
Abstract
Objective:
A review of the anatomy of the synovial recesses of the knee is important to better understand the different effusion presentations, update the diagnosis criteria of knee effusion based on the measured synovial recesses and discuss the differentiation of some effused recesses from other lesions around the knee.
Method:
This review focuses on the anatomy of the synovial recesses of the knee and classifies them into three groups (anterior, parameniscal, and posterior recesses), as well as provides an overview on the etiology of knee effusion, its sonographic detection, and diagnosis criteria.
Results:
Knee effusion is a very common pathological finding in sonography of the knee. The unique joint structure of the knee provides the possibility to host complex synovial recesses. Fluid in some of the synovial recesses is valuable for the diagnosis of knee effusion, while in certain situations, some recesses may impose diagnostic uncertainty. Knowledge of these synovial recesses is essential to avoid diagnostic pitfalls.
Conclusion:
This review provides an important discussion of the differentiation of some recesses effusions from other lesions around the knee.
A knee effusion refers to an increased volume of fluid in the synovial compartments of the knee. It is the earliest sign of synovial disease of the knee and is also a very common pathological finding in sonography of the knee.1–3 Due to the unique joint structure of the knee, there are complex synovial recesses arising from the interconnected synovial compartments, which include central, medial, and lateral synovial compartments. Fluid in synovial compartments of the knee can move or accumulate in any of the recesses depending on the position of the knee and the fluid volume.4,5 The most recognizable synovial recess in the knee is the suprapatellar recess. Many other less noticeable recesses scattered in the knee are also clinically important as fluid in some of these recesses in certain situations can be crucial for the diagnosis of knee effusion. Furthermore, these recesses sometimes may appear cystic and therefore need to be distinguished from other lesions around the knee.6–8 Ultimately, knowledge of these synovial recesses of the knee is essential to avoid diagnostic pitfalls. Although most of the synovial recesses of the knee have been well depicted on magnetic resonance imaging (MRI),7–10 at this point, no article has systematically addressed the sonographic presentations of the synovial recesses of the knee and their associated effusion. The purpose of this article is to review the anatomy of the synovial recesses of the knee in order to help understand the different effusion presentations, update the diagnosis criteria of knee effusion based on the measured synovial recesses, and discuss the differentiation of some effused recesses from other lesions around the knee.
Anatomy of the Synovial Recesses of the Knee
The knee consists of three joints: the femorotibial, patellofemoral, and superior tibiofibular joint. 6 Since the superior tibiofibular joint is usually completely separated from the other two joints, the knee joint generally refers to the femorotibial and patellofemoral joints (see Figure 1A,B). The femorotibial joint is composed of medial and lateral compartments. The medial compartment is formed by the medial condyle of the femur and the medial plateau of the tibia, while the lateral compartment is formed by the lateral condyles of the femur and the lateral plateaus of the tibia. The medial and lateral articular surfaces of the tibia are covered by the medial and lateral menisci to provide depth to the surfaces (see Figure 1A). The patellofemoral joint is formed by the groove of the femoral trochlea and the articular facet of the patella (see Figure 1B). 6
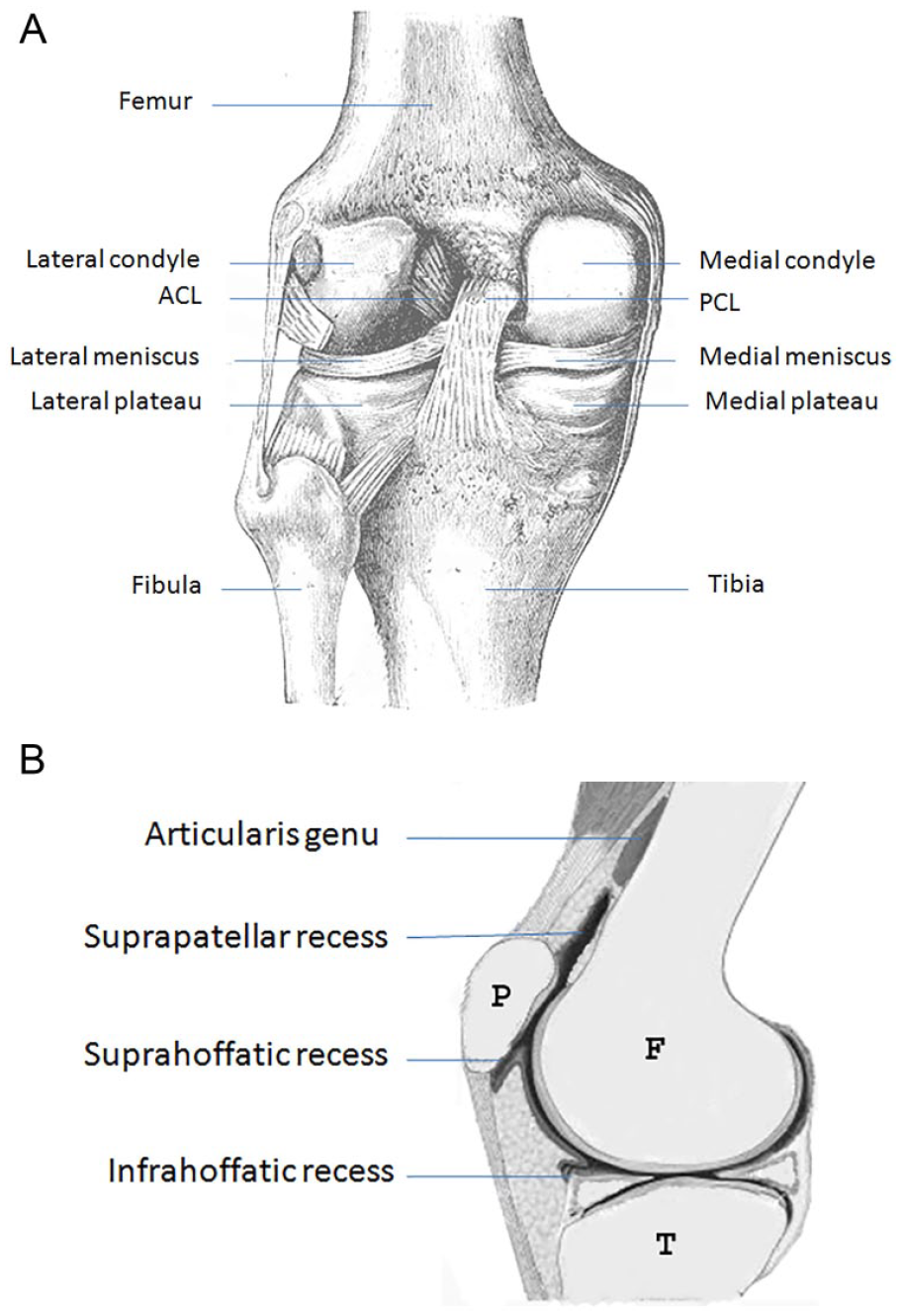
Knee joint: (A) posterior view of the femorotibial joint (modified from Gray’s anatomy of the human body, 1918); (B) sagittal view of the patellofemoral joint and related anterior recesses. F, femur; P, patella; T, tibia.
The knee joints are surrounded by an articular capsule, which consists of two layers, the thick outer fibrous membrane and the thin inner synovial membrane. The synovial membrane is responsible for the secretion of synovial fluid to lubricate and nourish the joints. 7 It lines the nonarticular portions of the joints and is the largest and most extensive synovial membrane in the body. This large synovial membrane forms interconnected recesses around the joints. According to their anatomical positions in the knee, they can be classified into three groups: the anterior, parameniscal, and posterior recesses.2,6–8
Anterior Recesses
The anterior recesses are the synovial recesses surrounding the patella in the anterior aspect of the knee, which include the suprapatellar recess, parapatellar recesses, and infrapatellar recesses.6–8 The synovial membrane attached to the patellar articular margins extends circumferentially to form a large cul-de-sac surrounding the patella.
The suprapatellar recess, also known as the subquadriceps recess, is the portion of the cul-de-sac located superior to the patella. It is situated beneath the quadriceps tendon but superficial to the lower part of the femur (see Figures 1B and 2A). There are two fat pads in the suprapatellar space. One is the suprapatellar pad, which is a small fat pad located superior to the patella and posterior to the distal third of the quadriceps tendon. Another is the prefemoral pad, which is a large fat pad located immediately superficial to the femur. 6 Therefore, more specifically, the suprapatellar recess is deep to the quadriceps tendon and the suprapatellar fat pad but superficial to the prefemoral fat pad (see Figures 1B and 2B). 2 Arising from the anterior surface of the femoral shaft, a small muscle called the articularis genu inserts superiorly into the synovial membrane of the suprapatellar recess (see Figure 1B). It stabilizes the recess by pulling it during knee extension and allows the patella to glide freely without friction over the femur. 7 The suprapatellar recess is the largest recess of the knee joint. It is formed from the fusion of the subquadriceps bursa with the joint cavity during fetal development.6,7
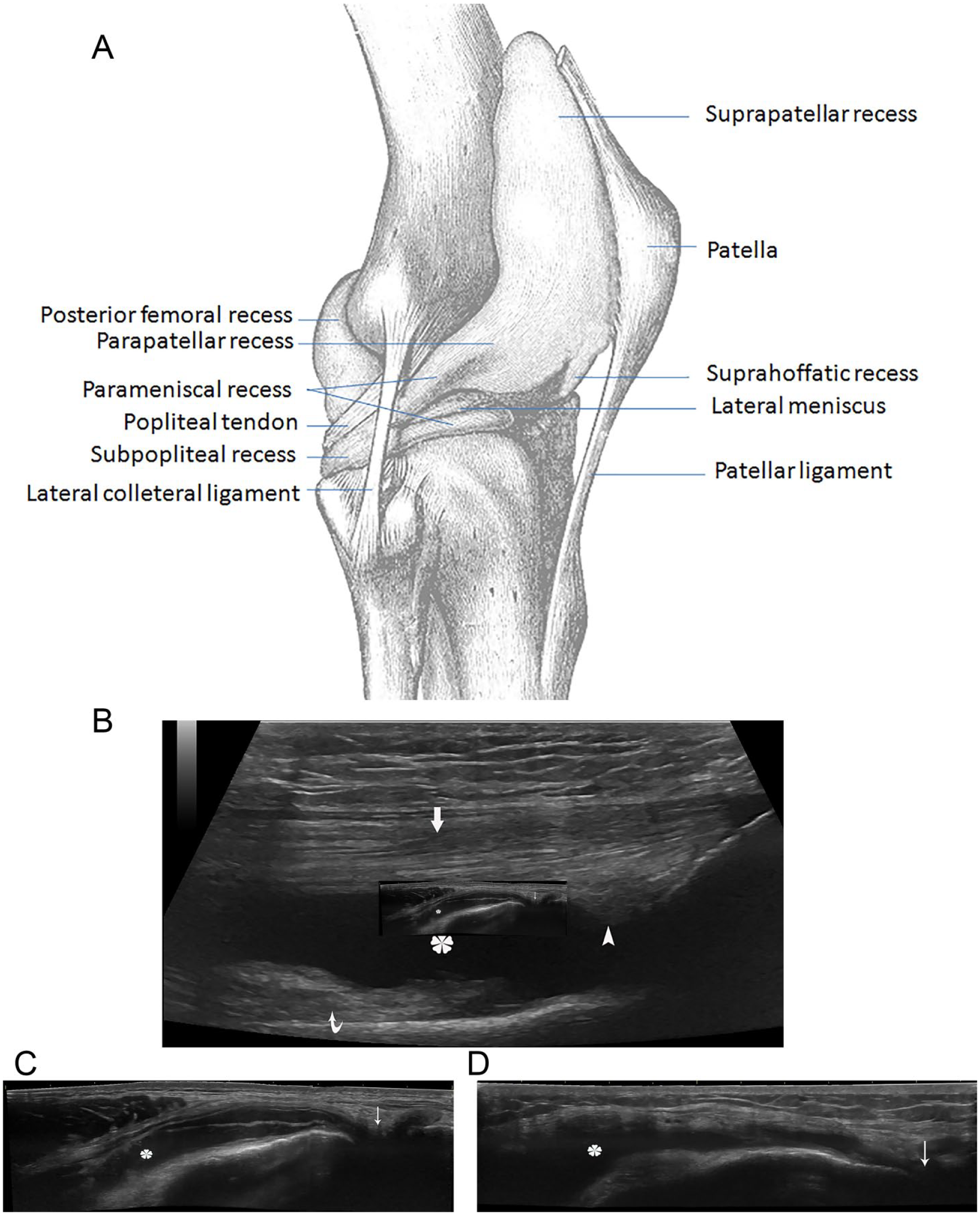
Suprapatellar recess and parapatellar recesses of the knee: (A) lateral view of the synovial recess of the knee (modified from Gray’s anatomy of the human body, 1918); (B) on sagittal view of sonography, the suprapatellar recess (asterisk) is deep to the quadriceps tendon (thick arrow) and the suprapatellar fat pad (arrowhead) but superficial to the prefemoral fat pad (curved arrow); (C) medial and (D) lateral parapatellar recesses on coronal view of sonography. The recesses (asterisk) extend downward to the menisci (thin arrow).
Parapatellar recesses are the portions of the cul-de-sac located medial and lateral to the patella. They lie underneath the aponeuroses of the vastus medialis and lateralis but superficial to the anterior femur.7,8 Therefore, both recesses are still in the anterior aspect of the knee but beside the patella. The synovial membrane on either side passes downward deep to the patellar retinacula to the meniscus (see Figure 2A,C,D).6,7
The infrapatellar recesses are the recesses in the infrapatellar space, including the suprahoffatic recess and the infrahoffatic recess (see Figures 1B and 2A).2,8,9 The infrapatellar space is filled with fat and vascular-rich tissue, called the infrapatellar fat pad, also known as Hoffa’s fat pat. Since it is in the joint capsule and superficial to the synovial joint cavity, it is an intracapsular but extrasynovial structure. The suprahoffatic recess is the small portion of the cul-de-sac located inferior to the patella but on the superior aspect of Hoffa’s fat pad. It is vertically orientated (see Figure 3A,B). The infrahoffatic recess is a horizontal recess inferiorly located in Hoffa’s fat pad. It is the synovial reflection at the anterior edge of the menisci. It is anterior to the anterior cruciate ligament (ACL). 8 Its shape can be linear, pipe-like, globular, or ovoid on transverse images (see Figure 3C,D). 9 Not all patients with knee effusion are necessarily having infrapatellar recesses. About 71% have the suprahoffatic recess while 45% have the infrahoffatic recess. 9 Based on the author’s experience, the infrahoffatic recess is sonographically more commonly seen than the suprahoffatic recess. Sometimes both recesses can be seen at the same time.
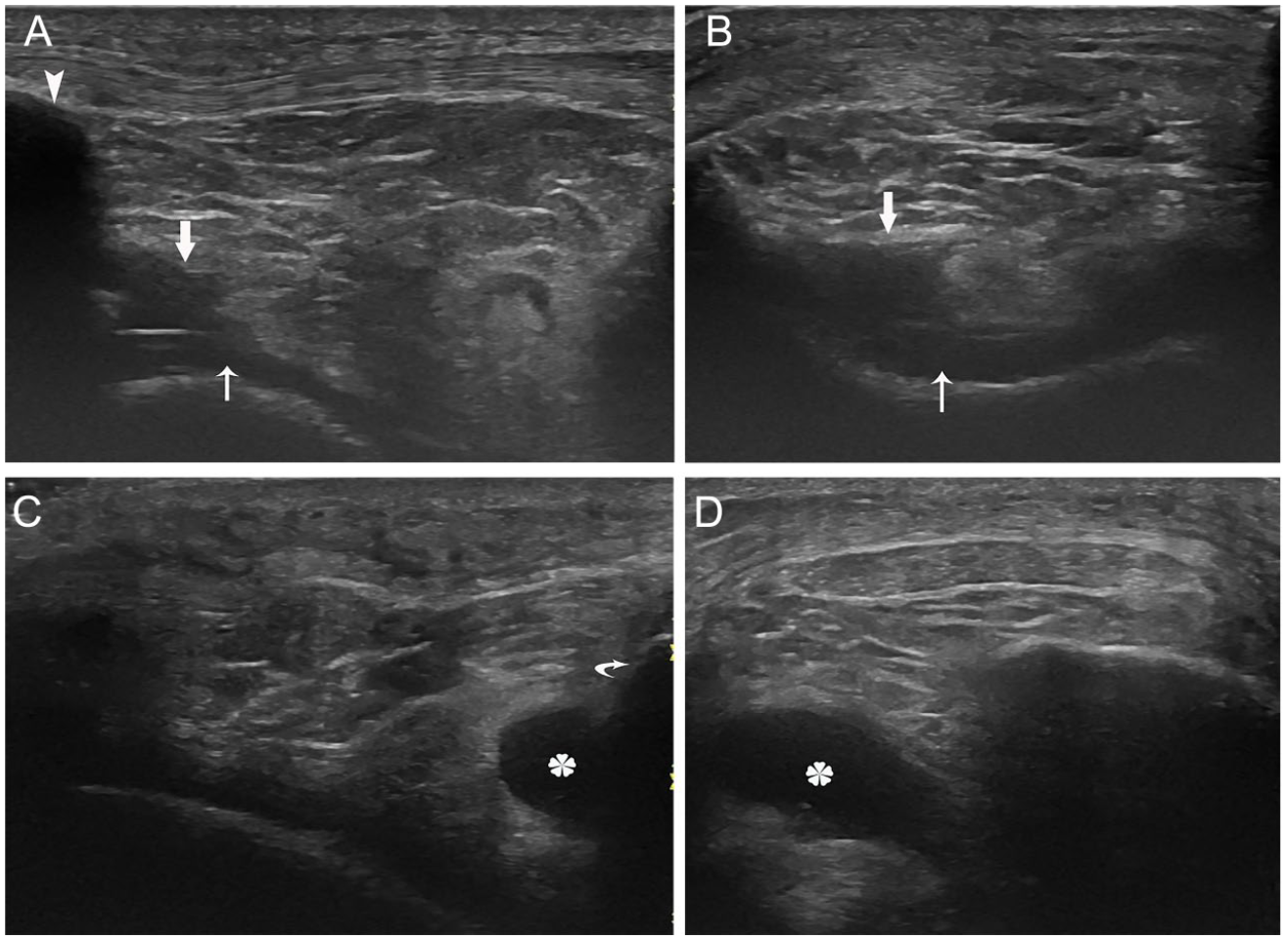
Infrapatellar recesses: (A) on sagittal view, the suprahoffatic recess (thick arrow) is inferior to the patella (arrowhead) and superficial to the joint (thin arrow); (B) on transverse view, this recess is superficial to the joint; (C) on sagittal view, the infrahoffatic recess (asterisk) is superior to the tibia (curved arrow); (B) on transverse view, this recess is pipe-like.
Parameniscal Recesses
These are the recesses on either side of knee located superior and inferior to the meniscus.2,8,9 They are in contact with the femoral condyle superiorly and tibial condyle inferiorly on either side (see Figure 4A–C). The recess on the lateral side (lateral recess) is usually more obvious than the one on the medial side (medial recess) of the knee. 8 With significant knee effusion, the superior pouch (the portion of the recess superior to the meniscus) can be seen connected with the parapatellar recesses anteriorly (see Figure 2A,C,D). The peripheral surface of the menisci themselves is not covered by the synovial membrane.
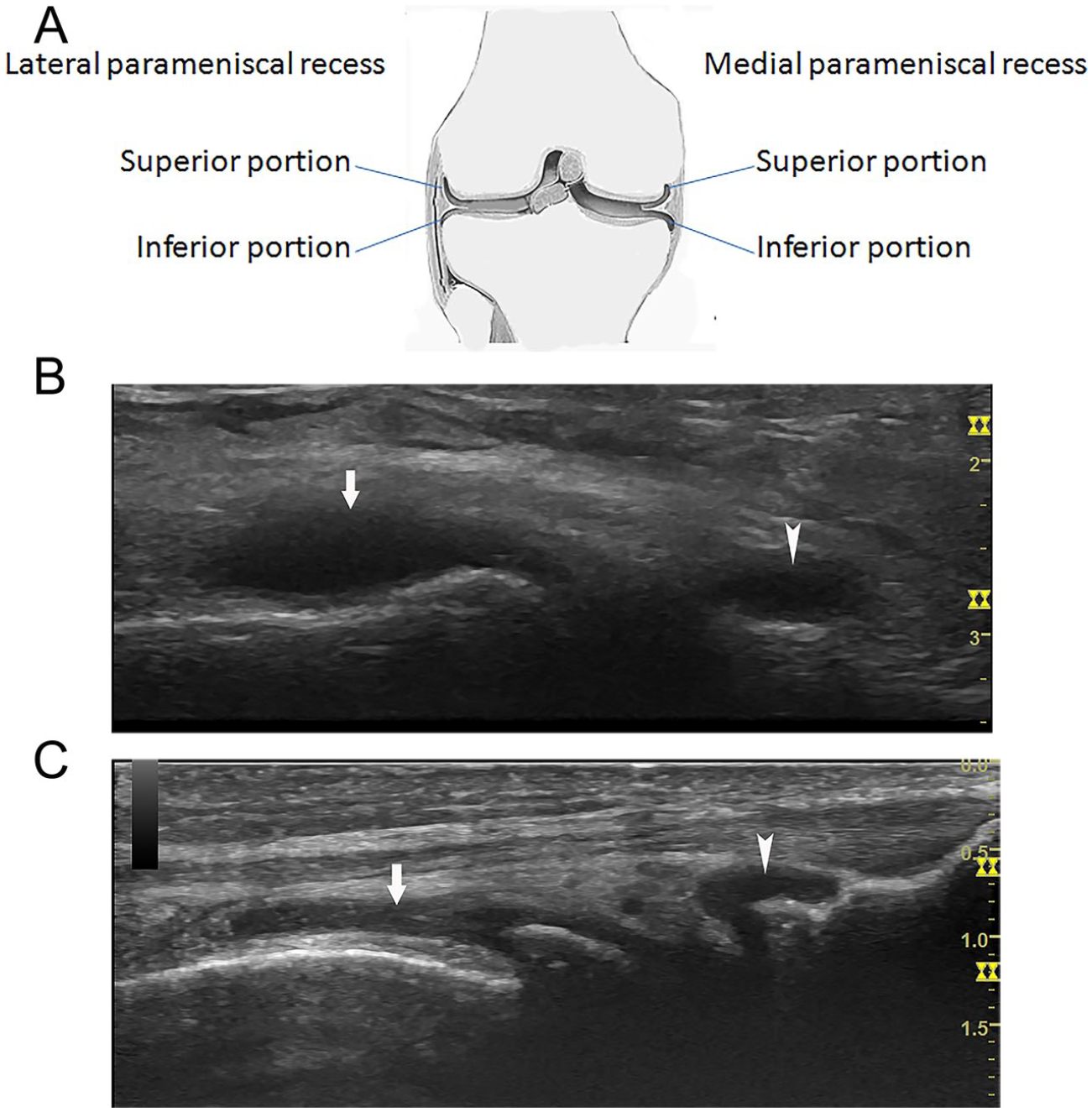
Parameniscal recesses: on coronal view, (A) the diagram of the parameniscal recesses; the superior pouch (arrow) and the inferior pouch (arrowhead) of (B) medial and (C) lateral parameniscal recesses.
Posterior Recesses
These are the synovial recesses in the popliteal fossa, including the posterior femoral recesses (posterior capsular recesses, or subgastrocnemius recesses), the subpopliteal recess, the posterior cruciate ligament (PCL) recess, and a small recess posterior to the lateral meniscus but superior to the tibia (referred to as the posterior supratibial recess).7,8,10
The posterior femoral recesses consist of medial and lateral recesses (see Figure 2A and Figure 5A,B). The posterior medial recess is located between the medial posterior condyles of the femur and the deep surface of the medial head of the gastrocnemius, while the posterior lateral recess is located between the lateral posterior condyle of the femur and the lateral head of the gastocnemius.7,8
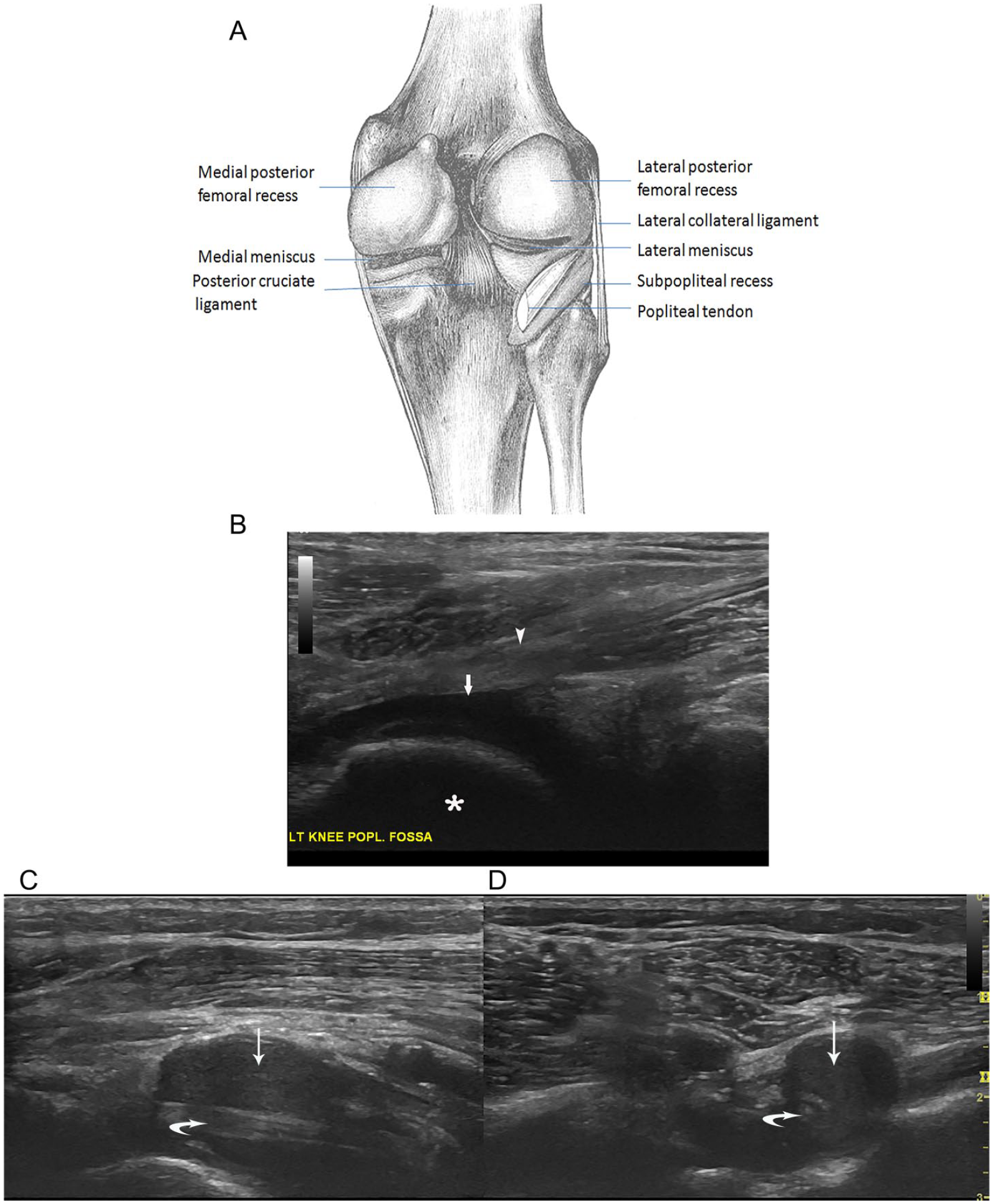
Posterior femoral recesses and subpopliteal recess: (A) posterior view of the recesses (modified from Gray’s anatomy of the human body, 1918); (B) the posterior femoral recess (arrow) is superficial to the posterior condyles of the femur (asterisk) but deep to the gastrocnemius(arrowhead) on sagittal view; (C) on longitudinal view, the popliteal tendon (curved arrow) is seen inside and along the subpopliteal recess (thin arrow); (D) on axis view, the popliteal tendon is seen mostly surrounded by this recess.
The subpopliteal recess is a small cul-de-sac between the posterior horn of the lateral meniscus and the popliteus tendon (see Figure 5A,C,D). It may be connected to the proximal tibiofibular joint in 10% of adults. 7
The PCL recess is the posterior extension of the medial femorotibial compartment. It is located posteriorly (superficially) to the PCL and adjacent to the lateral aspect of the medial femoral condyle in the popliteal fossa. 2 The anterior portion of the recess is in contact with the PCL except for the proximal one-third of it (Figure 6A). 10 The PCL recess can be round or elliptical and is commonly found when knee effusion is present. The recess can be distended during knee flexion. The connection between the recess and the medial femorotibial compartment is via a constricted area, or neck (see Figure 6B). 10
The posterior cruciate ligament (PCL) recess: (A) on sagittal view, the recess (thick arrow) is superficial to the PCL (arrowhead); (B) on transverse view, the recess is connected to the cartilage margin of the tibia (thin arrow).
The posterior supratibial recess is a small recess near the posterior midline and superior to the tibial. 11 It is also adjacent (lateral and superficial) to the distal end of the PCL. In many situations, the distended recess can be seen with the PCL in the same sagittal view (see Figure 7A). On transverse view, it is connected with the cartilage margin of the tibia (see Figure 7B). 11
Posterior supratibial recess: (A) on sagittal view, the recess (thick arrow) is superficial to the distal end of the posterior cruciate ligament (arrowhead); (B) on transverse view, the recess connects with the joint (thin arrow).
Effusion Etiology, Detection, and Diagnosis
Effusion Etiology
Knee effusion can occur in many situations. Osteoarthritis may be the most common cause. It usually presents in older, overweight, or obese individuals because of degenerative change or due to excessive weight on the knee joint, resulting in wear and tear of the articular cartilage.2,12 Another common cause is knee injury.2,13 Cruciate ligaments (anterior and posterior) tears, meniscal tears, articular cartilage injury, and patellar dislocation all can cause bleeding within the joint. Three quarters of acute hemarthrosis occurs due to an ACL tear. It usually happens in active individuals with an obvious trauma history. Quadriceps atrophy caused by patellofemoral dysfunction or the effect of injury, immobilization, or surgical procedures can also result in joint effusion.2,12 Gout and pseudogout are also sources for joint effusion. 13 The former is caused by the deposition of sodium urate crystals in the articular cartilage, while the latter is caused by calcium pyrophosphate deposition. The crystalline deposits irritate the tissue and result in effusion. Other causes of the joint effusion include benign synovial tumors, rheumatoid arthritis, psoriatic arthritis, or infection.2,12
Effusion Detection
The exact physiological amount of fluid in the knee joint is not known. If fluid in the joint is less than 6 to 8 mL, it cannot be appreciated clinically. 6 The distribution of the fluid in the joint is mainly influenced by the volume of the fluid, the position of the knee, and whether there is a Baker cyst in existence. In full extension of the knee, the parapatellar recesses are the most dependent recesses in the anterior knee, with the lateral parapatellar recess more dependent than the medial recess.4–6 Therefore, a small volume of fluid in the joint usually collects in the lateral parapatellar recess. With a larger volume, fluid also starts to collect in the medial parapatellar recess followed by the suprapatellar recess. For evaluation of fluid in the knee joint, ultrasound has demonstrated high correlation with MRI.14,15 The most sensitive sonographic approach is the transverse scan of the lateral parapatellar recess with knee extension, which can identify as little as 4 mL of fluid in live patients. 16 The joint cupping maneuver can be used to allow for detection of fluid at 1 mL in cadavers, which is equivalent to the sensitivity of an MRI. This maneuver can be done by applying pressure, with one hand, simultaneously on the medial side of the patella, the lateral lower side of the patella, and the infrapatellar area. It squeezes fluid from the rest of the recesses into the lateral parapatellar recess. 17 In living patients, the sensitivity showed no significant difference between the midline longitudinal scan of the suprapatellar recess and the longitudinal scan of the lateral parapatellar recess with knee extension. 16 Voluntary quadriceps contraction can increase the sensitivity of detecting knee effusion in the suprapatellar recess with knee extension. 18
More than 60% of Baker cysts in adult patients communicate with the knee joint through a capsular opening in the posterior medial femoral recess. 19 Because of the functional valve mechanism, fluid in the knee joint is constantly drained into Baker cysts, which results in decreased fluid in the anterior knee.20,21 Therefore, in adult patients with Baker cysts, lack of fluid in the suprapatellar recess cannot rule out knee effusion.
Effusion Diagnosis
When the knee flexes from extension, the fluid in the anterior knee will be redistributed.4,5 More fluid will shift to the suprapatellar recess and medial parapatellar recess. Therefore, it is easier to detect an effusion longitudinally in the suprapatellar recess and the medial parapatellar recess when the knee is in flexion. 5 An international study on knee effusion showed that the longitudinal scan of the suprapatellar recess with 30 degrees flexion of the knee is the best position for detection of knee effusion compared to scans of the lateral parapatellar and medial parapatellar recesses with the knees at different (0°, 15°, 30°, 45°, 60°, and 90°) degrees of flexion. 22 They also noted that the fluid diameter in the lateral parapatellar recess displayed less variation during various degrees of flexion. Therefore, their suggested protocol is to start the examination of the knee by a longitudinal scan of the lateral parapatellar recess with the knee in extension. If an effusion is detected, no further search for an effusion is needed. Otherwise, it is advised to evaluate the suprapatellar recess with the knee in flexion at 30 degrees. 22
There is no consensus for the volume required to be diagnosed with a knee effusion. Some suggest 4 mm of fluid depth with the transducer in a longitudinal position in the midline of the suprapatellar recess with the knee in full extension. 1 Others propose an accumulation of 2 mm in depth in the lateral parapatellar recess on coronal scan with the knee in extension. 16 The cutoff value suggested by the above international study is between 3.6 and 6.0 mm on the longitudinal scan of the suprapatellar recess with the knee in 30 degrees flexion (use 3.6 mm for higher sensitivity than specificity; use 6 mm for higher specificity than sensitivity). 22
Diagnostic Differentiation
Effusions within synovial recesses in some locations can be easily misdiagnosed. They need to be differentiated from cysts, bursitis, and other lesions in these areas.
Ganglion Cysts in the Infrapatellar Space
A ganglion cyst is an extra-articular cyst that can be found anywhere around the knee. It can arise from tendons, ligaments, joint capsule, bursa, muscles, and even nerves. It contains mucinous content and is lined by connective tissue. Ganglion cysts usually do not communicate with surrounding joint capsules. 23 It is postulated that ganglion cysts originate from mesenchymal cells at the synovial capsular junction. Because of repetitive micro-injury to the supporting capsular structure, fibroblasts are stimulated to produce hyaluronic acid, which is the mucinous content of the cysts. 24 Most ganglion cysts are asymptomatic. Some may present with pain, tenderness, or impinged nerve symptoms depending on the location of the cysts.
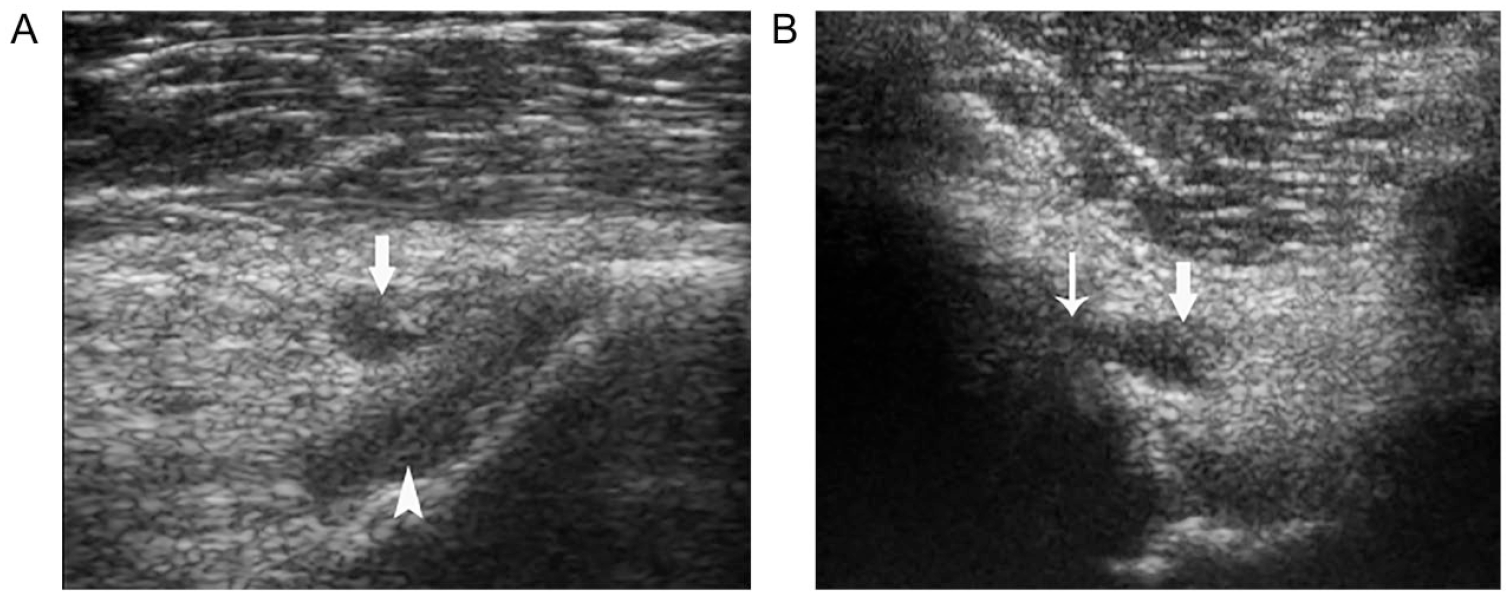
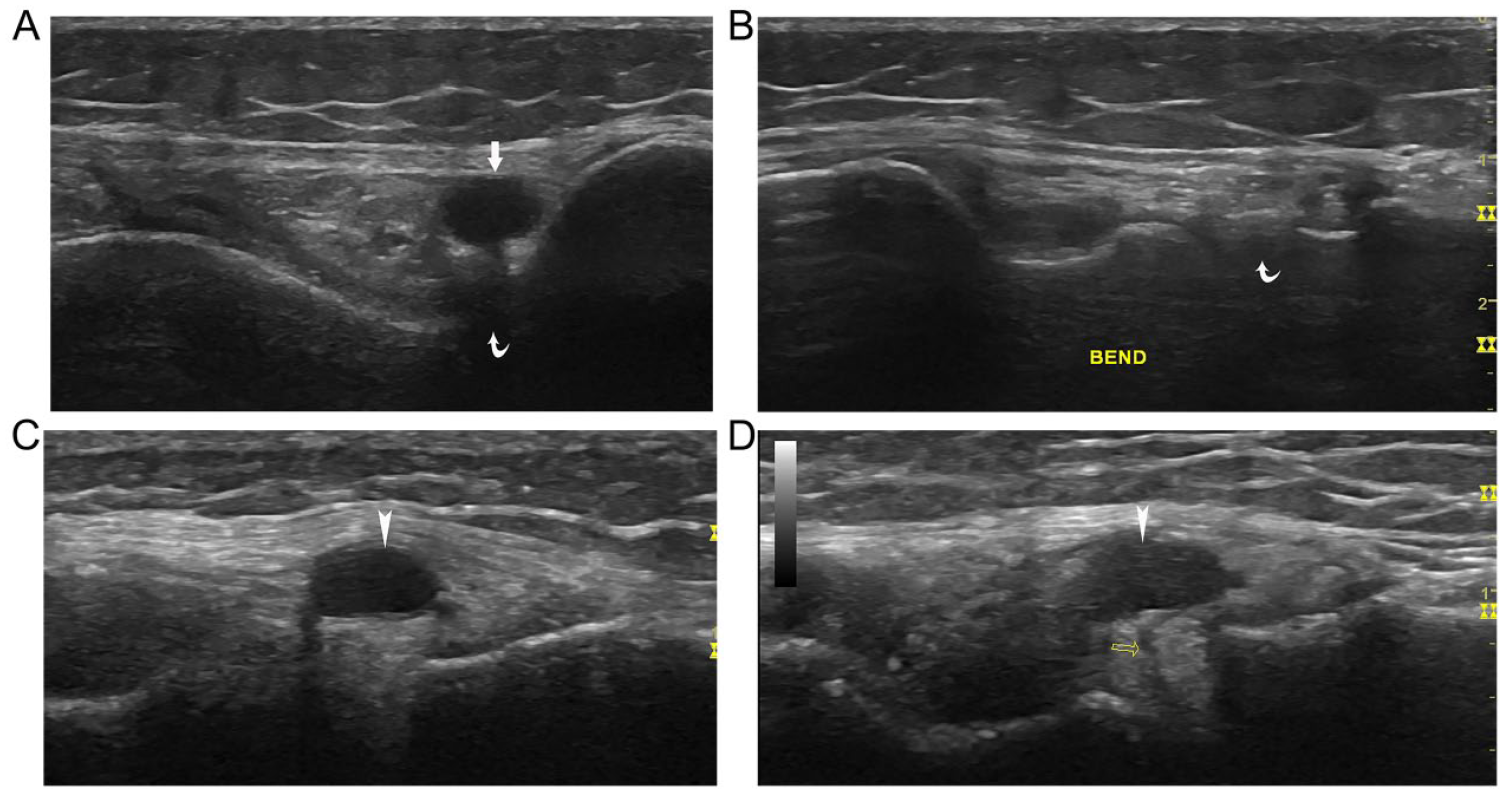
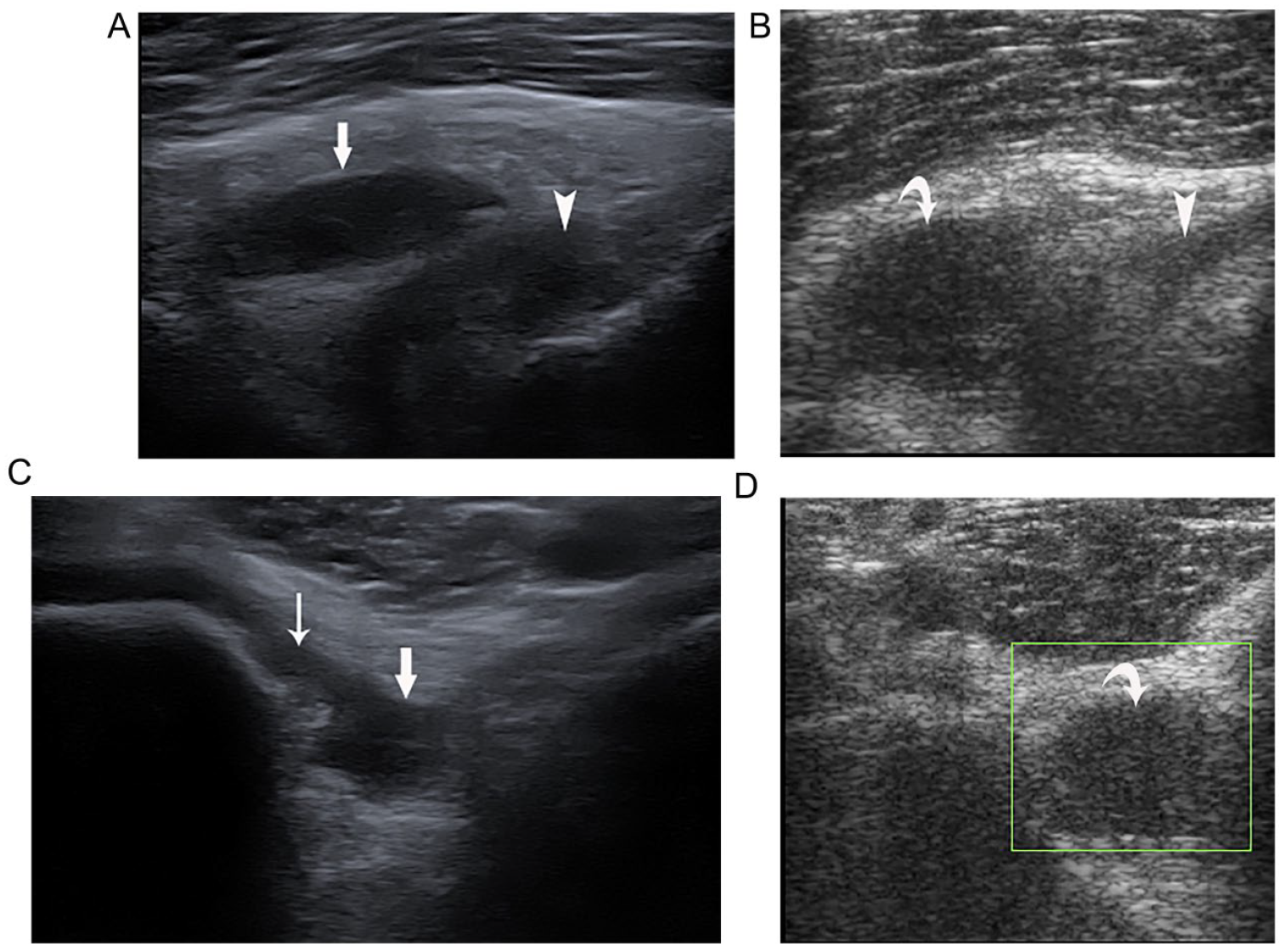
As we mentioned earlier, the infrapatellar space is an intracapsular but extrasynovial structure. Infrapatellar cysts in the knee are uncommon and occur mostly as ganglion cysts in men between ages 20 and 40 years. 25 The majority arise from the ACL while the rest arise from the PCL and menisci.26,27 The ACL is attached anteriorly to the front of the intercondyloid eminence of the tibia. It goes upward, backward, and laterally to attach to the medial and posterior aspect of the lateral condyle of the femur (see Figure 1A). ACL cysts are usually lobulated with a distinctive boundary. They extend along the course of the ACL and may also extend anteriorly toward Hoffa’s fat pad or posteriorly toward the femoral intercondylar fossa. 8 If an intracapsular cyst extends toward Hoffa’s fat pad (see Figure 8A,B), it needs to be differentiated from an effusion of the infrahoffatic recess, which is also anterior to the ACL (see Figure 8C). On a transverse view, an infrahoffatic recess often appears horizontally oriented. It can also be tracked to demonstrate its contact with the inferior tibial articular margin with dynamic scanning (see Figure 8D). Its shape and size may change with flexion and extension of the knee, while a ganglion cyst does not.4,5,10
Infrapatellar cyst and cyst-like infrahoffatic recess: the infrapatellar cyst (arrow) on sagittal (A) and transverse (B) views. The cyst-like infrahoffatic recess (arrowhead) on sagittal view (C) appears as a cyst, but on transverse view (D), it shows a connection with the tibial articular margin (thin arrow).
Lateral Meniscal Cyst
Meniscal cysts are one of the common disorders of the knee. They are cystic lesions filled with mucoid fluid. They may be parameniscal, intrameniscal or both, but during sonography, only the parameniscal cysts can be detected. 28 The pathogenesis of meniscal cysts is still not clear. One common explanation is that the meniscal cyst is developed from the collection of the synovial fluid through a tear in the articular surface of the meniscus.6,26 Another is that the cyst may be formed by cystic degeneration of the meniscus without tear. 28 It has been generally thought that the lateral meniscal cysts are more common than the medial meniscal cysts. However, recent MRI and arthroscopic studies indicate that there are more medial meniscal cysts than lateral ones.26,28 Most meniscal cysts are asymptomatic but with palpable and firm masses. Some may present with vague pain and tenderness.6,28 The lateral meniscal cysts usually grow anterior or posterior to the lateral collateral ligament (LCL) adjacent to the meniscus, while the medial meniscal cysts may extend through a pedicle from the meniscus because of the restriction of the medial collateral ligament (MCL). 6
Sometimes the inferior pouch of the lateral parameniscal recess can be seen turning around the inferior edge of the lateral meniscus and extending superiorly along the external surface of the meniscus. This phenomenon is usually seen when the knee is in the extended position. If the connection between the superiorly extended inferior pouch and the joint is too thin to be seen, it may look like a lateral meniscal cyst (see Figure 9A). 29 To differentiate it from a meniscal cyst, the simplest method is to flex the knee to more than 30 degrees. If the cyst-like structure disappears or becomes smaller, or a connection to the knee joint can be seen, then it is a parameniscal recess (see Figure 9B). Furthermore, a meniscal cyst can usually be traced to the source at the meniscus, typically where a tear of the meniscus is found (Figure 9C,D). 20
Meniscal cyst-like parameniscal recess and meniscal cyst: on coronal view, (A) the inferior pouch (arrow) of the lateral parameniscal recess appears as a meniscal cyst in the superficial aspect of the lateral meniscus (curved arrow) with the knee in extension position; (B) the cyst-like structure disappears with the knee flexing more than 30 degrees; (C) a lateral meniscal cyst (arrowhead); (D) this cyst has a connection with the meniscal tear (empty arrow).
Iliotibial Band Friction Syndrome
Iliotibial band friction syndrome (ITBFS) is very common among athletes, especially runners. Therefore, it is also known as “runner’s knee.” 30 Patients typically present with lateral knee pain after repetitive motion of the knee. Physical examination can locate tenderness at the lateral femoral epicondyle.23,31 The iliotibial band (ITB), also known as the iliotibial tract, is a thickened longitudinal fibrous band. It arises from the tendons of the tensor fasciae latae and gluteus maximus muscles at the upper lateral aspect of the thigh and inserts at the Gerdy tubercle at the anterolateral aspect of the tibia. At its distal third, ITB contacts the lateral aspect of the lateral femoral epicondyle while traveling along the lateral side of the knee. The extension and flexion of the knee is accompanied by the ITB moving forward and backward. During running or cycling, irritative stresses on the ITB and the underlying tissues caused by anteroposterior movement or mediolateral movement of the ITB over the lateral femoral epicondyle result in this syndrome. 30
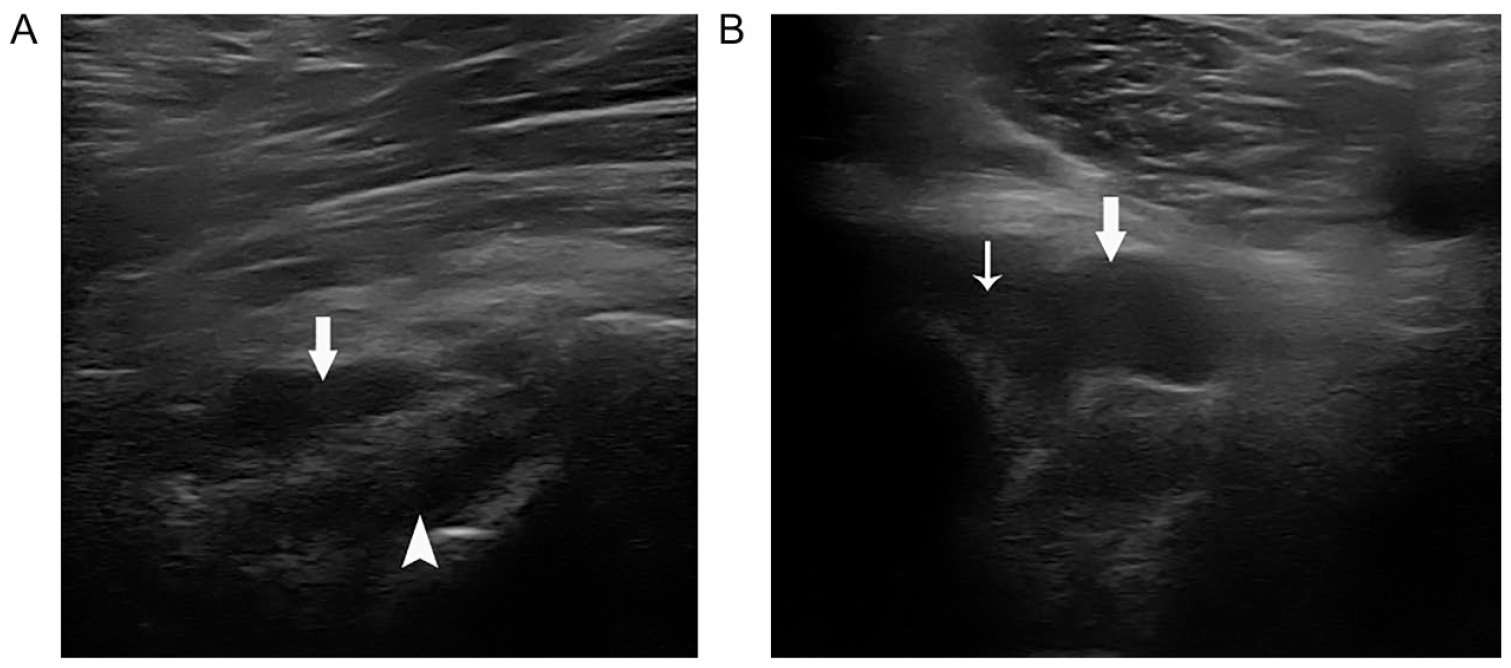
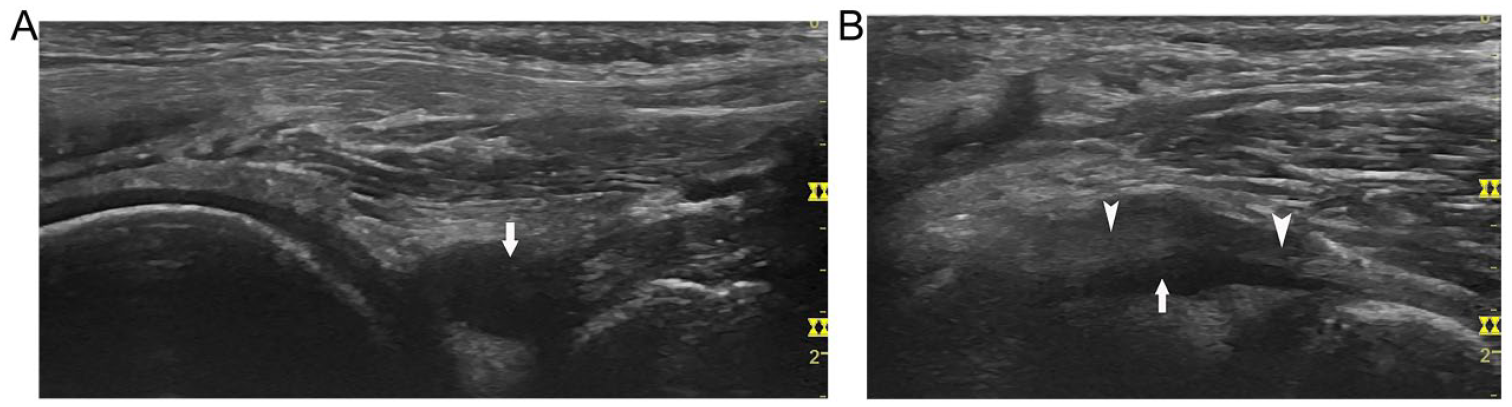
The pathology of ITBFS still remains controversial. The earlier hypothesis of ITBFS is that the repetitive friction of ITB over the lateral femoral condyle causes thickening of the ITB, as well as a bursitis in the sub-ITB space. However, the latest reports based on MRI, arthroscopy, and biopsy of cadavers did not identify inflammation of the ITB or a bursa deep to the ITB. Instead, they found MRI signal changes in the soft tissues deep to the ITB and in the lateral extension of the parapatellar recess deep and posterior to ITB. They called this recess a lateral synovial recess (LSR).32,33 It acts like a bursa between the ITB and the lateral femoral condyle to reduce the friction. The synovium deep to the ITB in ITBFS demonstrated chronic inflammatory change. 31 Therefore, an LSR effusion with focal synovial wall changes may be one of the important pathologic appearances of ITBFS. Another important pathologic appearance may be the inflammatory changes in the soft tissue deep to the ITB, as some researchers found that only this sign was observed in ITBFS (see Figure 10A,B).31,33
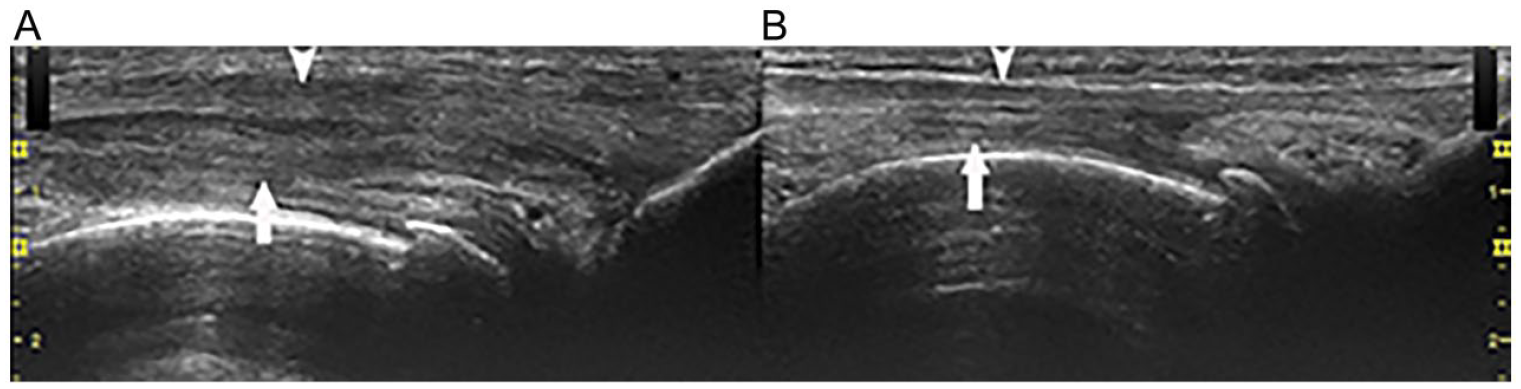
Deep soft tissue changes in iliotibial band friction syndrome: on coronal view, (A) the soft tissue (arrow) deep to the iliotibial band (arrowhead) shows hypoechoic and thicker changes compared with (B) the contralateral normal knee.
Knee effusion with extension to the LSR deep to the ITB is a regular phenomenon (see Figure 2D). 30 If patients do not have ITBFS symptoms, the effusion in the LSR may only imply that the amount of fluid in the knee joint is significant. If patients have ITBFS symptoms, it is crucial to determine if the source of the fluid is from the knee joint or an isolated accumulation. 29 The most important aspect of the examination is whether the synovial wall of the LSR is thick and demonstrates increased vasculature with power Doppler. If there is an LSR effusion but without a focal synovial wall and soft tissue pathologic changes, the diagnosis of ITBFS cannot be established even if the patients have symptoms.
Cysts Deep to the LCL and Inferior to the Lateral Meniscus
The effusion of the parameniscal recess on the lateral aspect of the knee usually displays fluid in both of the superior and inferior pouches (Figure 4C). However, sometimes only the inferior pouch is effused and appears isolated from the meniscus, which mimics a cyst deep to the LCL (Figure 11A). Therefore, it is necessary to differentiate it from a ganglion cyst in the same position. Ganglion cysts are usually multilobular while an effusion is a smooth unilocular fluid collection. In most situations, if the transducer position is appropriately adjusted, the cyst-like effusion can be tracked cranially to the joint space between the meniscus and the tibial plateau. Sometimes the connection between the cyst-like lesion and the joint space may be too thin to be seen, but with medial rotation of the knee or further flexion of the knee, an effusion will become smaller or disappear (see Figure 11B).4,5
Cyst-like parameniscal recess deep to the lateral collateral ligament (LCL): on coronal view, (A) the inferior pouch of the lateral parameniscal recess appears as a cyst (arrow) deep to the LCL (arrowhead); (B) the cyst-like structure changes to cord shape with the knee flexing more than 30 degrees.
Medial Collateral Ligament Bursitis
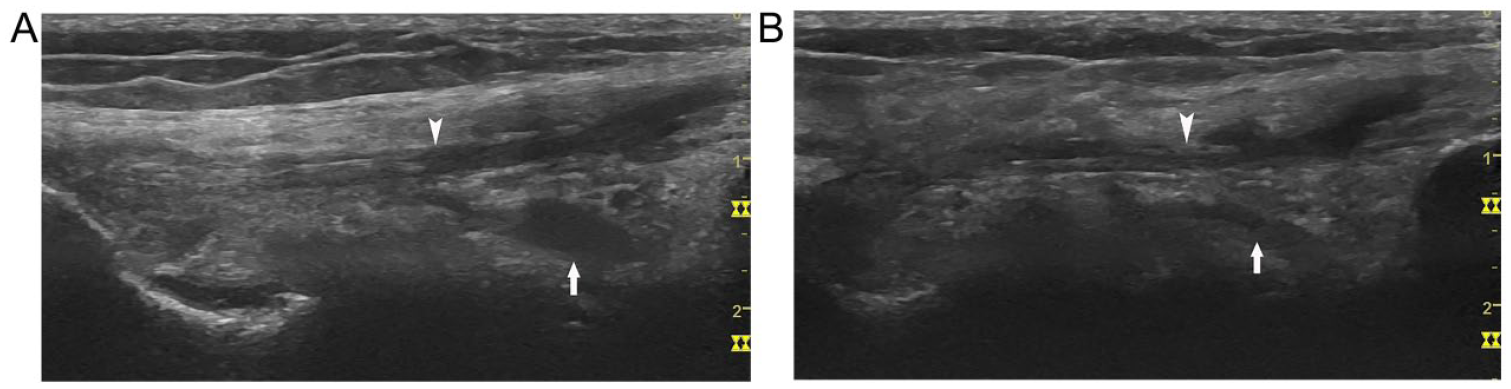
The medial collateral ligament (MCL) is composed of a superficial layer and a deep layer. The superficial layer is a strong, flat, and straight vertical fibrous band in the middle third of the knee. The deep layer is a thickening of the medial joint capsule, which is interlaced with the medial meniscus and attaches superiorly and inferiorly to the articular margins of the joint to form the meniscofemoral and meniscotibial ligaments.6,29,34 MCL bursa is located between the two layers of MCL. When the knee is in flexion, the bursa allows the MCL to glide over the bony surfaces of the tibia and femur without friction. The bursa is often separated into femoral and tibial compartments. The femoral compartment is superiorly located adjacent to the femoral cortex, whereas the tibial compartment is inferiorly located adjacent to the tibial cortex (see Figure 12A). 34 Normally, MCL bursa cannot be visualized with ultrasound or MRI. The distension of fluid in MCL bursa is usually a sign of bursitis caused by inflammation of the bursa. 34
Medial collateral ligament (MCL) bursitis and medial parameniscal recess: on coronal view, (A) fluid collection appears between the superficial layer (arrowhead) and the deep layer (arrow) of the MCL inferior to the medial meniscus (tibial compartment); (B) inferior pouch of the medial parameniscal recess (curved arrow) appears as bursitis of the tibial compartment of the MCL bursa with the knee in extension position; (C) with the knee in a 30-degree flexion position, the recess becomes smaller and the connection to the knee joint also appears (thin arrow).
The effusion of the inferior pouch of the medial parameniscal recess is sonographically very similar to the distension of the tibial compartment of MCL bursa (see Figure 12B). In most cases, this effusion can be identified deep to the deep layer of the MCL and can be tracked to the joint by moving the probe anteriorly. Therefore, the differentiation is usually not a problem. However, in some situations, it is difficult to track the effusion. As mentioned earlier, the shape and size of the parameniscal recess change with changes to knee position. When flexing the knee from extension to 30 degrees or more, the recess usually becomes smaller or even disappears. In addition, one can track the effusion to the joint because of the redistribution of fluid in the knee (see Figure 12C). In contrast, the fluid shape and size in MCL bursa may have no change or become more obvious with the knee flexed.
PCL Cyst
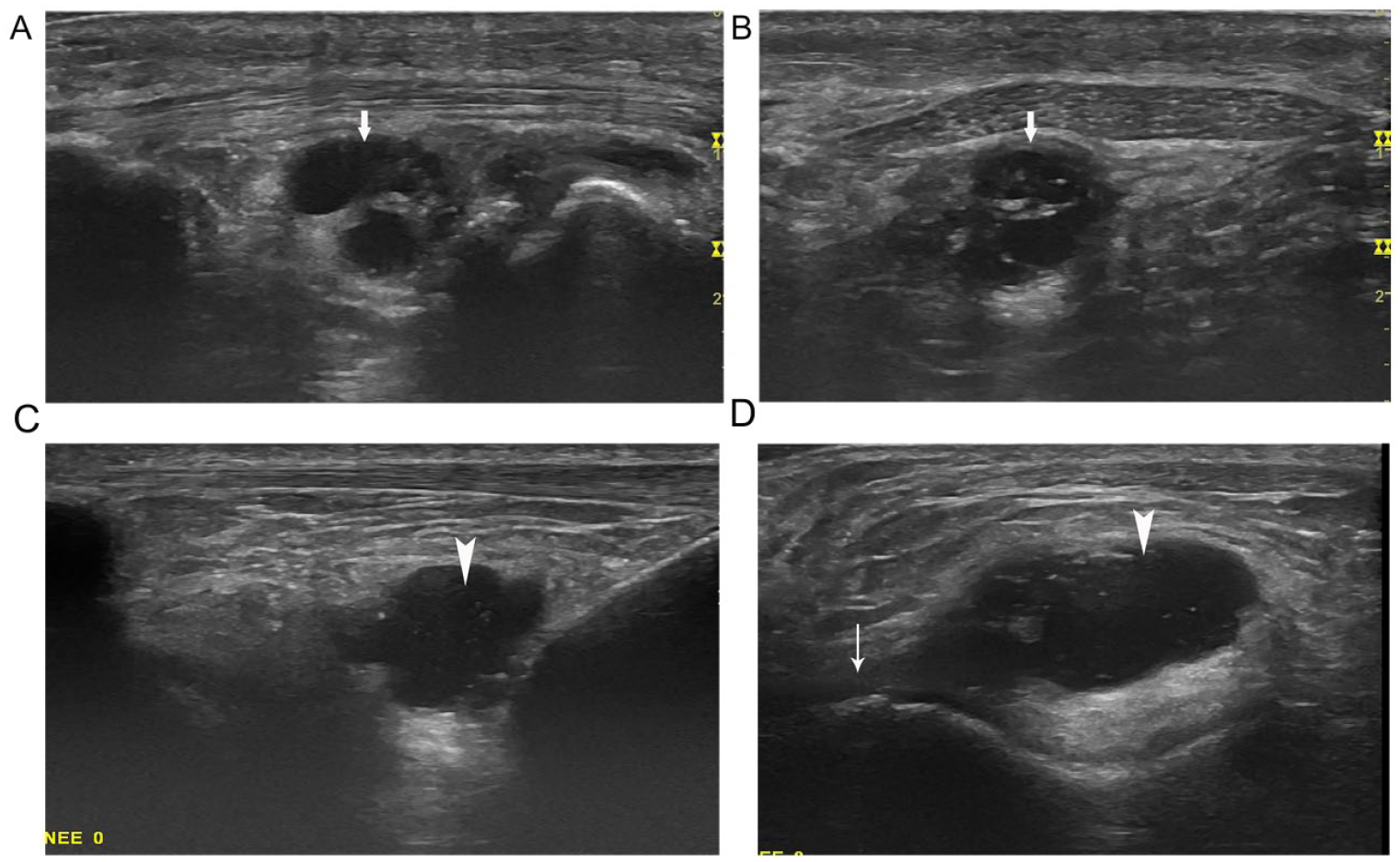
Effusion in the posterior supratibial recess and PCL recess is frequently seen when a knee effusion is present. 10 Since both of these recesses are adjacent to the PCL, the effusion of either of these recesses may be seen as a cyst-like lesion posterior to the PCL (see Figure 13A).
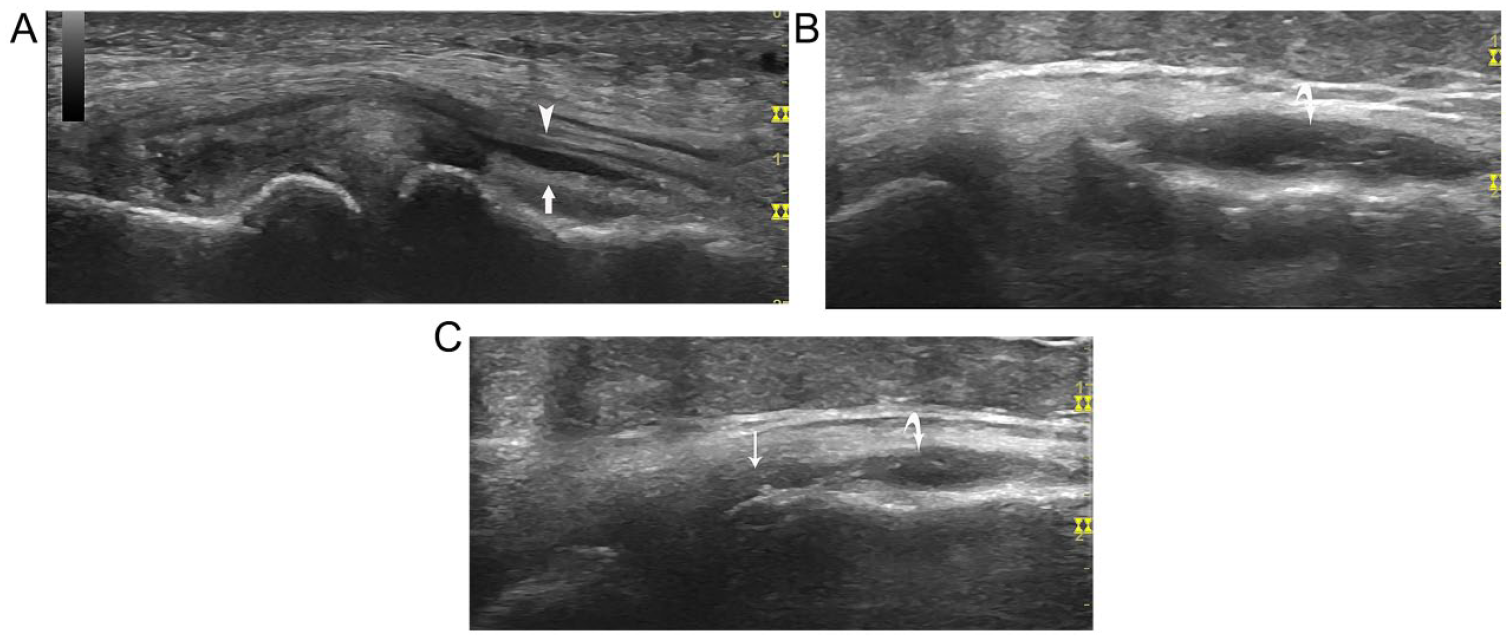
Cyst-like posterior cruciate ligament (PCL) recess and PCL cyst: on sagittal view, (A) PCL recess (arrow) and (B) PCL cyst (curved arrow). They both are posterior (or superficial) to the PCL (arrowhead). However, on transverse view, (C) the PCL recess (arrow) has a connection with the medial femorotibial compartment (thin arrow) while (D) the PCL cyst (curved arrow) has no such connection.
The PCL originates from the posterior intercondylar region and ends at the back of the tibial plateau (see Figures 1A and 5A). As mentioned earlier, it is an intra-articular structure similar to the ACL. PCL cysts are less common than ACL cysts. It is speculated that mechanical stress on the posterior aspect of the PCL during knee movement may be the cause of PCL cysts. 35 The majority of PCL cysts are located posterior to the PCL. 25 They range from very small to large (see Figure 13B). 8 The supratibial and PCL recesses are usually round or oval shaped, and they have no contact with the proximal one-third of the PCL. 8 Adjusting the orientation of the transducer may reveal the connection of the PCL recess with the medial femorotibial compartment or the connection of the posterior supratibial recess with the tibia (see Figure 13C). However, a PCL cyst has neither such connections (see Figure 13D). Clinical factors also need to be considered as PCL cysts usually occur in those younger than 40 years, while patients with effusions of the popliteal recesses are usually older than 45 years.6,25
Meniscal Cyst of the Posterior Lateral Horn
The effusion of the subpopliteal recess is the fluid partially surrounding the popliteal tendon in its anterior, superior, and inferior aspects. The subpopliteal recess is posterior to the posterior horn of the lateral meniscus. 7 Its effusion on sagittal view of the lateral popliteal fossa appears as an anechoic lesion adjacent to the posterior horn of the lateral meniscus, which looks similar to a meniscal cyst (see Figure 14A). The sagittal view of the popliteal fossa is actually an oblique view of the tendon. Therefore, to differentiate a subpopliteal recess effusion from a meniscal cyst, rotating the probe clockwise (right knee) or counterclockwise (left knee) to have it parallel to the popliteal tendon will allow a longitudinal view of the tendon and of the recess. In this probe position, the tendon will be seen inside and along the recess (Figure 14B). Further rotating the probe 90 degrees to get a transverse view of the tendon, the fluid of effusion surrounding the three aspects of the tendon could be seen (see Figure 5D). A meniscal cyst does not have these characteristics (see Figure 9C,D).
Meniscal cyst-like subpopliteal recess: (A) on sagittal view of the lateral popliteal fossa, the subpopliteal recess (arrow) mimics the meniscal cyst of the posterior lateral horn; (B) on longitudinal view of the popliteal tendon, the cyst-like recess surrounds the tendon (arrowhead).
Conclusion
Knee effusion is usually the earliest sign of synovial disease of the knee. Many pathological conditions or diseases of the knee can cause effusion. A consensus criterion for the diagnosis of knee effusion is needed to allow for accurate and consistent diagnoses. In the meantime, familiarity with the appearances and locations of the synovial recesses is necessary for differentiating unique presentations of knee effusion from other cystic lesions around the knee.