other PGY residents to confirm their total number of hands-on FAST exams.
Conclusion
In conclusion, practical FAST training for PGY1 residents during the EM rotation significantly improved their FAST test scores. PGY1 residents should learn and become facile with FAST exam during the EM rotation with attention paid to acquire proficiency scanning patients’ left side since it is technically more-challenging side.
Footnotes
Author contributions
K.Ob. and Y.I. contributed to the analysis and interpretation of data, and assisted in the preparation of the article. Ko.O., J.C., Ka.O., and A.T. wrote and revised the article. All authors have read and approved the article.
Availability of data and material
The data sets used and/or analyzed during this study available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval and consent to participate
The research was approved and consent to participate was obtained by the Institutional Review Board at Osaka Medical College (no. 2767).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from all subjects before the study.