
Abstract
Objective:
Acute common iliac artery occlusion which results from blunt abdominal trauma is rare and potentially leads to a late diagnosis.
Methods:
We report a case of a 58-year-old patient who suffered a late diagnosed acute left common iliac artery occlusion secondary to abdominal trauma. An emergency exploratory laparotomy was performed to stop intra-abdominal bleeding, while his left limb ischemia was not noticed until 32 h later and femorofemoral bypass was then successfully performed for revascularization. Compartment syndrome was observed postoperatively, and fasciotomy was performed promptly. The wound was temporarily covered with Vaccum Sealing Drainage due to high skin tension. Patient underwent skin-grafting after leg swelling subsided.
Results:
The follow-up turned out that these managements were valid in the preservation of the limb viability.
Conclusions:
This case highlights the prudent recognition of the acute lower extremity ischemia in the abdominal trauma and immediate remedy for acute iliac artery occlusion after a late diagnosis.
Introduction
Acute common iliac artery occlusion after blunt abdominal trauma is rare and potentially leads to a late diagnosis at an early stage, especially when accompanied by acute abdominal manifestations. The surgeons may incautiously neglect the ischemic limb until it is limb-threatening, and amputation unfortunately becomes the final choice. In spite of the low incidence (ranges from 0.1% to 7.1%), caution should be taken to prevent limb loss in the event of the possibility of iliac artery occlusion when a patient sustains an abdominal trauma. 1 The abdominal trauma may be accompanied by intimal damage to the vessel, which perhaps results in the development of thrombosis. 2 It is crucial to be aware of the ischemic process early and avert a missed diagnosis. Our case is based on a patient who suffered a missed diagnosed acute left common iliac artery occlusion secondary to abdominal trauma, and successful remedy was given to preserve the viability of the limb.
Case report
A 58-year-old man without any medical history got hit by his handcart and was admitted into a local hospital, complaining of persistent sharp pain in the lower abdomen and mild pain in the left leg. His physical examination revealed significant lower abdominal tenderness, and the ultrasonic examination showed a large collection of abdominal fluid. Furthermore, the blood from abdominal paracentesis demonstrated intra-abdominal hemorrhage. The left femoral pulse and the distal pulses were palpable, with no further attention paid to the left lower limb. An emergency exploratory laparotomy under combined spinal and epidural anesthesia was performed. About 1450 mL blood was sucked from the abdomen and the mesentery of the ileum where the bleeding was located. Hemostasis was achieved with suturing and ligation. After the surgery, the patient felt numbness and coolness below the level of his left knee, but the surgeon thought it was due to the effect of the anesthesia and no pulse examination was performed.
The patient was transferred to our unit after 32 h from the accident and presented with severe numbness and impaired motor function of the left lower limb. The complete examination of his leg showed the absence of the left femoral pulse and the distal pulses, together with calf muscle weakness and diminished sensation of the entire foot. Subsequently, computed tomography (CT) angiogram revealed that the left common iliac artery was occluded (Figure 1). This patient was immediately sent to the operation room. A femorofemoral artery bypass was established at the common iliac artery. The postoperative physical examination revealed a palpable pulse and warm skin. Postoperative Doppler ultrasound demonstrated the presence of blood flow.
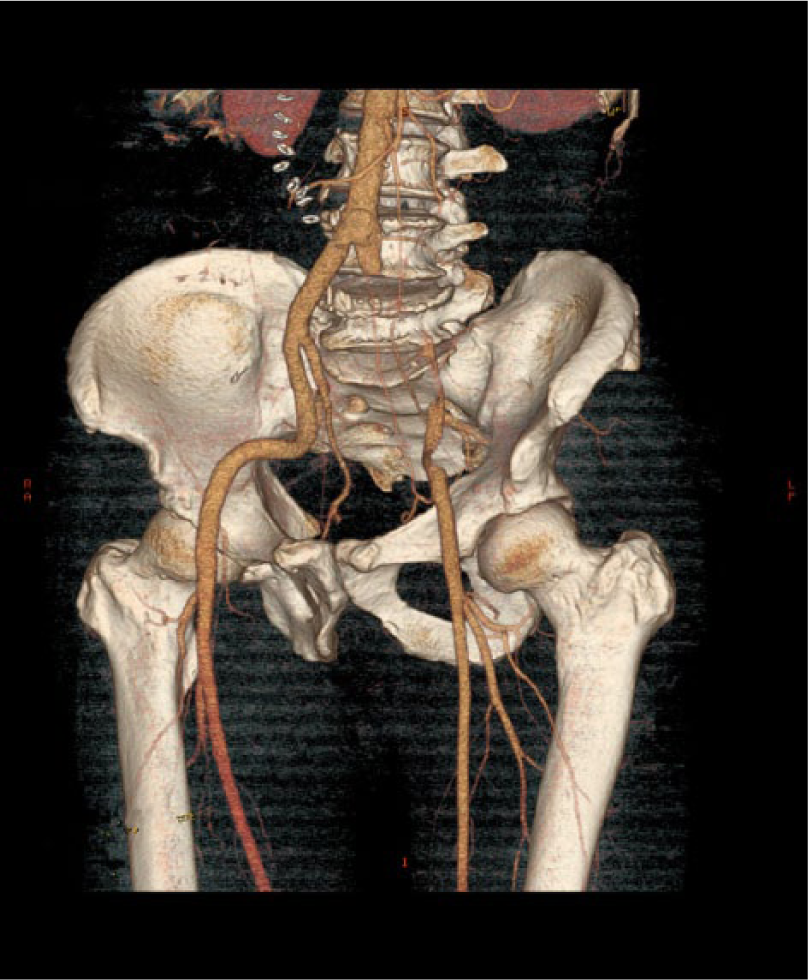
Three-dimensional computed tomography angiographic reconstruction confirms the occlusions of the left common iliac artery.
Unfortunately, severe pain and significantly progressive swelling occurred on the second day after revascularization. Characteristically, the calf was tender to palpation and pain increased with passive motion at the ankle. Compartment syndrome caused by the ischemia-reperfusion injury was diagnosed, and the four-compartment fasciotomy of the calf was performed for decompression. Wound closure was delayed, and the wound was temporarily covered with vacuum sealing drainage (VSD) because of high skin tension. The wound was then managed with skin-graft from the lateral thigh 10 days later after leg swelling subsided; 3-month follow-up showed ambulatory function with braces and the progressive wound healing, despite the weakness in dorsiflexion and numbness in the first dorsal web space due to a probable peroneal nerve damage. After 6 months, the patient could walk independently, and improved sensation in the leg was achieved. The patient gave informed consent for the information and image included in this report, which was also approved by the Institutional Review Board of The First Affiliated Hospital of Wenzhou Medical University.
Discussion
The common iliac artery injury from blunt abdominal trauma is rarely encountered by the surgeons due to the anatomical position within the protective pelvic girdle, but it is associated with a high rate of overall complications and even mortality.3–5 The most common mechanism associated with blunt trauma to the common iliac artery is the external compressive forces to the lower abdomen, which may subsequently result in intimal damage and lead to acute thrombosis of arterial lumen, 6 as is in our case. A high index of suspicion for iliac artery injury must be maintained in blunt abdominal trauma especially when the associated orthopedic injury is absent. This is because a clinical diagnosis of iliac artery injury is easily ruled out when abdominal symptoms are dominant. The thrombosis may initially be formed at the site of injury asymptomatically; however, it potentially leads to a dramatically sudden occlusion and can even precipitate limb-threatening ischemia. Therefore, blunt iliac artery injury may be a diagnostic challenge, as some of these injuries have normal pulses and mild presentations initially. 7
Evaluation of acute limb ischemia begins with obtaining an accurate patient history and a complete vascular examination. A CT angiogram ascertains diagnosis of the arterial occlusion and provides the underlying cause of the ischemia. The duration of the ischemia is an independent risk factor, which means earlier diagnosis and a better outcome. Although the accurate ischemic time remained unknown, this patient was prepped for operation about 32 h after the onset of the mild symptom in his limb. Although the consequences of revascularization in a limb-threatening ischemic limb may be life-threatening, it is believed that immediate treatment should be attempted in the late presenting limb considering the absence of gangrene. 8
The most appropriate management should be determined by the severity of ischemia, the location of artery occlusion, and overall medical conditions of the patient. 9 Two commonly used approaches are endovascular therapy and surgical therapy. The use of vascular covered stent in patient with isolated common iliac occlusion is also reported, and the follow-up is fairly satisfactory.10,11 This approach appeals to surgeons due to the advantages of easier access to the target location, reduced blood transfusion requirement, and decreased potential need for systemic heparinization. 12 However, vessel perforation and subsequent severe bleeding are unexpected complications when the vascular covered stent is placed in the traumatic artery, especially in cases in which the extent and accurate location of the lesions remain unclear. Furthermore, the appropriate stent graft (lambdoidal shaped), determined by the location of occlusion (Figure 1), is not routinely stored in our hospital. Considering the possibility of traumatic artery hemorrhoea and the time-consuming access to appropriate stent graft, we eliminated the choice of endovascular therapy. Conventional surgical therapy or embolectomy of the traumatic iliac artery also presents high risk for unexpected massive hemorrhage. In this case, considering the unilateral occlusion of iliac artery, extra-anatomic prosthetic bypass grafting (femorofemoral bypass) was used to achieve the occlusive iliac revascularization. It is currently used especially when the approach at the iliac artery is problematic because of a hostile abdomen. 13 This surgical modality without the exposure of the traumatic common iliac artery is especially valid in urgent procedures to minimize the total ischemic time and provide good midterm results. Rinckenbach et al. 14 have confirmed its safety (no perioperative death, no graft infections) and its durability (96.4% secondary patencies at 3 years).
Once arterial flow has been restored, the compartment syndrome resulting from the ischemic reperfusion injury should be on the alert. Compartment syndrome is a surgical emergency, which is caused by raised pressure within a closed fascial envelope; it reduces capillary perfusion below a level necessary for tissue viability. 15 Early diagnosis and prompt management are desperately needed to minimize the related functional loss. The pain (disproportionate to the size of injury and aggravated by the passive stretching) and physical examination (tense muscle that are tender to palpation, motor and sensory deficits) contribute to the diagnosis of compartment syndrome. However, the measurement of intracompartmental pressure remains the gold standard. 16 Following the diagnosis, the four-compartment fasciotomy is the only way to achieve fascial decompression and to preserve skeletal muscle viability. Wound closure after fasciotomy still remains controversial. At our institution, VSD is usually used for the primary wound closure due to limb swelling. The vacuum-assisted closure has a positive therapeutic effect by improving blood circulation in the wound through stimulating angiogenesis, decreasing the permeability of blood vessels and wound edema through narrowing endothelial spaces and restoring the capillary membranes, 17 thus promoting the formation of granulation tissue.
Fortunately, we carried out a successful remedy for the acute limb ischemia. This patient’s recovery was uneventful after a series of complicated, but effective managements and a 6-month follow-up turned out to be helpful in the preservation of the limb viability. However, there is no doubt that the treatments would have been simpler, and the postoperative course would be smoother without the missed diagnosis.
Conclusion
Acute iliac artery occlusion secondary to blunt abdominal trauma is rare, and its clinical manifestations may be concealed by significant abdominal presentations initially, posing a diagnostic challenge at its early stage. We report this case in order to emphasize the role of prudent recognition of the vascular system in avoiding the missed diagnosis after abdominal trauma and to share our experience in the appropriate urgent revascularization of the acute ischemic limb under complete considerations of the underlying cause of the ischemia.
Footnotes
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.