
Abstract
Compartment syndrome occurs when excessive pressure builds up inside an enclosed muscle space in the body. The dangerously high pressure in compartment syndrome impedes the flow of blood to and from the affected tissues. It can be an emergency, requiring surgery to prevent a permanent injury. In this case study, a lower extremities venous examination was performed on a male patient suspected of having compartment syndrome, as an incidental finding. Sonographic evaluation of the right leg revealed the absence of popliteal and small saphenous veins, and acute thrombus in the posterior tibial veins. The evaluation further revealed an incidental finding of double pseudo-aneurysm in the popliteal fossa, which was suspected for increasing the excessive compartmental pressure. This unique case study presents sonographical evaluation strategies when compartment syndrome is suspected.
Keywords
Compartment syndrome occurs when there is a significant buildup pressure within a fascia. Since the fascia cannot expand much with the exertion of the added pressure buildup, it results in the compression of the vein, artery, and nerve residing within that fascia. A reported annual incidence of acute compartment syndrome is 0.7 to 7.3 per 100,000 cases (0.0007%–0.0073%). 1 While the incidence rate is very low, depending on the severity of a case, the result can be detrimental. It can lead to permanent damage, as well as loss of a limb, without medical intervention, and this needs to be found within a few hours from the onset of symptoms. 2 Among the many symptoms of compartment syndrome, pain is the most common symptom associated with compartment syndrome, 1 which is also a common indication for ordering a venous duplex study. Therefore, the sonographer plays a crucial role in detecting the presence of compartment syndrome. This case study exemplifies the possible indications, or clues, to sonographers who suspect compartment syndrome.
Case Report
The patient is a 67-year-old man who underwent a total right knee replacement 2 days prior to the duplex venous study. During the assessment, the patient presented with symptoms that included pain, swelling with redness, and numbness with a burning sensation in the right calf. The physician ordered a lower extremity venous duplex examination since some of the symptoms associate with thrombus formation.
The venous duplex was performed following the lab’s specific imaging protocol. The common femoral, femoral, profunda femoral, popliteal, small and great saphenous, posterior tibial, peroneal and soleal sinus veins were examined. The images showed acute occlusive thrombus in the posterior tibial veins (Figure 1). The popliteal and small saphenous veins were not visualized which was very unusual because the popliteal vein was a major vein to carry the blood back to the inferior vena cava. There was not a collateral vein that connected the venous system in the calf to the thigh (Figures 2 and 3). Since it was crucial to have a patent venous system to return the blood back to the inferior vena cava from the lower extremity, the popliteal fossa was investigated thoroughly. Further interrogation revealed an incidental finding of double pseudo-aneurysm with to-and-flow blood flow arising from the popliteal artery (Figure 4). The first sac was 3.4 cm long and located posterior to the popliteal artery, and the second sac was 4.7 cm long and located anterior to the popliteal artery. Since veins could be easily compressed with small amount of external pressure, it was concluded that the popliteal and small saphenous veins must have been compressed by the two pseudo-aneurysmal sacs. The compression of the popliteal and small saphenous veins also provided a plausible explanation for the thrombus formation in the posterior tibial veins. The thrombus found in the posterior tibial veins most likely resulted due to venous stasis. Doppler waveforms of the distal posterior tibial and peroneal arteries at the ankle level were not imaged at the time of the venous duplex study because the patient was in a distressed stage. However, according to the vascular surgeon’s note at the time of the surgery, they were documented to be monophasic, which were abnormal Doppler waveforms. The patient’s symptoms of numbness, tingling, and limited range of motion most likely resulted from the compression of the nerve in the same fascia.
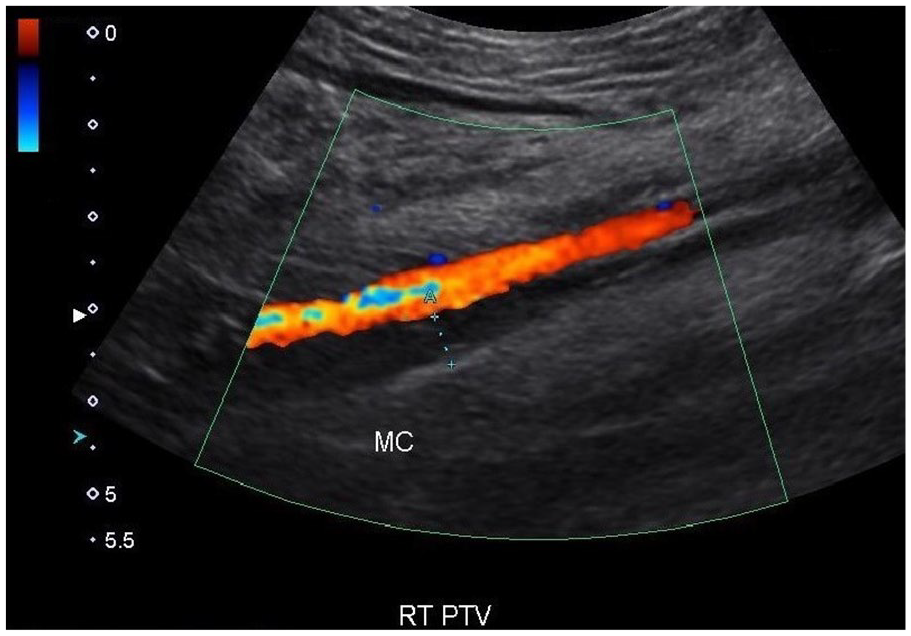
The color Doppler image of the acute thrombus in the posterior tibial vein.
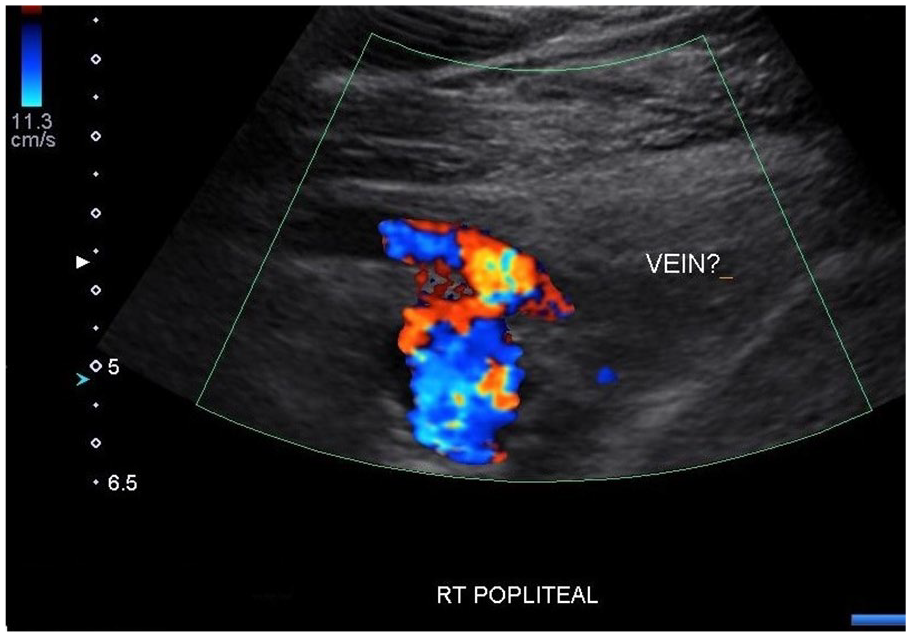
The pseudo-aneurysmal sac posterior to the popliteal artery. The popliteal vein was not identified.
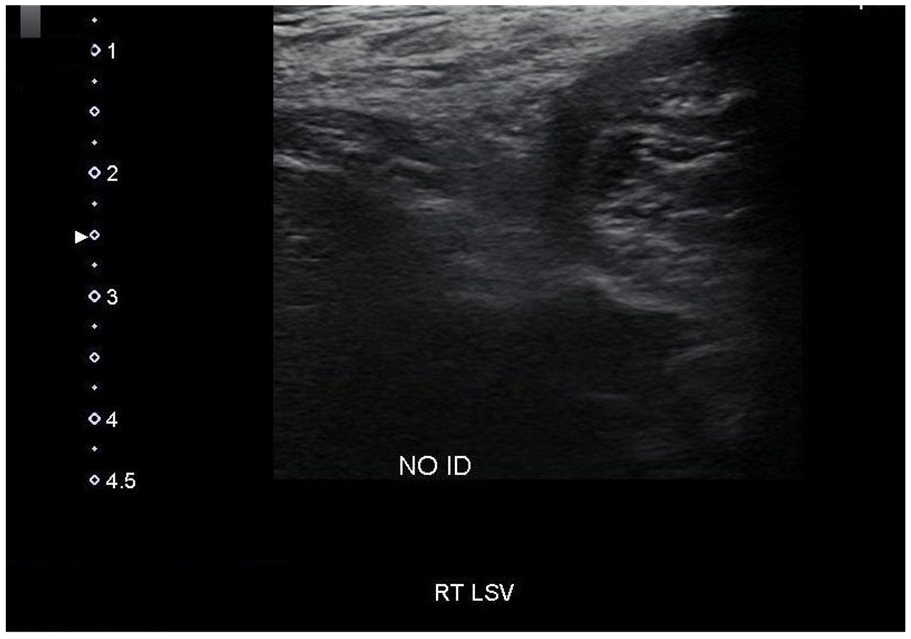
The small (lesser) saphenous vein is not identified on this gray-scale sonographic image.
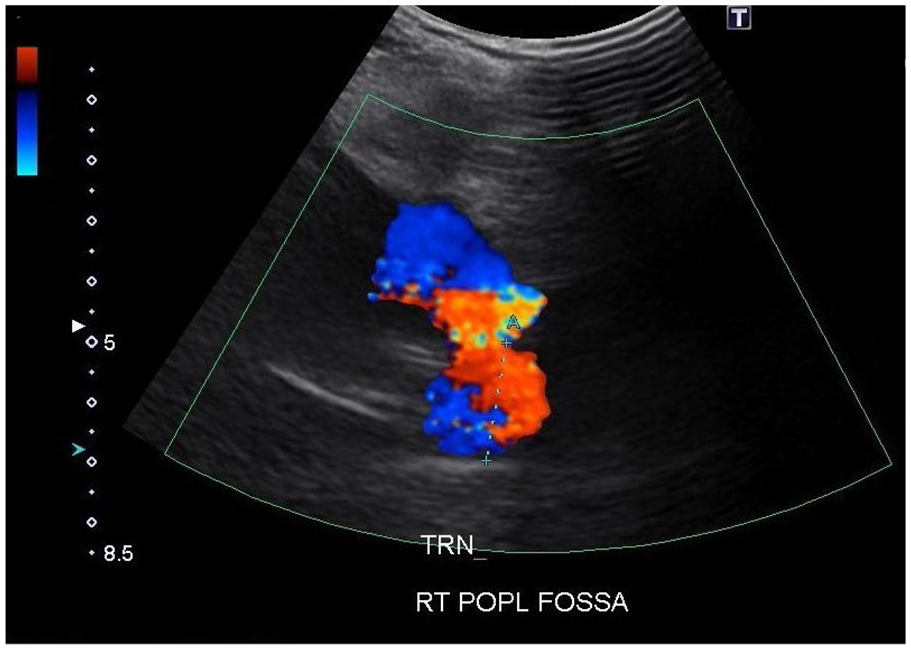
A transverse sonographic view of the popliteal artery with double pseudo-aneurysmal sacs.
Upon the completion of the venous duplex study, the ordering physician was notified of the results and the incidental finding, which led to a consult from a vascular surgeon. The vascular surgeon suspected compartment syndrome upon his evaluation and ordered a vein mapping study. The patient was taken into an operating room within 2 hours to treat the double pseudo-aneurysm and the resultant compartment syndrome. According to the vascular surgeon’s note, incision into the popliteal fossa showed that the anterolateral compartment, in particular, appeared to have some non-viable tissue, and there was a large hole behind the knee, possibly from a rupture of the double pseudo-aneurysmal sacs rising from the popliteal artery. Since placing a bypass graft from the distal femoral/proximal popliteal artery to the distal tibioperoneal trunk would be the best choice to bypass the ruptured area, the patient underwent a bypass graft placement surgery.
The follow-up arterial examination that was performed 8 months after the fem-tibioperoneal bypass surgery showed normal ankle-brachial indices and normal arterial Doppler waveforms at rest bilaterally. The ankle-brachial index and arterial Doppler waveform post exercise in the right leg showed minimal ischemia. The thrombus in the posterior tibial veins in the right leg persisted but resolved 20 months later after the first venous examination.
Discussion
The lower leg is divided into four compartments by the interosseous membrane of the leg: the anterior, lateral, superficial posterior, and deep posterior compartments. 3 Compartments are groups of muscle tissue, blood vessels, and nerves in the arms and legs surrounded by a very strong membrane called the fascia. 4 Compartment syndrome usually results from bleeding or swelling after an injury, as it occurs when excessive pressure builds up inside the enclosed muscle space in the body. The dangerously high pressure in compartment syndrome impedes the flow of blood to and from the affected tissues. After an injury, blood or edema (fluid resulting from inflammation or injury) may accumulate in the compartment. The tough walls of fascia cannot easily expand, and compartment pressure rises, preventing adequate blood flow to tissues inside the compartment. It can be an emergency, requiring surgery to prevent a permanent injury. Severe tissue damage can result, with loss of body function or even death. 1 The symptoms of acute compartment syndrome are also known as five P’s: Pain, Passive stretch, Paresthesia, Pallor, and Pulse. Pain is the most common symptom associated with compartment syndrome, whether it is acute or chronic. As the muscle is lacking in blood, it will be highly sensitive to stretching. 5
The incidence of acute compartment syndrome is estimated to be 7.3 per 100,000 in males and 0.7 per 100,000 in females, with the majority of cases occurring after a trauma. 2 There are a few tests that can detect compartment syndrome or its related symptoms. According to the Mayo Clinic, magnetic resonance imaging (MRI) or near infrared spectroscopy (NIRS) can be used to evaluate the structure of the muscles in the compartment and rule out other possible causes of the symptoms. The NIRS measures the amount of oxygen in the blood in the affected tissue to determine if the muscle compartment has decreased blood flow. Also, advanced MRI imaging can help assess fluid volumes of the compartments during an exercise, which accurately detects chronic exertional compartment syndrome. If any of these tests do not produce conclusive results, a gold standard test called compartment pressure measurement is suggested for diagnosing chronic exertional compartment syndrome. Because this test is invasive and mildly painful, involving insertion of needles into the patient’s muscles, compartment pressure measurement usually is not performed unless the medical history and other tests strongly suggest the patient has the condition. 6
Treatments for nonoperative treatments, which include discontinuation of the activity that causes the condition, pain medication, physical therapy, orthotics, and massage, are suggested. Since the nonoperative treatments do not provide a lasting benefit, a surgical option, such as a fasciotomy, might be suggested. A fasciotomy is a surgical procedure which involves cutting open the inflexible tissue encasing each of the affected muscle compartments (fascia) to relieve the pressure. The complication of the surgery can include infection, permanent nerve damage, numbness, weakness, bruising, and scarring. 6
For the acute compartment syndrome, such as this case study, the only option is surgery, such as fasciotomy, due to its critical nature. 7 This patient subsequently underwent bypass graft placement surgery from the distal femoral/proximal popliteal artery to the distal tibioperoneal trunk as well, due to the hole in the popliteal artery. A leg vein mapping examination was ordered within the next hour, and the patient was taken in for surgery within 2 hours from the time the lower extremities venous duplex study was completed.
The double pseudo-aneurysm, which was not present upon incision into the popliteal fossa due to the rupture would have been the most suspected culprit for causing the acute compartment syndrome in this case study. In general, the treatment of pseudo-aneurysm varies on the size of the pseudo-aneurysmal sac. A watchful-waiting approach may be recommended if the size of the pseudo-aneurysmal sac is less than 2 cm. For the pseudo-aneurysm wider than 2 cm, or for the patient on anticoagulants, treatment with sonography-guided compression repair, or sonography-guided medication injection such as thrombin, or a surgery may be recommended. 8 The size of the larger pseudo-aneurysmal sac of the patient in this case study was 4.7 cm long. If the pseudo-aneurysm in this case study had been an isolated incident without a complication, a treatment of thrombin injection might have been suggested.
The follow-up arterial examination 8 months after the fem-tibioperoneal bypass graft surgery showed normal ankle-brachial indices and normal Doppler waveforms at rest. The ankle-brachial index and Doppler waveforms post exercise in the right leg showed minimal ischemia. The thrombus in the posterior tibial veins in the right leg persisted but resolved 20 months after the first venous examination.
Conclusion
Sonographic imaging is a widely used diagnostic tool to identify many medical conditions such as ischemia of arterial vasculature, cholelithiasis, or liver cirrhosis. This unique and unusual case study provides information and images acquired while the patient was suffering from compartment syndrome. The popliteal and small saphenous veins were not visualized due to the external compression by the double pseudo-aneurysmal sacs. The acute thrombus in the posterior tibial veins most likely resulted due to venous stasis. The arterial Doppler waveforms of the arteries at the ankle were not imaged at the time of the venous study due to the patient being distressed, but according to the vascular surgeon’s note, they were monophasic at the time of the surgery. The pressure buildup in the popliteal fossa at the time of the surgery must have been so strong that it compromised the arterial blood flow as well as venous blood flow. These sonographic findings can serve as clues to suspect compartment syndrome when combined with the patient’s history, especially when the patient complains of numbness and limited range of motion, which could be related to nerve issues as well. It is crucial for sonographers to be aware of the combination of these findings, and to use critical thinking skills since acute compartment syndrome is a serious emergency situation and requires a medical intervention. It is also very important for sonographers to investigate thoroughly when there is an unusual situation, such as incidental findings of double pseudo-aneurysm in this case study. As we expand the knowledge and usage of sonography, the field will grow and the role of sonographers would become even more essential and crucial as a part of the medical team.
Footnotes
Acknowledgements
I would like to thank Matt Smith, MS, RVT, for proof reading, and Marsha Neumeyer, BS, RVT, FSDMS, FSVU, FAIUM, for the encouragement, and especially for the tremendous help to improve the writing of this case study.
Author’s Note
Permission to use images has been granted for the purpose of education.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.