
Abstract
Intracranial arterial Doppler derived resistive indices (RI), peak systolic velocities (PSV), end diastolic velocities (EDV), and pulsatility indices (PI) have been shown to differ across age groups; therefore, the flow parameters in the central retinal artery (CRA) could also be expected to vary. The aim of this study was to evaluate the effect of age in CRA hemodynamics in a convenience sample of healthy men by using Doppler sonography. A total of 100 healthy adult male participants were recruited prospectively. Hitachi (HI VISION Avius) ultrasound equipment was used to measure the CRA PSV, EDV, RI, and PI within the right eye. Data were analyzed to determine velocity flow differences based on age. The results indicated that the CRA’s PSV and EDV declined with increasing age. The CRA’s RI and PI increased with age. Further research is indicated, specifically employing research designs that are statistically powered and use age matching, to generate clinically useful interpretations.
Keywords
Published data have indicated that blood flow Doppler parameters, in the major intracranial arteries, differ across age groups and by sex; therefore, the flow parameters in the ocular vessels would also be expected to vary. 1 However, the data have been inconsistent with respect to age and gender dependency for ocular blood flow parameters.2–4 If such dependency exists, the diagnostic accuracy of color Doppler sonography could be used to compare the velocity measurements that are obtained in clinical evaluations. In addition, it would be important to compare these data with normal reference values, which are specific to age and gender groupings. 5
Retinal vessels (Figures 1 and 2) serve as informative models of microvasculature changes in systemic diseases.6,7
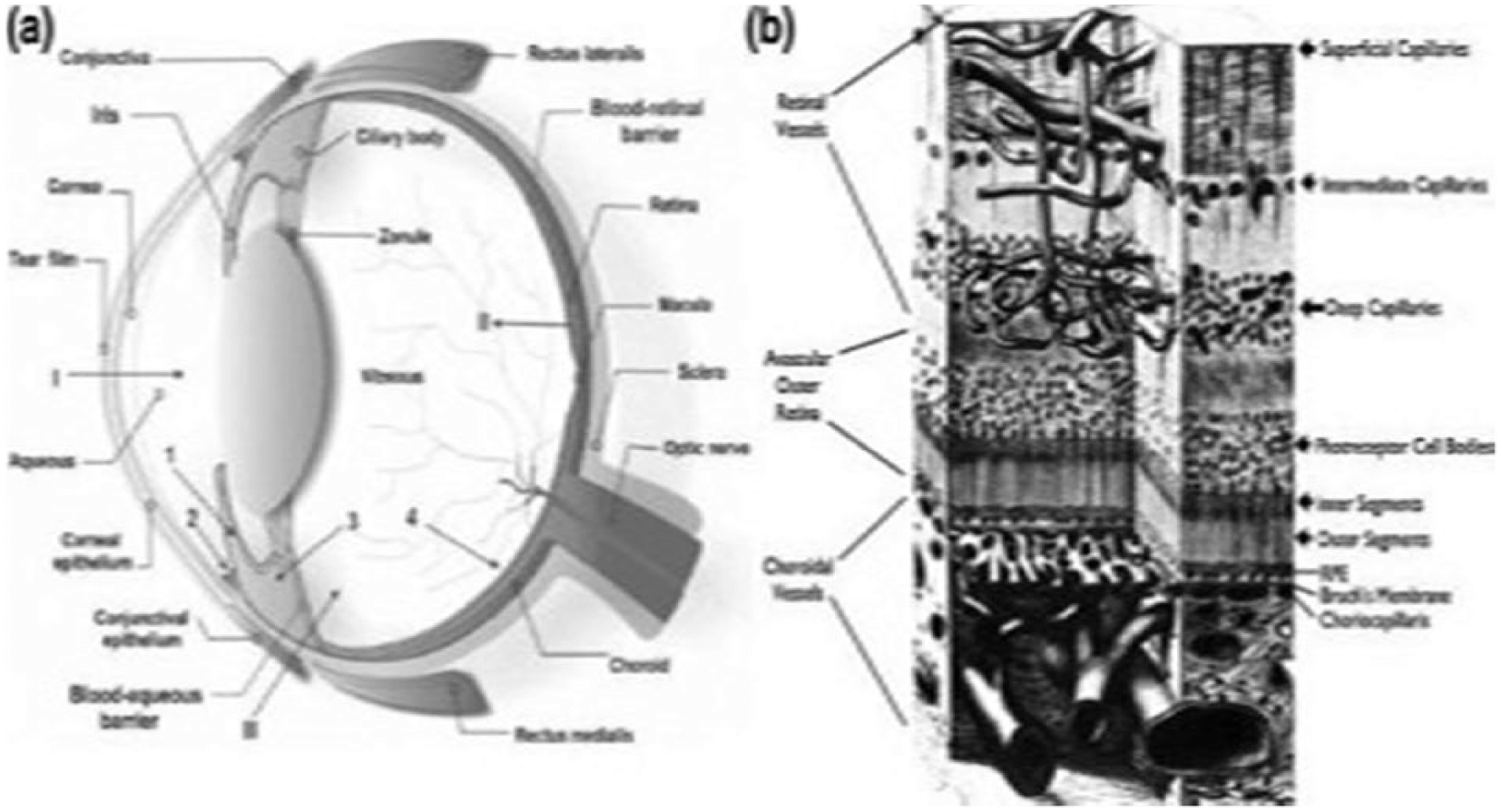
(a) Schematic of normal ocular anatomy; I is the anterior chamber, II is the retinal pigment epithelium (PRF), and III is vitreous. (b) Illustration of the retinal and choroidal vascular systems that nourish the retina in the posterior segment. 6
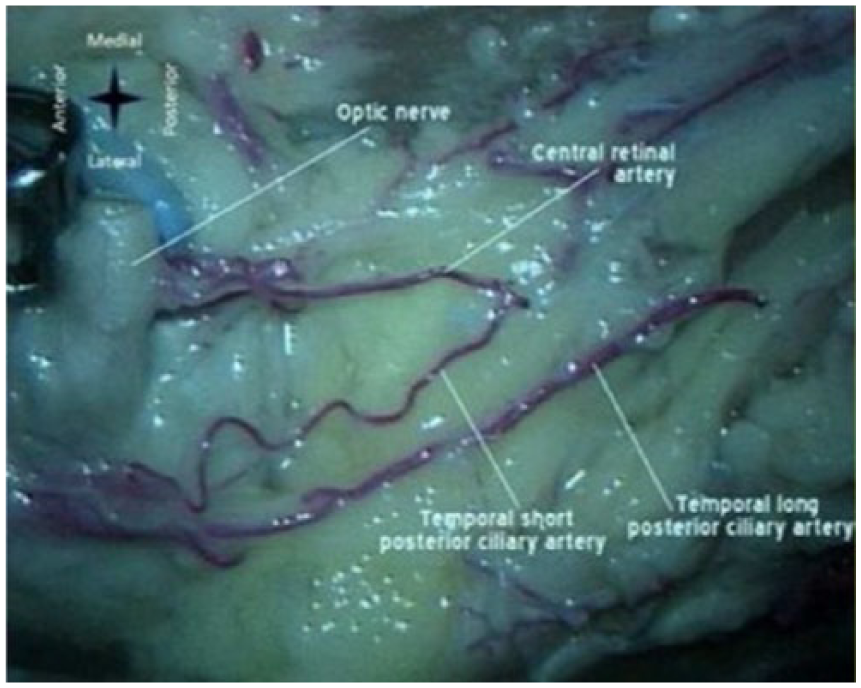
Cadaver image after removal of the proximal part of the optic nerve and overlying structures, demonstrating the origin of the central retinal and temporal short posterior ciliary arteries, from a common trunk. 8
Recently, noninvasive approaches for evaluating the retinal microvasculature have been reported, including scanning laser Doppler flowmetry, color Doppler imaging, and optical coherence tomography.9–11 Spectral Doppler sonography is one of the most widely used and well established techniques for assessing ocular blood flow velocities in the retrobulbar vessels. This is a noninvasive, painless imaging method with highly reproducible results in evaluating central retinal artery (CRA) velocities from spectral Doppler.
Color and pulsed Doppler sonography allows a noninvasive qualitative and quantitative assessment of peak systolic velocity (PSV) in cm/s, end diastolic velocity (EDV) in cm/s, resistive index (RI), and pulsatility index (PI) of the CRA in normal and abnormal cases (Figures 3 and 4).12–14
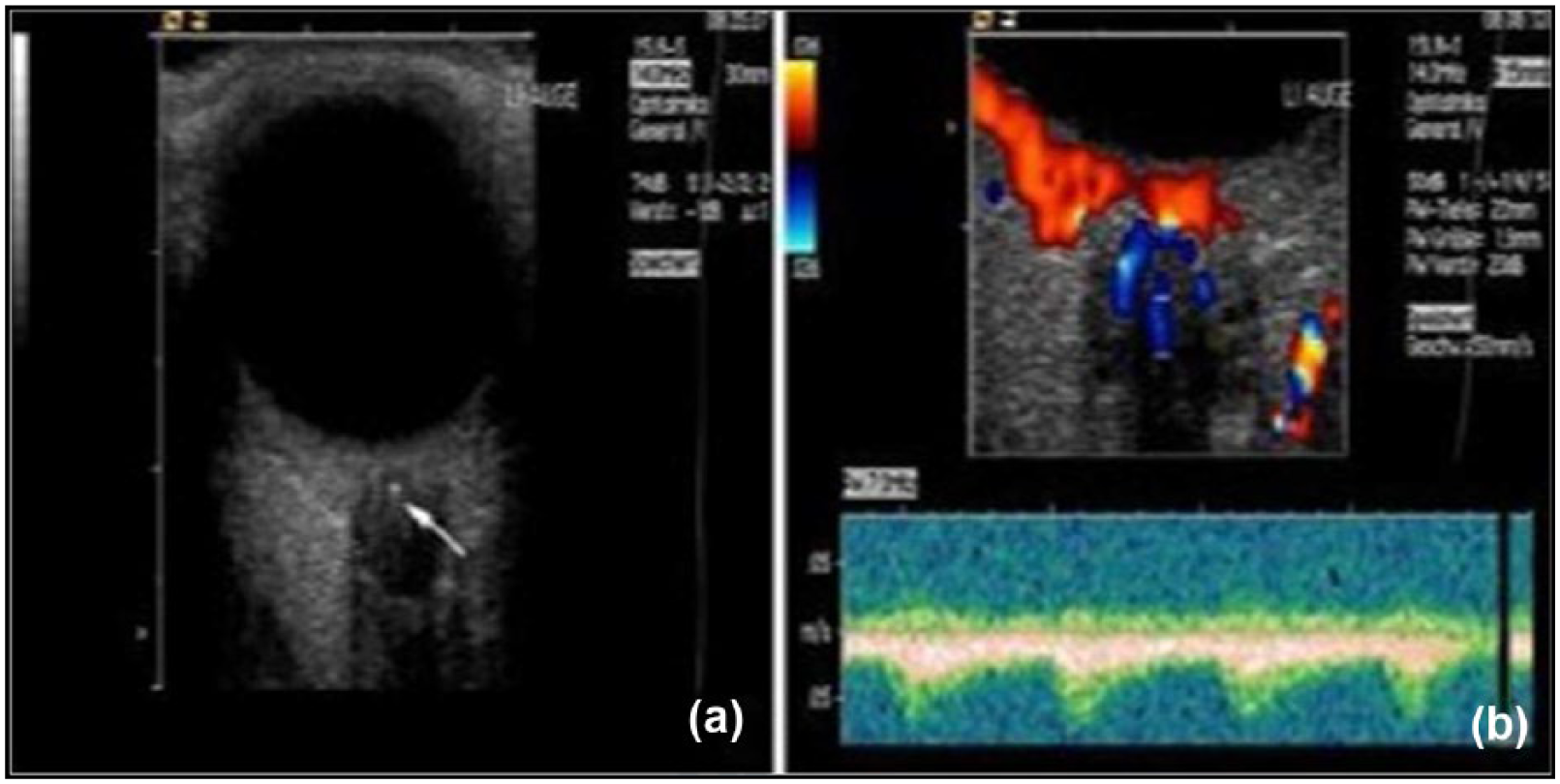
Sonography findings in a patient with embolic central retinal artery (CRA) occlusion. (a) B-mode: hyperechogenic “echogenic foci” in the optic nerve head (arrow), representing an embolus in the distal CRA. (b) Color and pulsed Doppler sonography: retrograde arterial flow in the CRA with persistent perfusion of the central retinal vein. 14
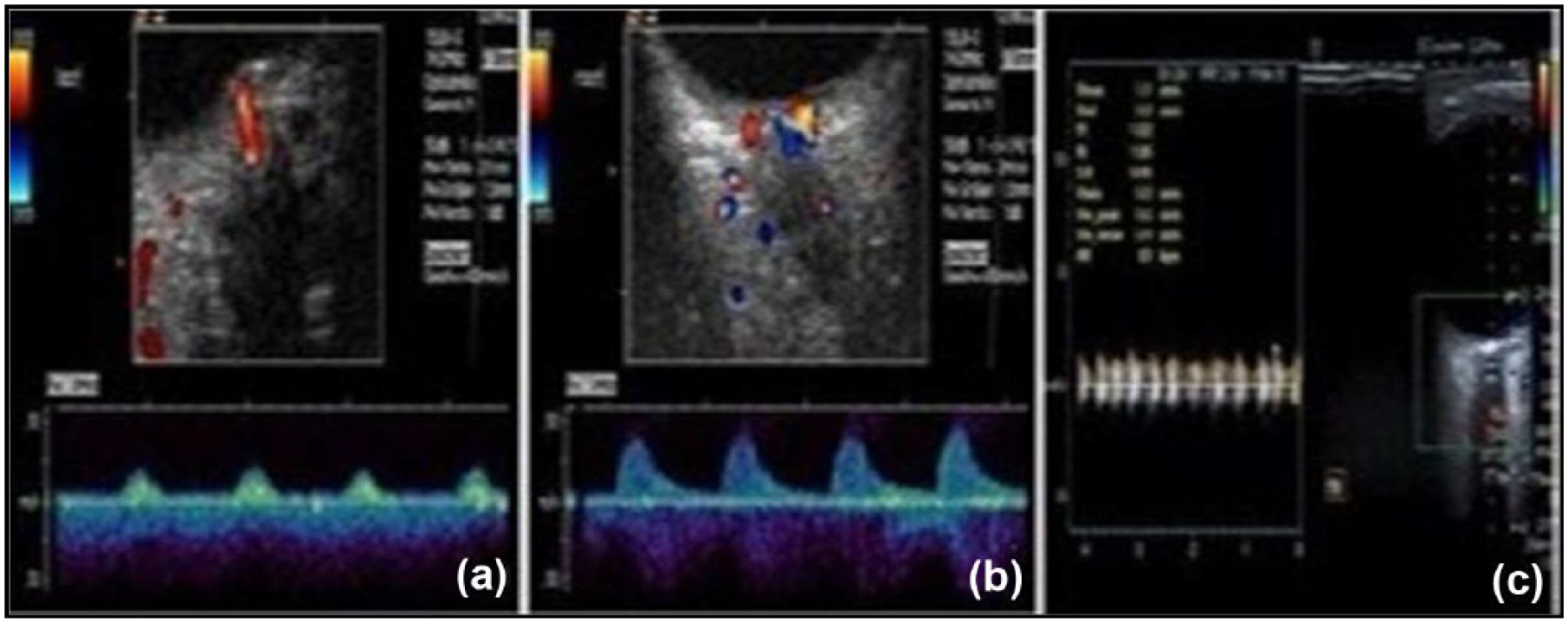
Sonographic findings in patients with central retinal artery (CRA) occlusion due to temporal arteritis. (a) Patient 1: color and pulsed Doppler sonography: Doppler gate detects arterial and venous flow in both the CRA and central retinal vein. (b) Patient 1: color and pulsed Doppler sonography: normal flow in the unaffected contralateral CRA. (c) Patient 2: color and pulsed Doppler sonography: lack of flow detected in the affected CRA. 14
This study was designed with the objective of evaluating the effect of age in CRA hemodynamics, in a convenience sample of healthy adult male participants, using color and pulsed Doppler spectral sonography.
Methods
Selection and Description of Participants
After receiving approval from the local ethics committee, a total of 100 consecutive healthy men were recruited and reported to the Department of Radiology and Medical Imaging, College of Applied Medical Sciences, Prince Sattam bin Abdulaziz University, Al-Kharj, Saudi Arabia. They were recruited for a period of nine months between December 2015 and August 2016 as part of this research study. A waiver of informed consent was granted in accordance with institutional guidelines. Before starting the Doppler sonography examination to interrogate the CRA, all participants underwent standard physical and ophthalmologic examinations. In addition, to ensure the credibility of the obtained results, very strict exclusion criteria were followed, which were the existence of one of the following conditions in participants: cardiac arrhythmia, heart failure (dyspnea at rest, paroxysmal nocturnal dyspnea, orthopnea, pulmonary effusions), acute or chronic arterial hypertension (systolic blood pressure > 150 mm Hg, diastolic blood pressure > 95 mm Hg), current and former smokers, chronic alcohol abuse (> 40 g/day), all types of diabetes mellitus (fasting serum glucose > 126 mg/dL on two independent determinations), ocular hypertension (> 20 mm Hg) or glaucoma, history of cerebral infarction or transient ischemic attacks, presence of substantial extracranial carotid artery disease, and the use of vasoactive (vasodilator or vasoconstrictor) medications. The exclusion criteria followed in this study were similar to the criteria applied by Kaiser et al. 4 and Muraoka et al. 11
CRA Color Doppler Protocol
All color Doppler sonography examinations were performed in a supine position in a thermally controlled room (26°C, or 78°F) by the same sonographer. Doppler examination for the CRA was performed on all of the participants with a linear-array transducer (10-15 MHz) connected to Hitachi (HI VISION Avius) ultrasound equipment. For efficient and accurate diagnosis of the sonography images, the appropriate time gain compensation (TGC) and dynamic range (DR) control of pulse echo signals were automatically set by the system and/or manually adjusted by the sonographer to obtain the desired image quality. The TGC was used for compensating the attenuation of ultrasound echo signals along the depth, and the DR was for controlling the image contrast resolution, for example, to increase the ability to distinguish between different echo amplitudes of adjacent structures. Acoustic coupling gel was applied to the external surface of the eyelids. Consistently, the right eye of each participant was selected and imaged; however, no pressure was applied to the eye during measurement. The examination began with locating the optic nerve, which provides a useful landmark for identification of several retrobulbar vessels. The flow toward the transducer was coded red and the flow away from the transducer was coded blue. The right CRA was interrogated in each of the participants. The CRA was detectable within the retrolaminar portion of the optic nerve (Figure 5) at approximately 25 mm; in this region, the vessel maintains a straight course, so angle correction was readily applied. The size of the sample volume was set at 1 mm and centered to the depicted artery.
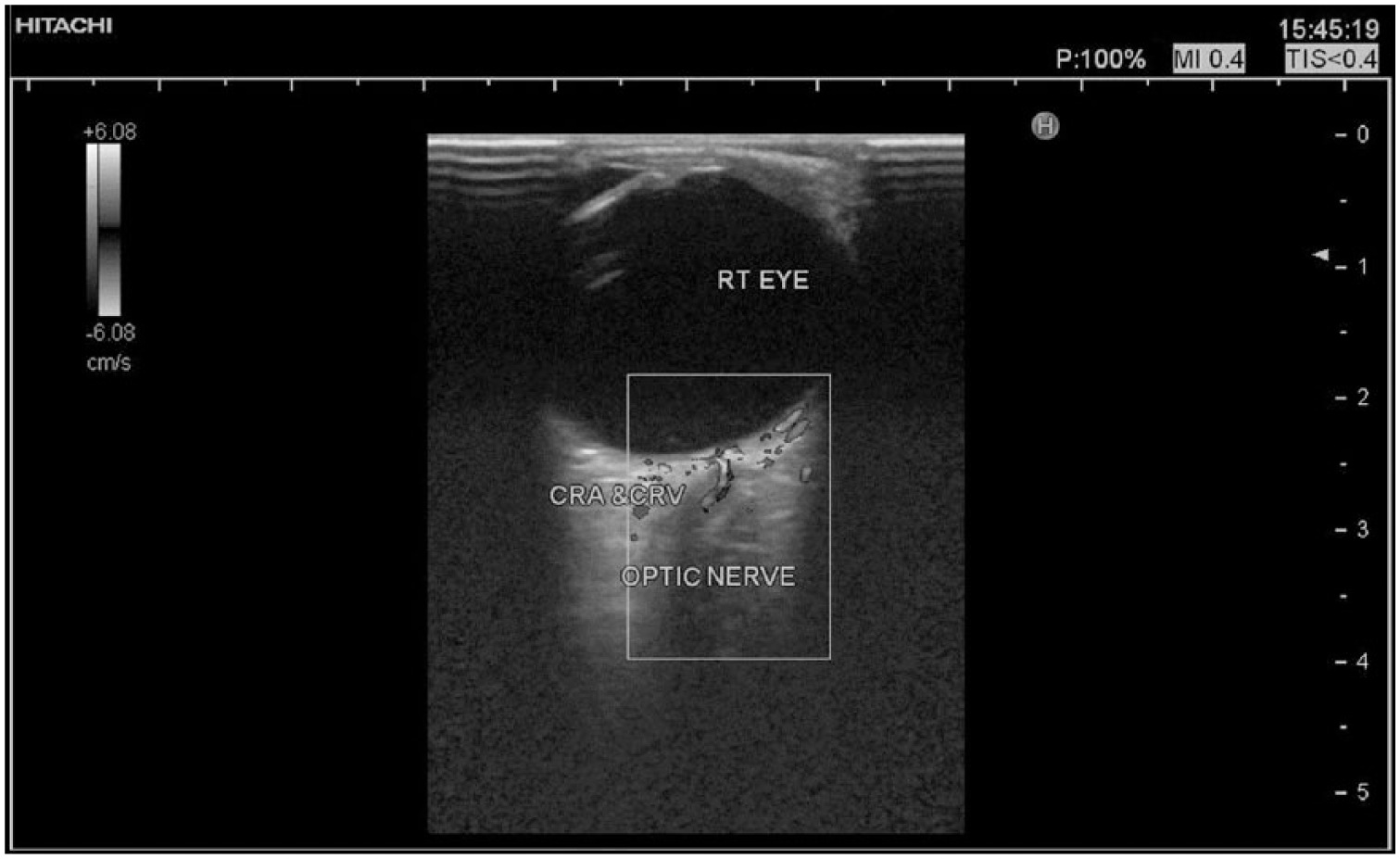
Color Doppler sonogram of the right central retinal artery (CRA) and central retinal vein (CRV) within the retrolaminar portion of the optic nerve. The values of the thermal index and mechanical index were maintained at < 0.4 and 0.4, respectively.
All measurements were performed with correction for the angle of insonation. This was achieved by aligning the electronic cursor on the display parallel to the direction of blood flow in the insonated artery. The angle correction for the CRA (angle between the Doppler beam and the long axis of the vessel) was always less than 60º for maximum Doppler shift (Figure 6). The PSV (cm/s) and the EDV (cm/s) were obtained by automatic tracing of the maximum frequency envelope of the Doppler waveform over a completed sweep of four cardiac cycles (Figure 7). Using the formulae provided by Pourcelot
15
and Gosling and King,
16
respectively, RI and PI were calculated, where
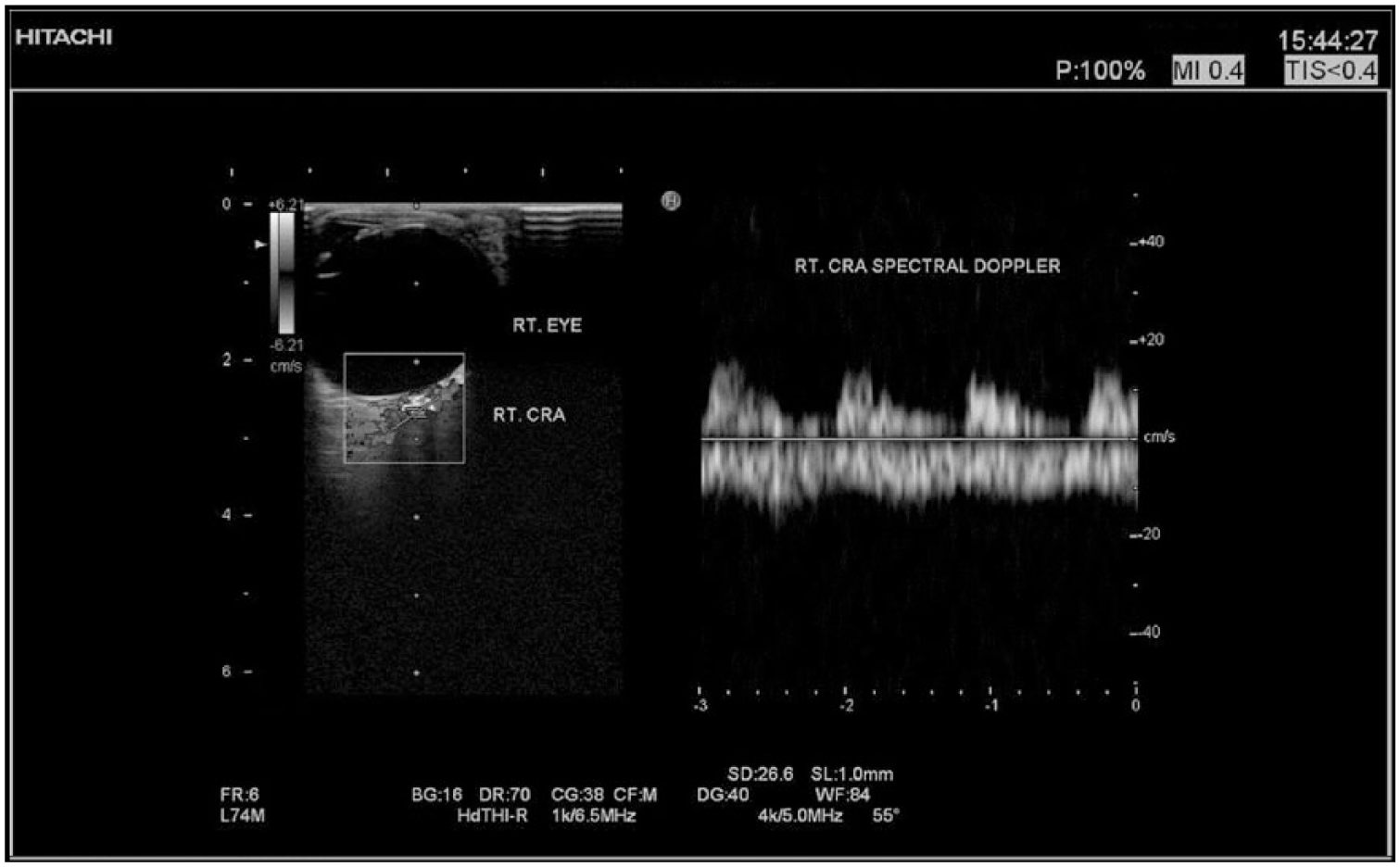
Right central retinal artery (CRA) spectral Doppler sonogram, where the electronic cursor aligned parallel to the direction of blood flow. The angle correction was 55º for maximum Doppler shift. The size of the sample volume was set at 1 mm and centered to the artery.
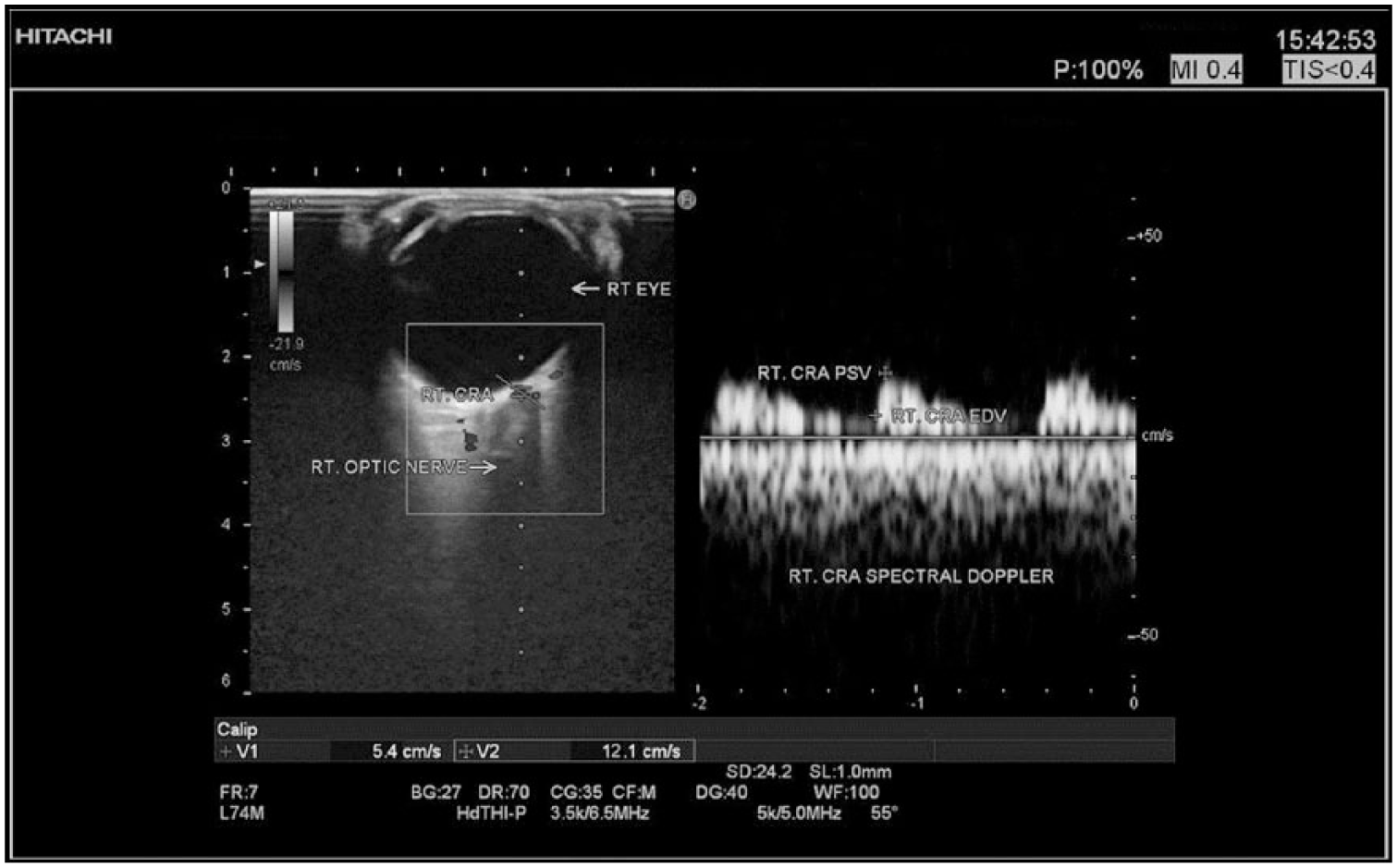
Sample spectral Doppler sonogram demonstrating the peak systolic velocity (PSV) (cm/s) and the end diastolic velocity (EDV) (cm/s) in a selective right central retinal artery (CRA).
Doppler Instrumentation Parameters for the CRA
The image controls that affect the color Doppler detection, within the CRA, were output power, overall gain, frequency selection, velocity, scale/pulse repetition frequency, region of interest, and focus, whereas output power, overall gain, velocity, scale/pulse repetition frequency, and gate size were the most salient factors that affected the appearance of spectral Doppler tracings within the CRA. 17
In this study, the Doppler instrumentation settings to interrogate the CRA were concentrated on the following: (a) As CRA color and spectral Doppler used high levels of output power, attention was paid to the safety indices. Power and gain were set so that clear spectral tracings were obtained. (b) The CRA color Doppler images required higher frequencies in order to detect low flow and to achieve better spatial resolution. (c) In CRA color and spectral Doppler, a low pulse repetition frequency was used to examine low velocities and to avoid aliasing that might occur if high velocities were encountered. (d) Since more pulses were needed to interrogate the CRA, with color Doppler, reduction of the width and maximum depth of the region of interest was applied to improve frame rate. It also allowed for a higher color scan line density and associated improved spatial resolution. (e) While scanning the CRA with color Doppler, the focal zone was adjusted to the area of interest. This made a significant difference in the appearance and accuracy of the image. (f) The CRA spectral Doppler was conducted for participants by using an appropriate gate size, since a larger gate size could include unnecessary signals from adjacent vessels.
Considerations for Performing the Doppler Examination of the CRA
To confirm imaging safety procedures specific to the eye, ultrasound bioeffects guidelines were applied such as the initial output power, exposure time, stationary probe technique, and Doppler modes. The initial output power settings for the ultrasound equipment used during the imaging of the eye were defaulted to the low power setting. The output power was increased during the investigation only if deemed necessary to produce a satisfactory result. Also, the overall examination exposure time for each case was kept as short as possible and produced a diagnostic result. The ultrasound transducer used for evaluating the eye was not held in a fixed position for any longer than was necessary. It was also removed from the participant’s eye whenever there was no need for imaging or Doppler acquisition. For example, the freeze frame or cine loop was used to allow review and discuss images without adding acoustic exposure. Varied Doppler modes were used to investigate the CRA, since pulsed Doppler techniques generally involve greater temporal average intensities and powers and the associated potential for heating the tissue. In addition, high duty factors were used given that high pulse repetition frequencies were needed. Thus, the use of spectral pulsed Doppler, or color Doppler mode with a narrow write zoom box, was not applied for the investigation of ocular structures, especially the CRA, without the thermal index and mechanical index continuously being monitored during scanning. The recommended values for both thermal index and mechanical index in this case were < 0.4 and 0.4 to 0.6, respectively.
These specific considerations for performing Doppler examination of the CRA were informed by both the American Institute of Ultrasound in Medicine consensus statements about mechanical ultrasonic bioeffects and the guidelines for the safe use of diagnostic ultrasound equipment developed by the British Medical Ultrasound Society.18,19
Statistical Analysis
Data were initially summarized as mean and standard deviation (SD) in the form of comparison tables. Range, mean, and standard deviation across participants were calculated for age and CRA PSV, EDV, RI, and PI. Student t test (unpaired t test) was used when comparing between means, participants’ mean age, and CRA spectral Doppler mean parameters. Pearson’s correlation coefficient (r) was used to evaluate the relationships between the CRA spectral Doppler parameters and age, where the value r = 1 means a perfect positive correlation and the value r = −1 means a perfect negative correlation; the P value was used for the significance of the results. The results were considered significant when P was < .05. Statistical analysis was performed using the standard Statistical Package for the Social Sciences (SPSS Inc., Chicago, IL, USA), version 20 for Windows.
Results
In this prospective study, a total of 100 consecutive and healthy men were recruited. The mean (SD) age was 43 (2.1) (range, 14-64) years. The CRA PSV ranged from 6.9 to 12.7 cm/s among participants (Table 1).
Values for CRA PSV and CRA EDV Within Different Age Groups.
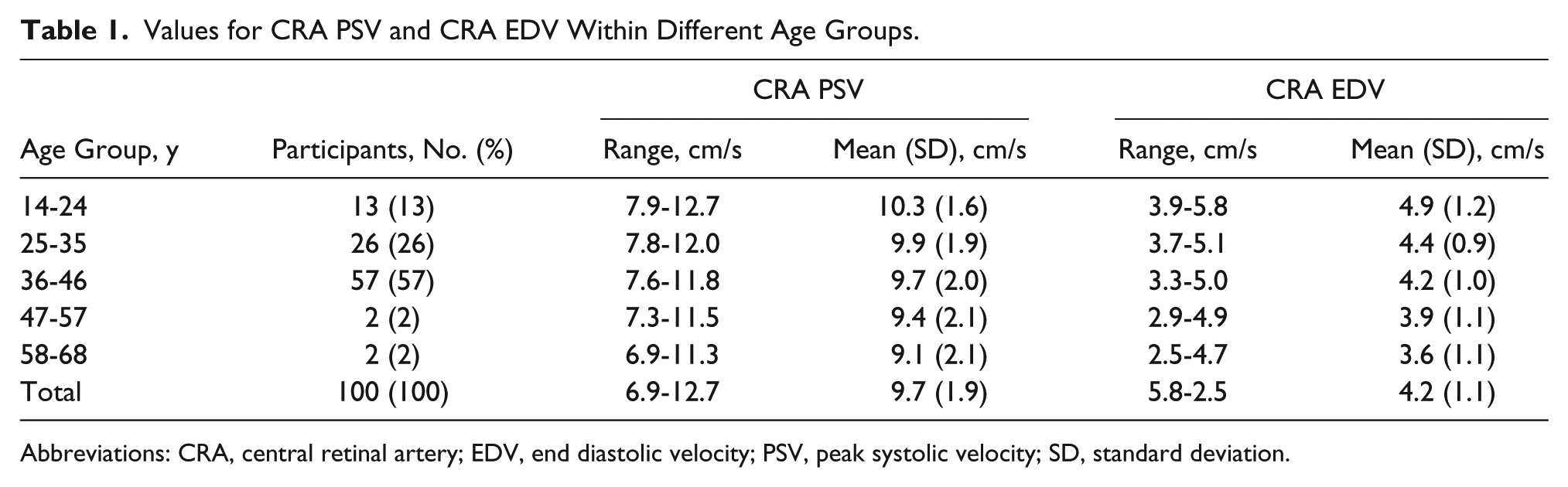
Abbreviations: CRA, central retinal artery; EDV, end diastolic velocity; PSV, peak systolic velocity; SD, standard deviation.
The values for CRA RI and CRA PI across different age groups are presented in Table 2.
Values for the CRA RI and CRA PI Across Different Age Groups.
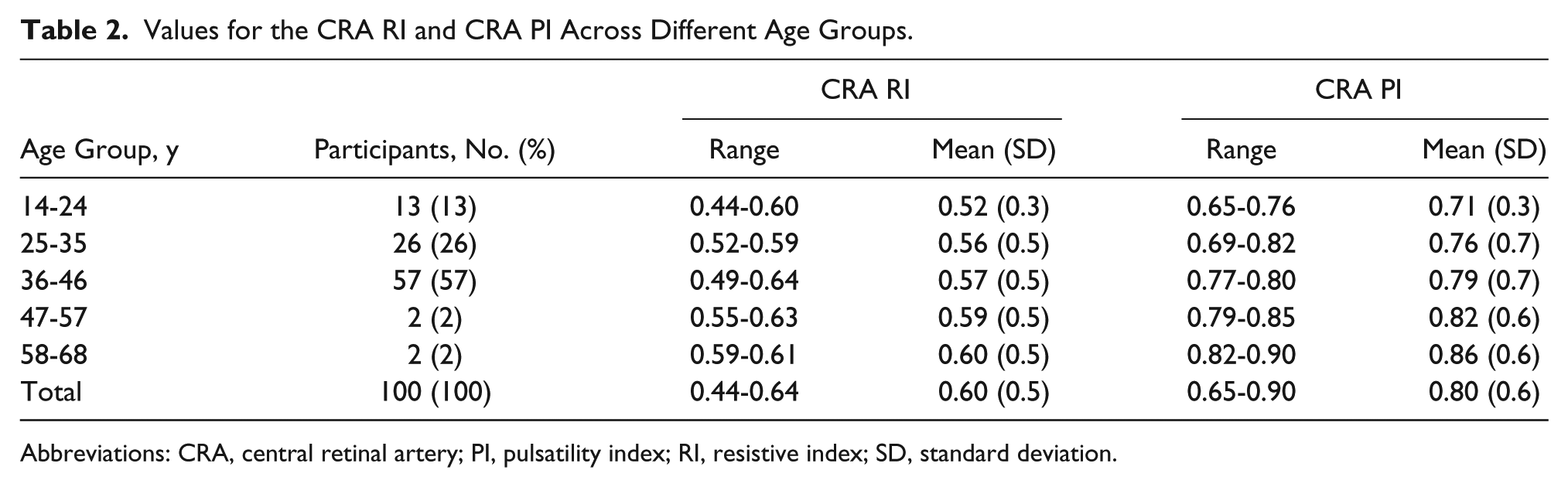
Abbreviations: CRA, central retinal artery; PI, pulsatility index; RI, resistive index; SD, standard deviation.
A statistically significant and highly negative correlation (P < .0001) was noted between participant mean age and mean PSV and EDV of the CRA (t = 117.6 and 163.7; r = −1.00 and −1.00, respectively) for each (Table 3). Another statistically significant highly positive correlation (P < .0001) was detected between participant mean age and the mean of CRA RI and CRA PI (t = 196.4 and 193.2; r = 1.00 and 1.00, respectively) (Table 4).
Correlations to Determine the Strength of Association Between Mean Participant Ages Compared to CRA PSV and CRA EDV.
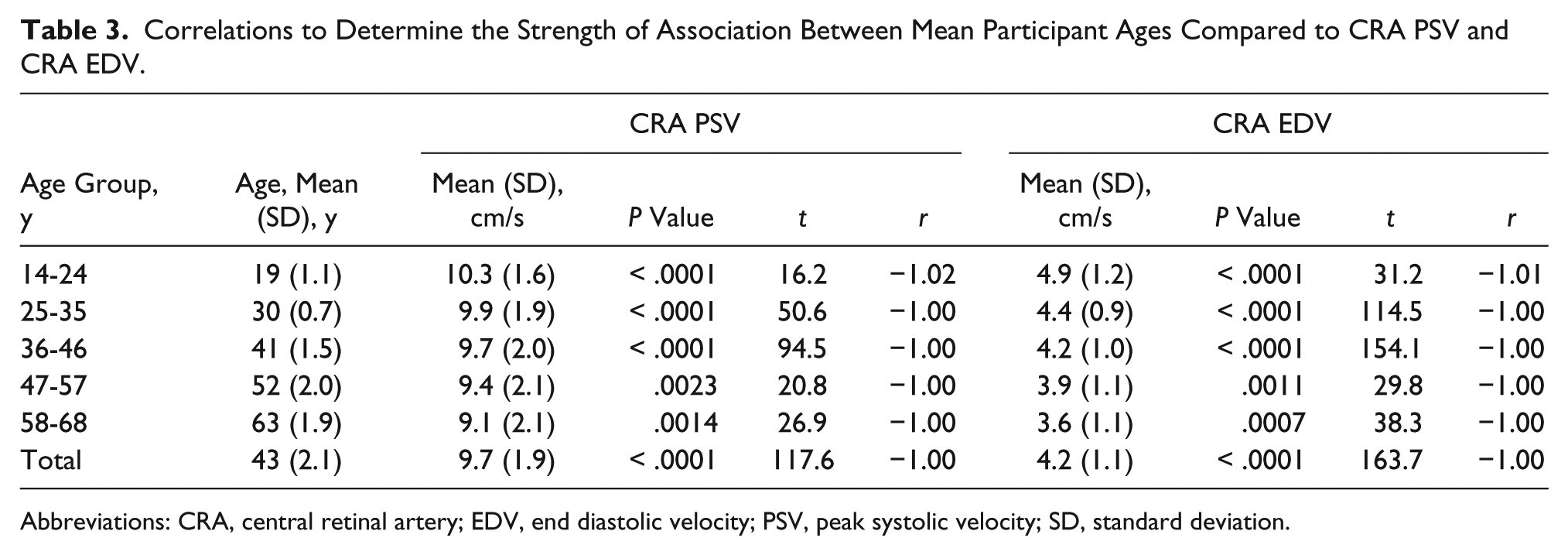
Abbreviations: CRA, central retinal artery; EDV, end diastolic velocity; PSV, peak systolic velocity; SD, standard deviation.
Correlations to Determine the Strength of Association Between Mean Participant Ages Compared to CRA RI and CRA PI.
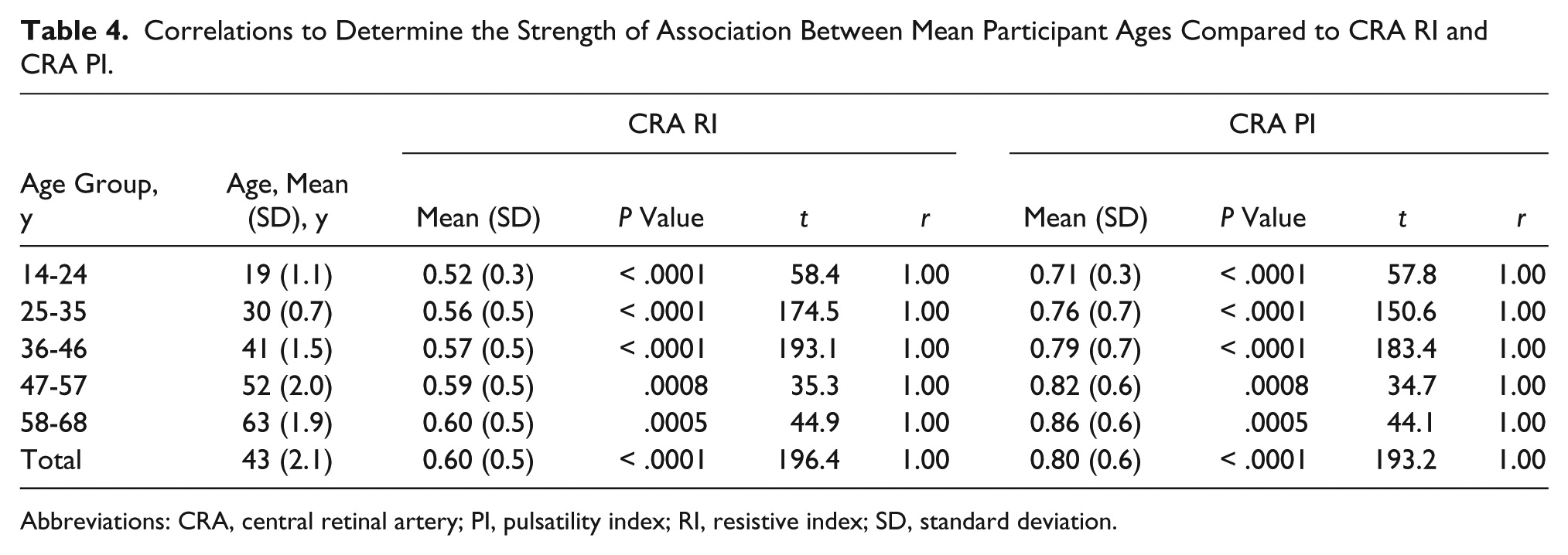
Abbreviations: CRA, central retinal artery; PI, pulsatility index; RI, resistive index; SD, standard deviation.
Discussion
This study provides normal intervals and ranges for the CRA blood flow detected with Doppler in a convenience sample of 100 healthy adult male participants (Tables 1 and 2). The study showed that CRA blood flow Doppler parameters are significantly age dependent (Tables 3 and 4). Therefore, an improvement in diagnostic accuracy of sonography might be obtained if the results of sonographic examination for the CRA could be compared to normal intervals specific for a participant’s age.
Several published studies have been inconsistent with respect to age and gender dependency of CRA Doppler blood flow parameters.3,4,20,21 However, the existence of such dependency due to the effect of a participant’s age on CRA hemodynamics (Tables 1 and 2) could improve the diagnostic accuracy of Doppler sonography, especially during a clinical evaluation. It is well known, however, that blood flow in major arterial beds decreases with age.22,23 This may be due to, but not limited by, an age-related decrease in cardiac output, an increase in peripheral vascular resistance, or both acting together.22,24 The Doppler frequency waveform is shaped not only by downstream organ resistance and cardiac function but also by fluid inductance and the compliance of arterial walls. These factors are essential components of the vascular impedance in a nonsteady state flow system of a body organ. 24
This cohort study demonstrated an increase in CRA Doppler indices as participants’ age increased (Table 2). It is reasonable to assume that microvascular constriction significantly increases the resistance met by blood flowing from arteries supplying the microvasculature.25,26 Wong et al. 27 provided evidence that the diameter of retinal arterioles decreases with increasing age. This decrease is estimated to be about 2.1 µm for each decade increase in age, which would result, on average, in a 21% resistance increase from the age of 20 to 80 years. 27 Regarding obtained results, the observed changes in the CRA RI and CRA PI were of similar magnitude.
In the current study, a statistically significant correlation (P < .0001) was noted among participants’ mean age and the mean of different Doppler parameters of the CRA (Tables 3 and 4). The same findings were obtained by Ustymowicz et al. 13 in a study of normal reference intervals and ranges of side-to-side and day-to-day variability of ocular blood flow Doppler parameters. They found that the probabilities (P) for slope were P = .062 and P = .001 for CRA PSV and CRA EDV, respectively, whereas P < .001 for CRA impedance indices when age of participants increases. 13
The current study adds to the body of knowledge, given that it is one of the recent studies that relates to the effect of age on CRA hemodynamics. It is also important to note that previous studies were conducted more than 20 years ago; therefore, the sensitivity and effectiveness of the ultrasound equipment are questionable. Clinicians have examined a variety of male and female patient age groups (14-64 years); however, this study was centered on adult male patients. This study also does not address the effect of younger age (< 14 years) on the CRA’s hemodynamics. More research is needed with current ultrasound equipment to better inform clinicians who are examining patients with compromised vascularity in the eye.
Limitations
The research design used has threats to internal and external validity; therefore, these results can be applied only to this cohort of participants. Despite the limitations of the research design and the lack of statistical power, the findings were similar to those published by Kaiser et al., 4 Ustymowicz et al., 13 and Williamson and Harris. 20 Another limitation of this study is that the age group of 36 to 46 years had the most participants (57%) compared to the other age groups (Tables 1 and 2), which reduces the effect of the conclusions. Further studies should consider randomized assignment of participants and a powered statistical study that has varied age and gender for maximum translational quality.
Conclusion
In conclusion, spectral and color Doppler sonography is a feasible noninvasive technique that can be used to evaluate the blood flow velocities in the CRA. This study provides results regarding the CRA spectral Doppler parameters of normal blood flow velocities in a cohort of healthy men. For this cohort, Doppler sonography distinguished variations in blood flow velocities compared to a participant’s age. These research findings to evaluate the effect of age were specific to flow taken only in the right CRA. This is a limiting factor and future studies should attempt to take vascular flow measures bilaterally. Based on these limited results, it appears feasible and worth further investigation to match age groups with sonographic data as a prerequisite for clinically useful interpretations. Thus, additional studies to evaluate changes that may occur in hemodynamics of the CRA among younger ages (< 14 years) may be of some use. The bioeffects of such a pediatric study would need to be carefully considered.
Footnotes
Acknowledgements
The author would like to thank the volunteers from Prince Sattam bin Abdulaziz University, Prince Sattam bin Abdulaziz University Hospital, and King Khalid Hospital and Prince Sultan Center for Health Services, without whom this study would not have been possible.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.