
Abstract
The incidence of bile leaks following blunt liver trauma ranges from 0.5% to 21%. Bile leaks could give rise to biliopleural fistula, which can end up causing cholethorax, where a bilious effusion is seen in the pleural cavity. Early recognition of this condition is essential for favorable outcome. We report an unusual case of delayed biliopleural fistula causing cholethorax in a 30-year-old male, presented following blunt abdominal trauma following a motor vehicle collision. Abdominal examination revealed tender right upper quadrant. He was haemodynamically stable following initial resuscitation. Computed tomography of the abdomen revealed American Association for the Surgery of Trauma grade IV liver laceration without active extravasation of contrast, causing a moderate haemoperitoneum. Decision was made to manage the liver injury conservatively. Repeat imaging performed on day 11 due to progressive abdominal distension revealed bilateral pleural effusions and increased amount of abdominal free fluid. Bilateral intercostal tubes and an ultrasound-guided pigtail catheter was inserted to the abdomen. The right-sided intercostal(IC) tube drainage found to be bilious, along with a bilious drainage through the pigtail catheter placed on the peritoneal cavity. Due to persistently high drain output, an endoscopic retrograde cholangiopancreatography performed revealed a contrast leakage at cystic duct. Sphincterotomy was performed and a biliary stent was placed. Patient completely recovered following decompression of biliary system. The unusual presentation of biliopleural fistula requires a good clinical acumen for early diagnosis. Timely endoscopic and interventional radiological management for biliary decompression and drainage are required for a successful outcome.
Introduction
The incidence of bile leaks following blunt liver trauma ranges from 0.5% to 21%. 1 The incidence is more in high-grade liver injuries. 2 Direct trauma, secondary rupture of subcapsular hematoma and bile duct ischemia can give rise to bile leaks. 1 These bile leaks can range from simple intraparenchymal or extraparenchymal bile leaks to more complex biliopleural fistula (BPF) formation. 2
BPF can give rise to cholethorax, an even rarer but well-known complication where a bilious effusion is seen in the pleural cavity. 3 Bile in the pleural cavity can be damaging to the lungs and pleura due to the corrosive nature of bile and may further worsen the condition of the patient with already compromised physiology due to the initial trauma. 4 This warrants early recognition and prompt management to prevent significant morbidity and mortality.
We report a case of a young male who presented following blunt trauma to abdomen due to motor vehicle collision causing an American Association for the trauma of Surgery 5 (AAST) grade IV liver laceration, who developed a delayed BPF and cholethorax.
Case presentation
A 30-year-old, previously healthy male, presented to the trauma room following a motor vehicle collision. He was a restrained driver who impacted against a fixed object. During primary survey, he was found to have a pulse rate of 120 bpm and a blood pressure of 90/70 mmHg. He was tachypneic with a respiratory rate of 24/min with equal bilateral air entry to lungs and on-air saturation was 97%. The Glasgow coma scale 6 (GCS) was 8/15. Abdominal examination revealed tenderness in the right upper quadrant with guarding. As patient had major facial fractures and haemodymic instability, he was immediately intubated to protect the airway. During initial resuscitation, he was transfused with two pints of crystalloids and two units of group-specific blood.
Focused Assessment with Sonography for Trauma scan revealed moderate amount of free fluid in the abdomen. Therefore, after initial resuscitation and stabilization of the patient, Computed tomography (CT) of the chest, abdomen and pelvis was performed with X-ray imaging of the relevant limbs. His CT of the brain was unremarkable. CT of the abdomen revealed AAST Grade IV liver laceration without active extravasation of contrast, leading to a moderate haemoperitoneum (Figures 1 and 2). Apart from that the patient was found to have left-sided fractures involving maxilla, clavicle and first rib, without any vascular or nerve injury which were attended and managed by the orthopedic and oral-maxillofacial teams later. During primary survey, he was found to have a pulse rate of 120 bpm and a blood pressure of 90/70 mmHg. He was tachypneic with a respiratory rate of 24/min with equal bilateral air entry to the lungs, and on-air saturation was 97%. After resuscitation with blood products and crystalloids, the pulse rate was 88/min, the BP was 120/90 mmHg and the respiratory rate was 18/min. On admission, FBC showed Hb 7 g/dl and following resuscitation and blood transfusion, it was 10 g/dl.

CT images of the abdomen (arterial phase) showing laceration involving segment VI/VII/VIII/IVA with haemoperitoneum.

CT images of the abdomen (venous phase) showing laceration involving segment VI/VII/VIII/IVA with haemoperitoneum.
As the hemodynamic parameters were stable after resuscitation, decision was made to manage the liver injury conservatively with invasive ventilation and close monitoring of vital parameters at intensive care unit. He was monitored twice with US of the abdomen/liver during this period for intra-abdominal fluid collections. US of the abdomen on day 5, which was performed as control imaging was stable without expansion of liver haematoma. But on day 11 there was increasing ventilator demand and progressive abdominal distension. Therefore, repeat US Imaging was performed and it revealed bilateral pleural effusions and a moderate amount of free fluid in the abdomen, which was comparatively more to the initial images. Therefore, he had repeat CT of the thorax and abdomen. It revealed bilateral pleural effusions and a moderate amount of free fluid in the abdomen which was comparatively more to the initial images (Figure 3).
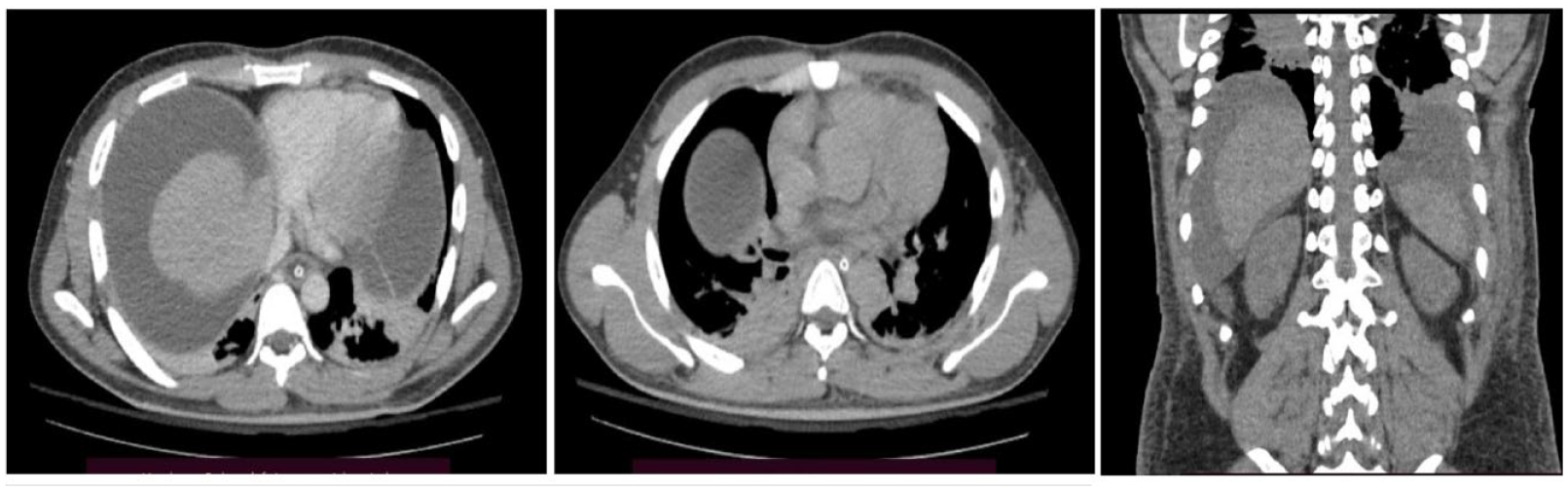
CT of the abdomen, axial and coronal views showing biliopleural fistula.
Subsequently, bilateral intercostal tubes and an ultrasound-guided pigtail catheter to the abdomen were inserted. The right-sided intercostal tube drainage revealed an initial bilious drainage of 1500 ml along with a bilious drainage through the pigtail catheter placed on the peritoneal cavity. IC drain fluid biochemistry showed an elevated bilirubin value that was similar to the bilirubin value of pigtail catheter output. The output of these two drains was persistently high, and the patient’s general condition failed to show much improvement. Therefore, the decision was made to perform endoscopic retrograde cholangiopancreatography (ERCP), which revealed a contrast leakage in the cystic duct. Biliary sphincterotomy was performed during the procedure, and a 17 Fr × 15 cm single-end pigtail catheter was placed to decompress the biliary system and facilitate the healing of the biliary injury. Following this, the patient gradually improved with a reduction in IC tube drainage and pigtail catheter drainage. He was extubated on the 20th day following the injury and was transferred to the ward setup after 23 days of care at an intensive care unit.
Biliary stent was removed 6 weeks after the insertion. Patient remains asymptomatic and his liver functions were within normal limits on 8 weeks follow-up. He was planned to be reviewed in an outpatient clinic with a 3-monthly US of the liver and a liver profile up to 1-year duration.
Discussion
Nonoperative management of high-grade liver injuries in haemodynamically stable patients can be challenging, but safely done with the latest advances in interventional radiology and endoscopic techniques. 7 Failure rates of nonoperative management are shown to be as low as 5.5%. 7 The complication and failure rates of nonoperative management are more with high-grade liver injuries. 1 There should be a low threshold to perform repeat imaging, when conservatively managing patients with high-grade liver injuries, to identify complications early.
Bile duct injuries leading to BPF and cholethorax are among the most devastating complications encountered and according to the literature, most will spontaneously heal with adequate biliary drainage. 1 BPF can be managed surgically, endoscopically or conservatively depending on the extent and the severity of BPF. 8 Conservative management was done with placement of intercostal tube in the pleural cavity, antibiotics and somatostatin analogues. 8 Our patient was initially opted for conservative management after identifying the presence of BFP. As conservative management failed due to persistently high IC tube drainage, endoscopic management was considered. Compared with the surgical management, endoscopic management with ERCP and stenting is more popular and success rates are as high as 90%–100%. 2 As the patient recovered remarkably with ERCP and stenting, our patient did not require surgical management, which is preserved for large BPF or following failure of conservative and endoscopic management.
Conclusion
The unusual manner in which a BPF presents require a good clinical acumen to be detected when the initial CT reveals no definite diaphragmatic tear. A high index of suspicion for anticipating rare complications following trauma and timely endoscopic and interventional radiological management are required for successful outcome.
Footnotes
Acknowledgements
Authors wish to acknowledge the nursing staff who took care of this patient during the hospital stay.
Authors’ note
Authors’ contribution
Y.M.K.A.Y. and D.S. designed the article. Y.M.K.A.Y. and B.P. wrote the article. D.S. critically analysed the article. Y.M.K.A.Y., R.M. and D.S. involved in the patient management. All authors read and approved the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval was not sought for the present study because according to our institutional policy ethics approval is not necessary for case reports.
Informed consent
Informed written consent was obtained from the patient for the publication of this case report and any accompanying images. This patient was fully recovered and currently on follow-up as an outpatient. This case was designed to be written with the consent of the patient once he had fully recovered with a GCS of 15/15.
Trial registration
Not applicable.