
Abstract
Uterine artery Doppler has been a useful aid in the sonographic evaluation of uteroplacental hemodynamics of the gravid uterus. Pulsatility index, resistive index, and systolic/diastolic ratio can be calculated and interpreted in the evaluation of blood flow. The waveform itself can be evaluated for diastolic notching and used to interpret the qualitative appearance of the blood flow. In addition to the hemodynamic characteristics, practitioners have incorporated maternal serum tests to attempt to isolate at-risk candidates. This article summarizes the effectiveness of each methodology, with a primary focus on an at-risk population, since studies of low-risk populations have not demonstrated significant sensitivity for prediction of complications such as pre-eclampsia, placental abruptia, or fetal demise.
Keywords
Introduction
During a routine low-risk pregnancy, the uterine arteries undergo a trophoblastic change in which the hemodynamics transition from a high resistive blood flow to a low resistive blood flow (Figure 1). This is to perfuse the uteroplacental system with oxygenated blood to allow for adequate fetal development. Complications of fetal development and well-being can occur when this transition is compromised. There are predisposing health conditions that have been identified with interrupting this hemodynamic transition such as hypertension, diabetes, autoimmune disorders, clotting disorders, and renal disease, as well as maternal factors, such as body mass index (BMI) and ethnicity, that increase chances of pregnancy complications.1–3
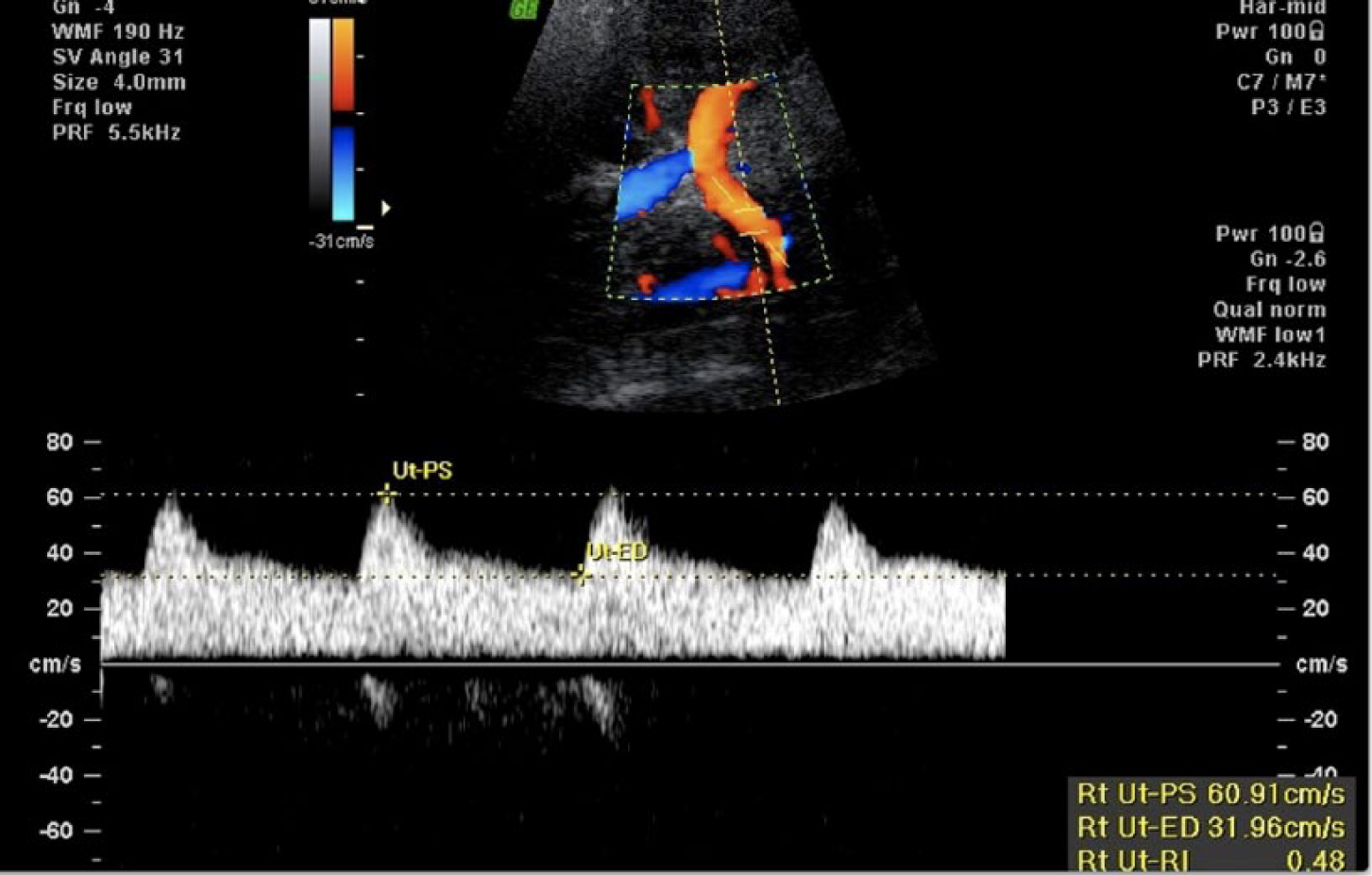
Spectral and color Doppler image of a normal right uterine artery showing the characteristic low resistance waveform (peak systolic velocity [Ut-PS] = 60.9; end diastolic velocity [Ut-ED] = 31.9; resistance index = 0.48).
Uterine artery Doppler has been a useful aid in the sonographic evaluation of uteroplacental hemodynamics of the gravid uterus. Over the years, practitioners have been using it as a predictive tool to analyze or isolate pregnancies that are at-risk for adverse outcomes. Numerous parameters can be calculated in the evaluation of the blood flow; typical quantitative values used include the pulsatility index (PI), resistive index (RI), and systolic/diastolic (S/D) ratio. The waveform itself can be evaluated for diastolic notching, defined as an early diastolic velocity measurement lower than the mid-diastolic measurement, used to interpret the qualitative appearance of the blood flow (Figure 2). There have been numerous studies that have demonstrated the benefits of uterine artery Doppler in assessing for pregnancies at an increased risk for adverse pregnancy outcomes.1–6 However, there is debate as to which Doppler parameter provides the best screening parameter to most effectively isolate the potentially problematic pregnancy. In addition to the hemodynamic characteristics, practitioners have also tried to incorporate maternal serum tests in the attempt to isolate at-risk candidates.7,8 The goal of this article is to summarize the effectiveness of the different methodologies reported in the literature, concentrating primarily on at-risk populations, since studies of low-risk populations have not demonstrated sufficient sensitivity for prediction of adverse outcomes of pregnancy such as preterm delivery (PTD), intra-uterine growth restriction (IUGR), pre-eclampsia, fetal demise, admission to neonatal intensive care unit, placental abruptia, HELLP syndrome, and proteinuria.2,3
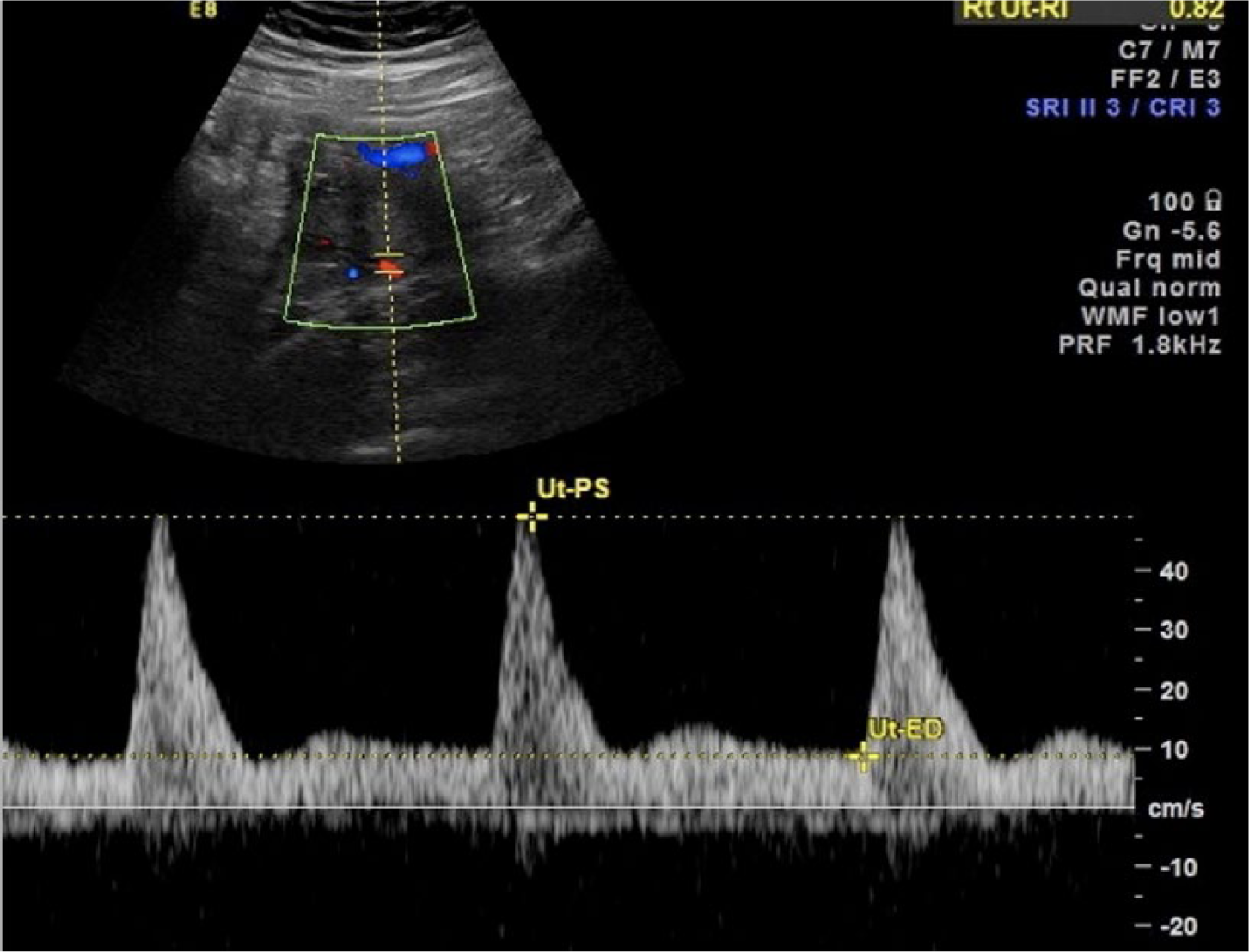
Spectral and color Doppler image of an abnormal uterine artery waveform showing diastolic notching, with an early diastolic velocity (Ut-ED) less than the mid-diastolic velocity.
Methods
The articles selected for review had to incorporate similar parameters of patient selection and comparative statistical criteria in order to logistically analyze the data of each study. For each article, the sonographic methods used had to be described in detail and follow the protocol below. The common denominator for patient selection in each study was pregnant women with increased risk for adverse outcomes.
The sonographic protocol to be used when evaluating a patient in the second trimester and after requires the Doppler sample gate to be placed in the main uterine artery at its level coursing over the iliac vessels to avoid incorrect gate placement in the spiral arteries. The waveforms of the bilateral uterine arteries had to be analyzed using PI, RI, and the presence or absence of notching. A diastolic notch in the waveform of the gravid uterine artery is considered abnormal if detected after the expected time of trophoblastic transition, which begins at approximately 8 weeks gestation and ends between 16 and 20 weeks. 4 This particular marker is widely accepted as an indicator of compromised uteroplacental circulation, with the limitation that the existence of a notch relies solely on the perception of the evaluator. The more objective parameters of resistive and pulsatility indices help quantify the level of blood flow impedance.
Over the years, there have been numerous studies using different Doppler cut-off criteria. This study considers articles dating from 1997 to 2013 to compare the criteria that practitioners have used and to discuss the evolution to the current practice of screening pregnancies for adverse outcomes.
Screening Parameters
Over the time period of interest, the literature on this topic describes many different ways to interpret abnormal blood flow in the gravid uterus. Zimmerman et al 1 used a combination of persistent diastolic notching and an elevated RI > 0.68 in the uterine artery and > 0.38 in the uteroplacental arteries at 21 to 24 weeks’ gestation. 1 In the high- risk population with abnormal Doppler studies, 58.3% had proteinuric pregnancy-induced hypertension (PPIH) and/or IUGR, whereas only 8.3% were adversely affected if Doppler studies were normal. In the low-risk population, 6.4% of patients with abnormal Doppler waveforms developed PPIH and/or IUGR, in comparison to 5.2% in pregnancies with normal waveforms—not a significant difference. Similarly, Coleman et al 2 determined that if both RI values were greater than or equal to 0.7, 58% developed complications (Table 1). In addition, of those patients with bilateral notching, 65% developed complications. The authors noted that risk determination was only slightly improved with the inclusion of notching status, and in the population with RI, less than or equal to 0.58 notching was rarely seen, supporting the observation that using an objective numerical index is similar in efficacy of prediction of adverse outcomes to the more subjective presence of bilateral notching. Albaiges et al 4 also incorporated PI, RI, and notching status in their evaluation. Using a mean RI with a cut-off of 0.67 or a mean PI with a cut-off of 1.41 and bilateral notching had similar sensitivities of 90.5% and 88% as well as similar positive predictive values of 82.6% and 80.8%, respectively. Without the consideration of notching, using cut-offs for RI greater than or equal to 0.69 and for PI greater than or equal to 1.51 had sensitivities just greater than 50% and positive predictive values of approximately 72%.
Prediction of Adverse Outcomes. a
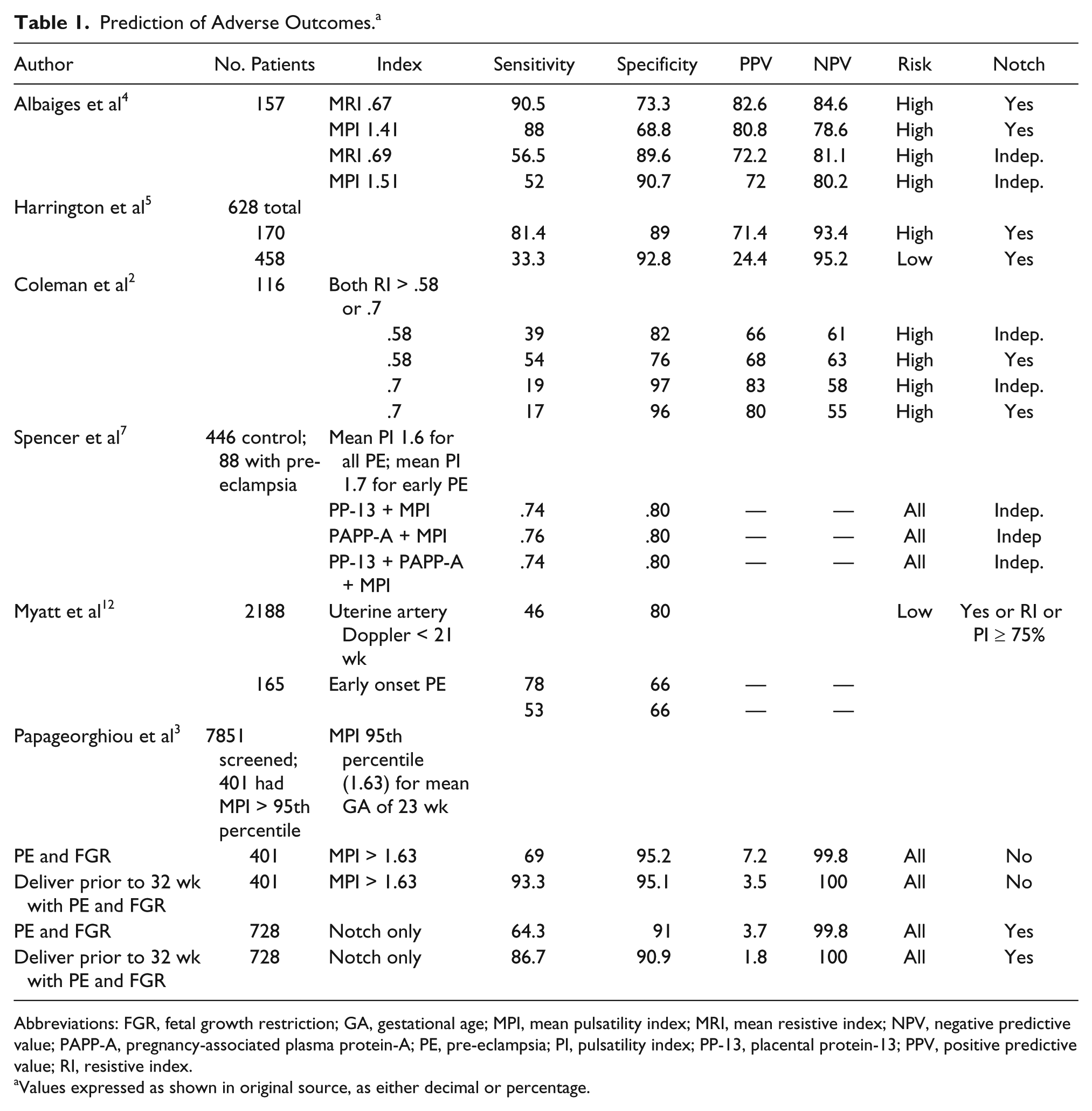
Abbreviations: FGR, fetal growth restriction; GA, gestational age; MPI, mean pulsatility index; MRI, mean resistive index; NPV, negative predictive value; PAPP-A, pregnancy-associated plasma protein-A; PE, pre-eclampsia; PI, pulsatility index; PP-13, placental protein-13; PPV, positive predictive value; RI, resistive index.
Values expressed as shown in original source, as either decimal or percentage.
Other researchers have also incorporated using the means of the Doppler parameters to allow for uniformity in comparison of studies and following any change during gestational age. Napolitano et al 9 evaluated the changes of uterine artery resistance between first and second trimesters to screen for pre-eclampsia (Table 2). They showed that the mean uterine artery PI difference was a better predictor for early onset of pre-eclampsia. Other investigators have evaluated the uterine artery blood flow initially during the second trimester, at 20 to 24 weeks, often with follow-up in the third trimester. Ghi et al 10 and Shwarzman et al 11 included low-risk populations in their analysis. They followed up examinations with a PI greater than the 95th percentile, or 90th percentile in the third trimester. In the study by Ghi et al, 10 62 of 104 low-risk women had persistent abnormal waveforms at the 26- to 28-week follow-up. Ten of these 62 had pre-eclampsia, 20 of 62 had small for gestational age (SGA) deliveries, and 16 of the 62 infants were admitted to the neonatal intensive care unit. Their study also considered “late normalizers” and concluded that this population had an increased risk of SGA (4 of 42 pregnancies). Shwarzman et al 11 evaluated 198 patients with a mean gestational age of 34 ± 3.1 weeks; 80 patients had intrauterine growth restriction, pre-eclampsia, or both. Of the 198 patients, 37 had unilateral abnormal waveforms and 17 had bilateral abnormal waveforms. Patients with bilateral pathological waveforms had a significantly higher incidence of adverse pregnancy outcomes; 15 of the 17 had SGA in comparison to the control group, where only 42 of the 144 patients had SGA. Nine of 17 had PTD compared to the control group, where only 28 of 144 had PTD. The data from these two studies support the value of low-risk pregnancy uterine artery Doppler screening.
Use of Pulsatility Index/Resistive Index to Predict Adverse Outcomes.
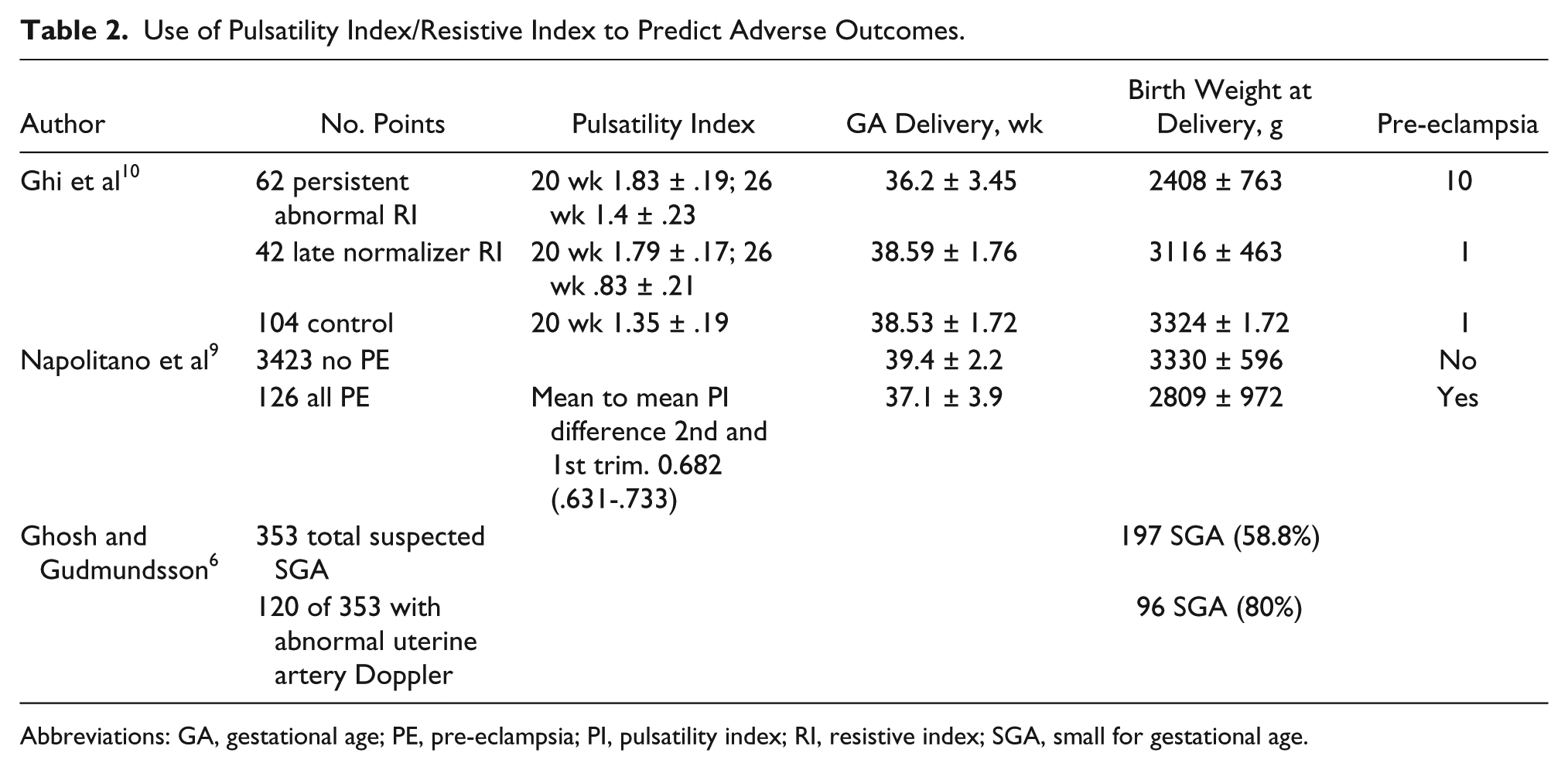
Abbreviations: GA, gestational age; PE, pre-eclampsia; PI, pulsatility index; RI, resistive index; SGA, small for gestational age.
Contrary to these studies, Myatt et al 12 and Harrington et al 5 suggested that uterine artery Doppler screening provides minimum benefit in isolating adverse pregnancy outcomes in the low-risk population. These researchers considered the presence of unilateral and bilateral notching and cut-off values of RI and/or PI greater than or equal to the 50th to the 75th (Myatt) or 80th (Harrington) percentiles. 13 Myatt et al screened 2188 low-risk nulliparous patients, of whom 165 (7.5%) developed pre-eclampsia. Harrington et al evaluated 628 pregnant women at 20 weeks’ gestation. Four hundred fifty-eight women were considered low risk and 170 were clinically high risk. Of the 458 patients in the low-risk population, 30 women had adverse outcomes (6.6%) compared to 48 of the 176 high-risk patients (28.2%) with adverse pregnancy complications (P < .0001). In the study by Harrington et al, for the high-risk group, sensitivity equaled 81.4%, specificity 89%, positive predictive value 71.4%, and negative predictive value 93.4% (Table 1). Harrington et al also concluded that a normal uterine artery Doppler result in the high-risk obstetric patient equalizes the risk to that of an uncomplicated obstetric patient. Although both of these studies had good predictive values of adverse outcomes in the high-risk obstetric patient, their data indicated that uterine artery Doppler screening of the low-risk population was not effective in identifying the potential of adverse complications. In the low-risk population, the criteria used by Myatt et al had only a 46% sensitivity and 80% specificity, whereas Harrington et al had a sensitivity of only 33.3% and a positive predictive value of 24.4%.
As the studies above indicate, Doppler evaluation is an effective tool to interrogate the hemodynamics in the gravid maternal uterine artery and determine the clinical significance of the findings. It aids in the prediction of pre-eclampsia and other adverse pregnancy outcomes, allowing clinicians an earlier opportunity to monitor and treat these patients.14–16 Most of the screening in the past has occurred in the second trimester. More recent studies have incorporated first trimester maternal biochemical markers into the screening to further target these at-risk patients for pre-eclampsia at an earlier stage of pregnancy.7,8 Two of the more common markers considered are PP-13 (placental protein-13) and PAPP-A (pregnancy-associated plasma protein-A). Low values of these markers in the first trimester are associated with increased incidence of developing early pre-eclampsia. Poon et al 8 showed a detection rate for early pre-eclampsia of only 37% when using clinical factors alone, but when they used a combination of uterine artery lowest PI, mean arterial pressure, and serum PAPP-A, they had an 83.8% detection rate for early pre-eclampsia, with only a 5% false positive rate. These results are very comparable to those of Albaiges et al 4 —positive predictive values of 82.6% and 80.8% using the RI and PI, respectively, in the second trimester.
Conclusion
Incorporating early screening tools in pregnancy aids in the prediction of pre-eclampsia and other adverse pregnancy outcomes, providing clinicians an earlier opportunity to monitor and treat at-risk patients. Screening by clinical factors alone has been shown to have a detection rate of early PE of only 37%. 8 Combining maternal factors with first trimester biophysical data such as uterine artery PI and mean arterial pressure more than doubles the detection rate to 78%, and adding serum PAPP-A increases it to 84%. Uterine artery Doppler screening has proven to help isolate at-risk pregnancies.
In the second trimester, increased PI alone and increased PI with notching are both associated with an increased incidence of adverse pregnancy outcomes. Evaluation of the uterine artery in the first trimester and follow-up in the third trimester also provides additional information. A first trimester screening protocol provides clinicians the opportunity to monitor and treat patients. Follow-up uterine artery Doppler in the late second or early third trimester evaluates for late-normalizers who likely have less risk for PPIH but remain at risk for SGA. Persistent abnormal Doppler waveforms are associated with pregnancies that may be more likely to develop complications. Uterine artery Doppler screening is a valuable tool allowing for a noninvasive means of providing pertinent information regarding uteroplacental hemodynamics. Although some studies have suggested increased benefit of screening low-risk populations, the evidence has not been consistent in these patients and factors such as cost and availability may prevent uterine artery Doppler screening from being adopted into routine protocols.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded in part by a grant from the Sonography Research Institute of the Society of Diagnostic Medical Sonography Foundation.