
Abstract
Objective:
Diabetes can lead to diabetic retinopathy, which damages the retina due to blood flow remodeling of occular vessels. Early stages of diabetic retinopathy may not present with patient symptoms. Doppler indices, of the ophthalmic arteries, could help in determining the effect of diabetic vascular remodeling. This research was designed to compare the Doppler indices, in the ophthalmic artery and central retinal artery, in both diabetic and nondiabetic patients.
Materials and Methods:
This was a cross-sectional observational study of 72 total patients. Sonography was performed on the ophthalmic arteries of 36 diabetics and 36 nondiabetics, to compare Doppler indices. All patients were voluntarily consented to this research that was approved by the university’s Institutional Review Board (IRB). Doppler parameters recorded were peak systolic velocity, end dystopic velocity, resistive index, and pulsatility index, which were taken in both patient groups and compared.
Results:
A significant difference was noted in the ophthalmic artery peak systolic velocity, end-diastolic velocity, pulsatility index, and resistive index for diabetic and nondiabetic individuals, with a statistically significant set at .01.
Conclusions:
There was a significant difference between diabetic and nondiabetic ophthalmic Doppler indices in this cohort of patients. This cohort demonstrated vascular remodeling of the ophthalmic arteries, caused by diabetes; therefore, blood flow resistance was increased due to diabetes.
Diabetic retinopathy (DR) is a disease of the retina, caused by diabetes, that can damage tiny occular vessels. Early disease may not present with patient symptoms. 1 As the disease progresses, these tiny vessels become fragile and can bleed, blur vision, and destroy the retina. Diabetic patients are at significant risk for DR. For these reasons, it is strongly recommended that all diabetic patients have an eye examination, at least twice a year. 2 Spectral Doppler can be used for the assessment of retrobulbar velocity metrics such as peak systolic velocity (PSV), end-diastolic velocity (EDV), and mean velocity, within the eye. Reproducible blood velocity measurements have been reported with this sonographic technique. In addition to blood flow velocity, spectral Doppler also allows for the measurement of the resistive index (RI) and pulsatility index (PI) of recorded waveforms. 3
Hyperglycemia levels can also cause edema within the retina’s blood vessels and limit the functionality of the retina as well as put pressure on the optic nerve, leading to retinopathy. 4 Optical coherence tomography has been used to assess retinal thickness and intraretinal pathology as well as wide-field fundus photography to reveal clinically asymptomatic microvascular lesions. 5 Treatment of diabetic macular edema is now achieved by intravitreous injection of anti-vascular endothelial growth factor agents, and the same drugs are now used for proliferative diabetic retinopathy (PDR). Improvements in medications and devices, for systemic treatment of diabetes, has also improved patient’s ability to optimize their metabolic control. A recent position statement incorporated these recent developments as a guide for both physicians and patients. It states that PDR is a highly specific neurovascular complication of both type 1 and type 2 diabetes and their prevalence strongly correlates to both the duration of diabetes and level of glycemic control. 6 This was based on evidence provided by Solomon et al’s 6 pooled meta-analysis, which involved 35 studies conducted worldwide. They estimated a global prevalence of DR and PDR, among patients, to be 35.4% and 7.5%, respectively. 6 DR is the most frequent cause of acute onset of blindness, among adults 20 to 74 years of age, in developing countries. Glaucoma, cataracts, and other disorders of the eye can occur earlier and more frequently, in diabetic patients. 6
The ophthalmic artery (OA) is a branch of the internal carotid artery, which supplies the orbital structures. The central retinal artery (CRA) and posterior ciliary arteries are branches of the ophthalmic arteries, which supply the retina and ciliary muscles, respectively. 7 The CRA vascularizes the retina and is of critical importance for vision. Diabetes affects ocular circulation and altered blood flow which may contribute to the development and progression of DR. 8 Doppler evaluation of the OA is a quick noninvasive diagnostic technique. 9 Therefore, ophthalmic spectral and color Doppler can play an important role in the evaluation of hemodynamic changes. 10 However, Doppler is not commonly performed, in many clinical settings, for detection of hemodynamic changes within the OA and CRA. In diabetic patients, early diagnosis and management could be helpful to avoid the development of serious complications such as DR. 11
Materials and Methods
This cross-sectional, observational study was conducted at the sonography clinic in Lahore, Pakistan. The aim was to compare the resistive indices, of the OA, in both diabetic and nondiabetic patients. The Board of Studies and the Institutional Review Board (IRB), at the University of Lahore, approved this research protocol. A total sample of 72 patients was calculated to obtain statistical power. For comparison, 36 nondiabetic and 36 diabetic patients were recruited. Participation was voluntary and written consent was obtained from the patients or their guardians. The ultrasound machine used in the study (Xerio, Toshiba) was equipped with a linear transducer that provided 7 to 14 MHz frequency, for the OA examination. 12 The research and examination techniques were explained to each of the patients. Each patient was placed in a recumbent position, with the head tilted back, or supine. A large amount of aqueous ultrasound transmission gel covered the closed eyelid and minimal to light transducer pressure was applied. Excess transducer pressure, on the globe, can result in imaging artifacts. Both eyes were imaged through closed eyelids and the patient’s gaze was directed at the ceiling. To perform the sonographic examination of the orbit, the ultrasound equipment settings were set at a mechanical index (MI) of 0.6, which limited the bioeffects to the eye (Figure 1). This was based on the linear-array transducer having frequencies with a bandwidth of 5 to 10 MHZ. It is important to note that this ultrasound equipment setting only displayed the MI setting for gray-scale images and not for the use of color and spectral Doppler images. Imaging was conducted through the eye and orbit in multiple scan planes to identify the desired structures and vessels. For consistency, gray-scale imaging was used to locate normal structures, which included the globe, optic nerve, extraocular muscles, and orbital blood vessels. Intraocular structures included the anterior chamber, lens, and vitreous cavity were also visualized (Figure 2). The OA can be detected at nasal side (medially) (Figure 3). The vessels were identified by using Doppler and this ocular interrogation was performed with a gate size of 1.5 mm, as well as proper Doppler angle correction. The CRA was visualized as a fine vessel that was situated in the central part of the optic nerve (Figure 4). The vessel’s best velocity spectrum can be achieved with a Doppler angle ranging from 0° to 20°. 13 This enabled researchers to attain the maximum Doppler shift values. Usually, the vessel’s spectrum was captured with the blood flow that was within the central retinal vein (CRV). The color and spectral Doppler helped to distinguish between the various vessels that are at or near the optic nerve, such as the CRA and CRV. Spectral waveforms of the desired vessels were obtained by proper sample volume placement. The vessels for this research study were identified based on the demonstrated vascular anatomy. The OA can be detected with color Doppler medial to the optic nerve, while the CRA can be found within the optic nerve, approximately 12 mm behind the globe. Angle correction is also needed for the OA as it has an angular vascular course. The parameters including PSV, EDV, PI, and RI were calculated automatically by machine software. The RI is derived by the equation: (PSV – EDV) / PSV. The CRA and OA were interrogated by color Doppler in all the patients. The PSV, EDV, PI, and RI were measured for the CRAs and OAs. All the acquired data were evaluated and analyzed using the Statistical Package for the Social Sciences version 24 (SPSS 24, IBM, Armonk, NY, US). 14 The statistical significance was set a prior at P ≤ .01.
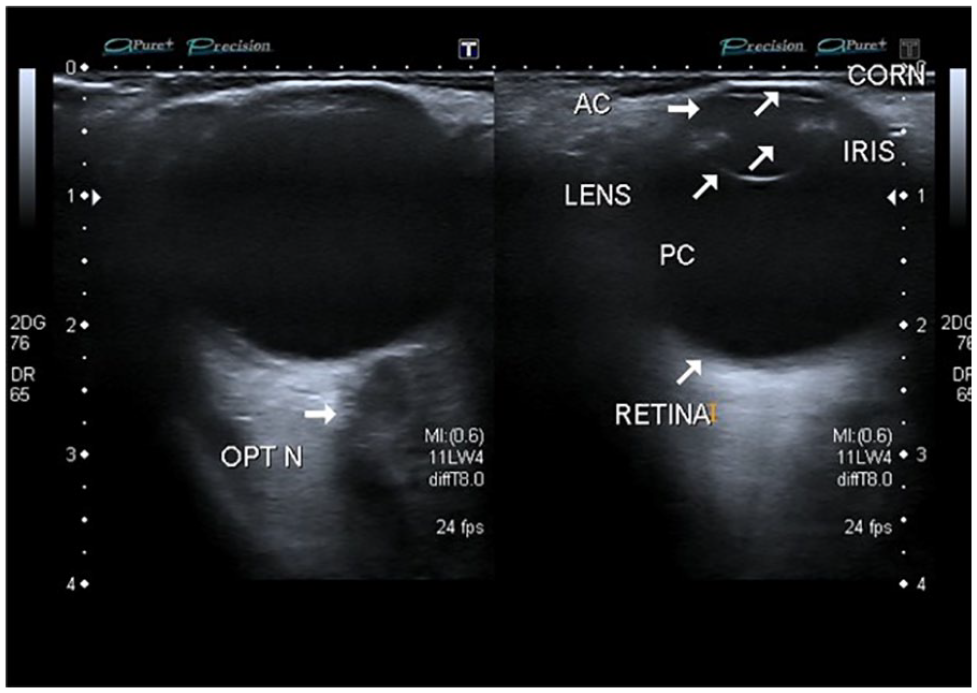
A 2D image demonstrating the anatomy of the eye using a mechanical index of 0.6. DR, diabetic retinopathy.
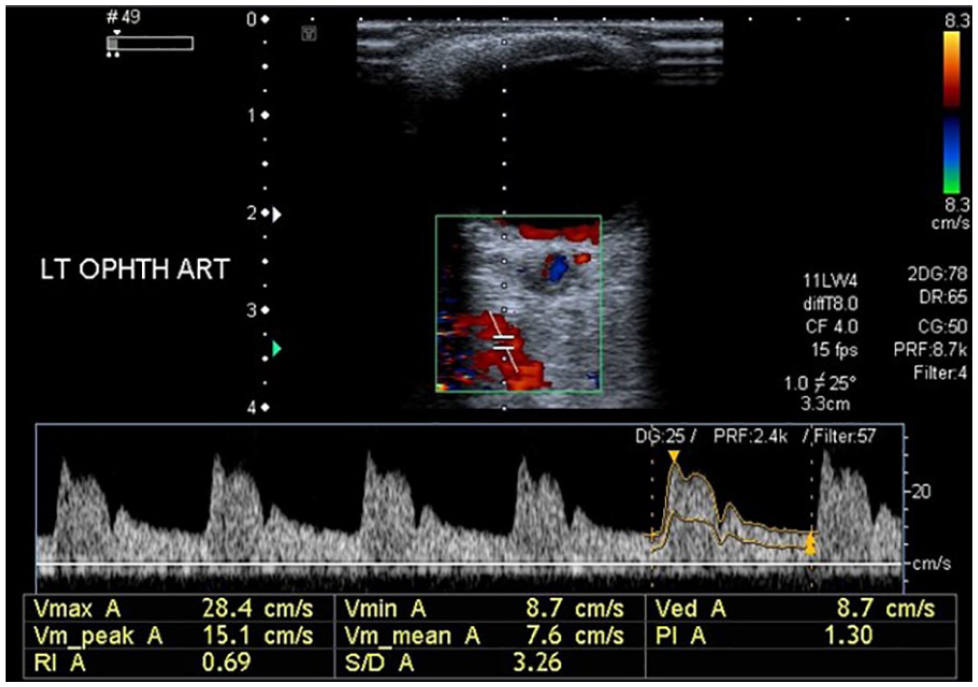
The left ophthalmic artery in nondiabetic individual with normal Doppler indices. PSV = 28.4 cm/s (normal), EDV = 8.7 cm/s (normal), PI = 1.30 (normal), RI = 0.69 (normal). EDV, end-diastolic velocity; PI, pulsatility index; PSV, peak systolic velocity; RI, resistive index.
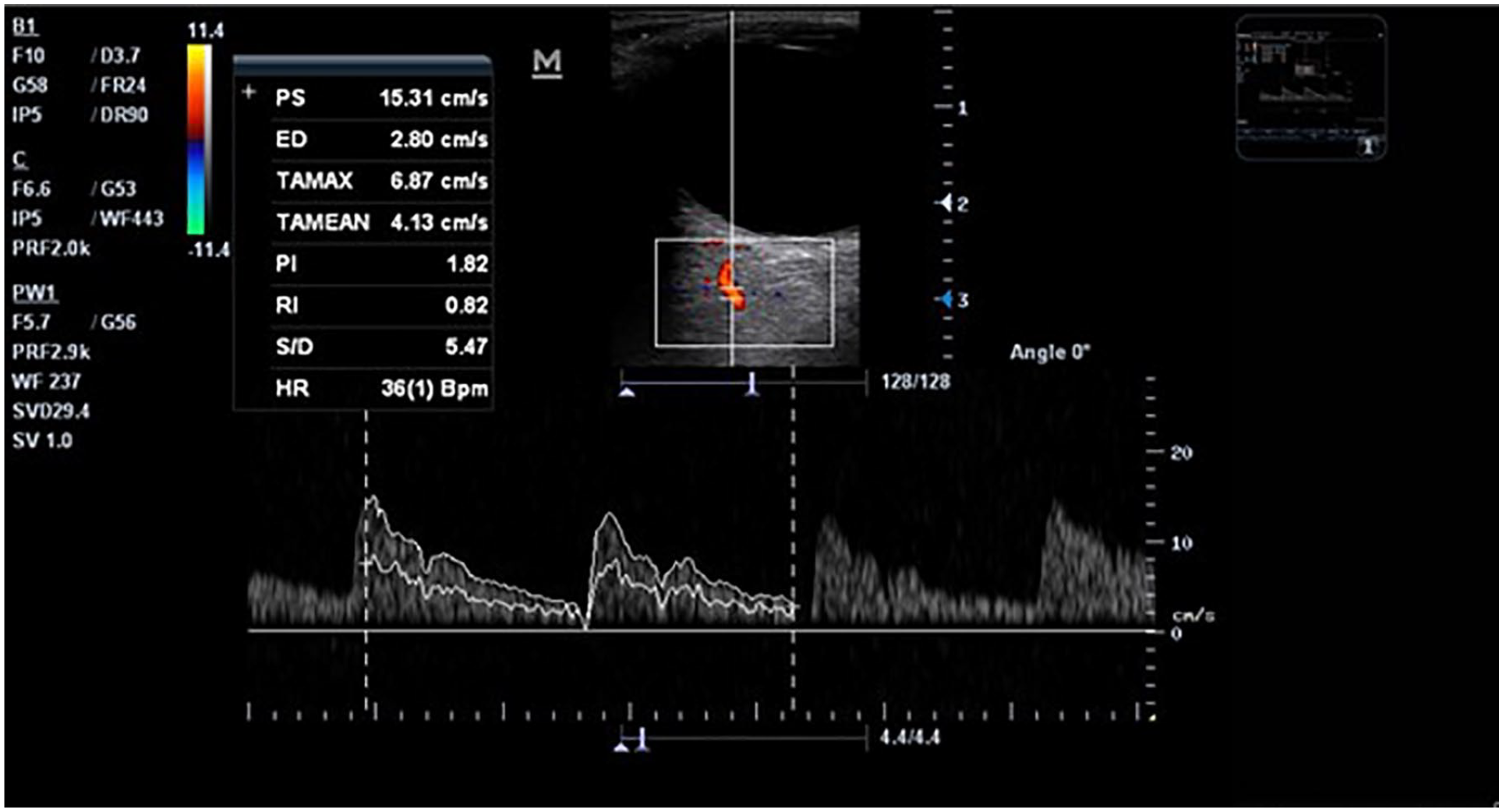
The left ophthalmic artery Doppler waveform showing increased Doppler indices in this diabetic patient. PSV = 15.31 cm/s (too low), EDV = 2.8 cm/s (too low), PI = 1.82 (high) and RI = 0.82 (too high). EDV, end-diastolic velocity; PI, pulsatility index; PSV, peak systolic velocity; RI, resistive index.
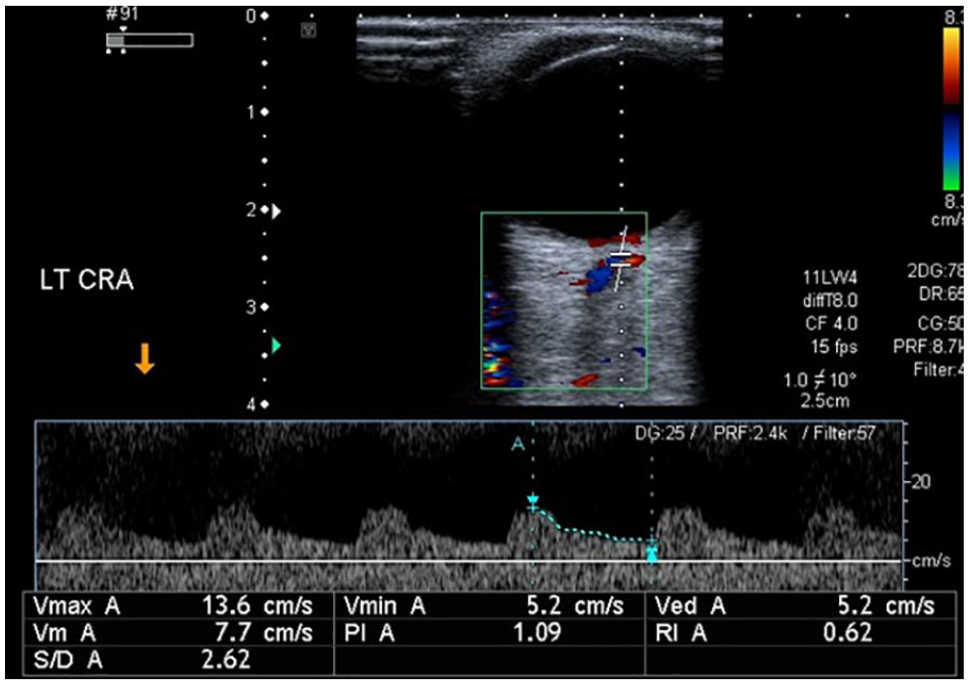
Central retinal artery in nondiabetic individual with normal Doppler indices. PSV = 13.6 cm/s (normal), EDV = 5.2 cm/s (normal), PI = 1.09 (normal), RI = 0.62 (normal). EDV, end-diastolic velocity; PI, pulsatility index; PSV, peak systolic velocity; RI, resistive index.
Diabetic patients were identified by the post-prandial blood test with a glucometer and the duration of diabetes was recorded by taking a patient history. Constitutional signs, symptoms, and demographic data (i.e., age and location) were obtained from the patients, while data related to the Doppler velocimetry of the OA were calculated on the ultrasound machine. The mean and standard deviation values were calculated for patient age. Likewise, the Doppler indices of the CRAs and OAs, in diabetic and nondiabetic patients were recorded for comparison.
The data normality was assessed and it was normally distributed. Independent-sample t test was applied to compare the mean of the Doppler indices of the CRAs and OAs, in diabetic and nondiabetic arteries.
Results
The mean age of the participants was 39.40 ± 9.3 years with the range from 22 to 70 years. The number of male and female participants were 12 (16.7%) and 60 (83.3%). In this cohort, 36 patients were diabetic and the other 36 patients were nondiabetic.
The acquired data from diabetic patients was compared with normal ranges of Doppler indices. The normal range of Doppler indices of the OA were PSV = 30 to 35 cm/s, EDV = 6 to 7 cm/s, RI = 0.77, and PI = 1.21. The normal range of the Doppler indices of the CRA were PSV = 7 to 10 cm/s, EDV = 3 to 5 cm/s, RI = 0.69 and PI = 1.05, which were all compared with the nondiabetic patients.
The mean and standard deviation of the Doppler indices for the diabetic and nondiabetic individuals were compared. A significant difference was seen in PSV, EDV, PI, and RI for diabetic and nondiabetic patients (see Table 1). A significant relation was found between diabetic and nondiabetic, with the Doppler indices of the OA, and for all the indices, the P values were significant at .01 level.
Comparison of the Mean and the Standard Deviation in Diabetic and Nondiabetic Individuals.
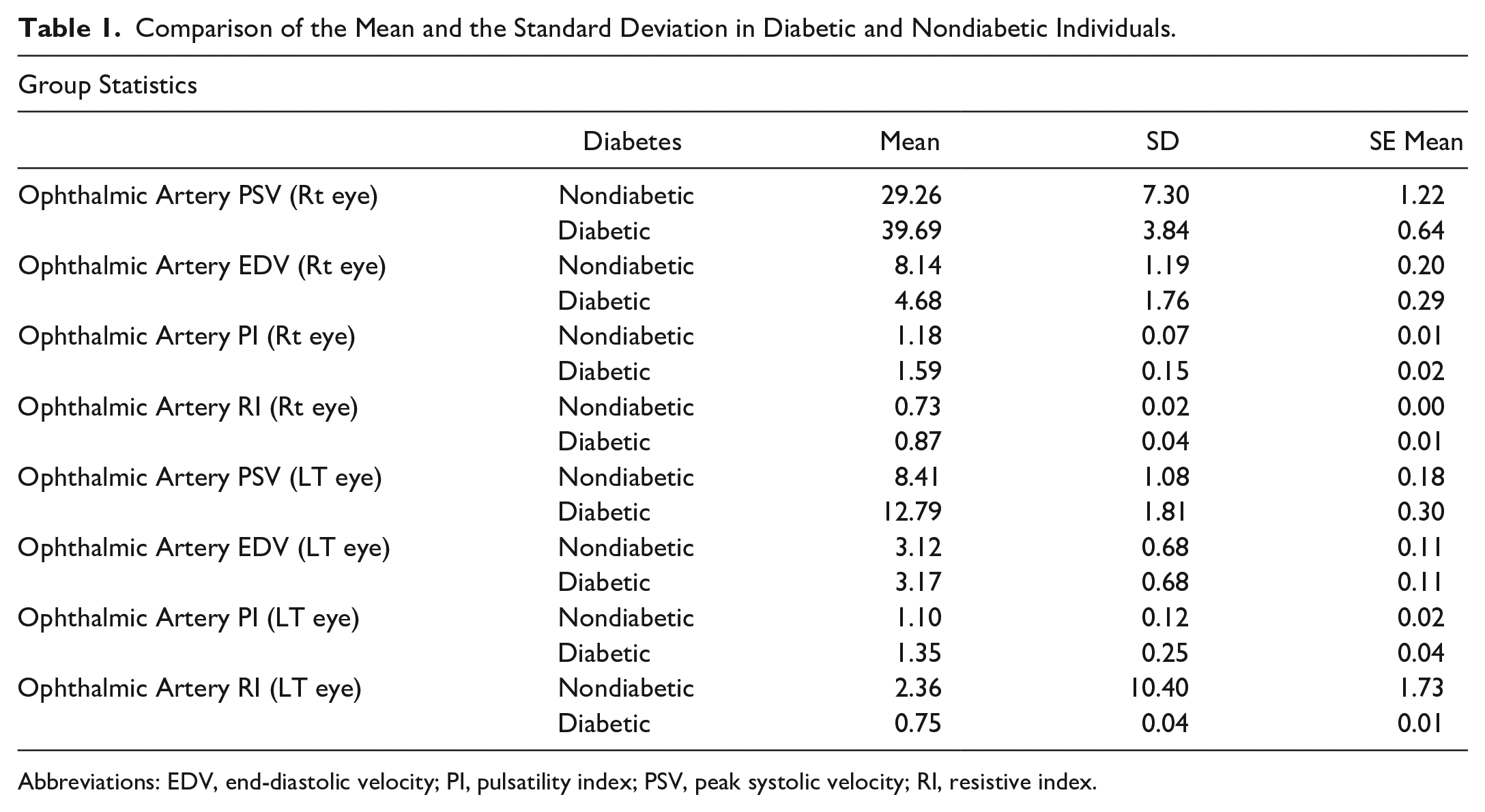
Abbreviations: EDV, end-diastolic velocity; PI, pulsatility index; PSV, peak systolic velocity; RI, resistive index.
Discussion
Visual impairment is the most common microvascular complication of diabetes mellitus and the foremost cause of blindness.15,16 In a research study conducted by Sarkar et al, they measured ocular blood flow velocities, RI, and PI, within the OA, CRA, CRV, and carotid artery, using color and spectral Doppler. In their study, an analysis was done with middle-aged diabetic and nondiabetic groups, for comparison. The mean RI within the OA was found to be significantly higher in the diabetic group (0.74 ± 0.11) than the nondiabetic group (0.66 ± 0.13), at a P value of .002, 17 while the mean PI within the OA was found to be significantly higher in the diabetic group (1.55 ± 0.48) than in the nondiabetic group (1.22 ± 0.39), with a P value of .002. 17 In a pilot study by Somfai et al, 18 they noted that ocular blood flow in diabetic patients showed a reduction in PSV, EDV, and RI with values of PSV = 0.01, EDV = 0.07, and RI = 0.03.
In a study by Wang et al, 64 patients were studied in group groups: healthy, diabetic without retinopathy, background retinopathy, and proliferative retinopathy. The RI among diabetic patients, with proliferative retinopathy, had the highest mean of 0.83 and the lowest mean was 0.54, among healthy subjects, at a P ≤ .001. The PI values were also highest among their diabetic patients. Results of that study demonstrated that the sensitivity, specificity, positive, negative predictive values, and overall accuracy of RI and PI, in diabetic patients with proliferative retinopathy, had the best cut-off values of 0.645 and 1.0175 for 100%. Wang et al also indicated that an OA’s RI and PI were significantly increased in their patients, with DR. However, their sensitivity and specificity for detection of retinopathy was 100%. They advocated that color Doppler was a more efficient screening method for diabetic patients with retinopathy. 19 The results of the current cohort study agreed with these research studies, as shown in Table 1. There was a significant difference between the means of all the Doppler parameters in diabetic and normal patients, of the same age group, body habitus, and gender. Orbital blood flow velocities in diabetics have been reportedly increased in some studies, 16 decreased in others, 17 or unchanged. Numerous clinical studies have demonstrated increase in the RI, in the retrobulbar vessels, with progression of DR. 17 Increased RI has also been reported in the OA and posterior ciliary arteries, of DR patients. 18 Few studies have also demonstrated increased PI, with PDR. 11
In the current study, 60 females and 12 males were included with a male to female ratio of 1:5. According to a study by Ozawa et al, 21 the frequency of DR among males and females was 43.62% and 56.38%, demonstrating a 1:1.3 male to female ratio. The researchers explained that for their study, the incidence of type 1 diabetes was greater in males, whereas with type 2 diabetes, the incidence was greater in females. Type 2 diabetes most commonly leads to retinopathy therefore female gender is more involved. 20
Large studies of diabetic patients, for suspected DR, have been conducted. In a study by Mahar et al, 22 about 19 000 individuals were included with ages ranging from 30 and 90 years. In a pilot study conducted for the prevalence of DR in Pakistan, 3000 diabetic individuals were included with 26% of the patients having retinopathy; 52% of the patients were males and 48% females. 23 In a study conducted by Zou et al, 12 they included more than 5000 individuals, and the mean age of DR and non-DR was 58.2 ± 14.0 and 60.0 ± 12.0 years, respectively. Interestingly, Wubben 24 indicated that as a result of their research, retinal dysfunction, prior to the microvascular changes, could be detected with an elecroretinogram. This is a difficult procedure as dilation of the pupils is required pre-procedure and placement of Alkane electrodes. Patient cooperation is needed so that eye movements are limited. 13 Although it is a good technique to check retinal dysfunction prior to microvascular changes, it may not be feasible for all patients. In the current study presented, injections were not used for any of the patients. No preparation was required before the examination as it only required a small amount of aqueous ultrasound gel, which was not harmful to the eye. No ultrasound bioeffects have been reported using a MI setting of 0.6. Spectral Doppler sonography can detect any vascular resistance from the eye structures in the form of increased resistive indices (see Figure 3). In the current study, the mean age was 39.40 with a standard deviation of 9.3 years. Blood sugar levels were checked on all the study patients and a mean glucose level of 188 mg/dL with a standard deviation of 77.63 mg/dL was found. The significant increase in Doppler indices among this cohort of diabetic patients was an indication of ocular blood flow remodeling, as well as possibly other organs and systems.
Conclusions
These cohort study findings may indicate disturbances of retinal and choroidal circulation in patients with diabetes. Significant changes in ocular retrobulbar blood flow can be found with DR, which can be detected with color Doppler. These imaging techniques could serve as diagnostic screening to assess hemodynamic changes, in different stages of DR. There was a significant difference between diabetic patients and nondiabetic ophthalmic Doppler indices. The findings of altered velocities in the CRA and the OA of diabetic patients, with an increased RI, may suggest the involvement of both retinal and choroidal circulation, as part of the disease process. Monitoring with color Doppler may have predictive power in identifying those at greatest risk of developing PDR. Further studies with a larger group of patients are needed to understand better the role of retrobulbar hemodynamics, in the pathogenesis of diabetes.
Footnotes
Ethics Approval
The ethical approval was taken from the ethical committee of the University of Lahore.
Informed Consent
The informed consent was also taken prior to the start of the scan.
Animal Welfare
Not applicable.
Trial Registration
Not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.