
Abstract
Portal hypertension is a result of an increase in intrahepatic resistance in the main portal vein. The Meso-Rex shunt is used to bypass the obstructed portal vein and restore the venous flow into the liver. This procedure alleviates the need for a hepatic transplant. The Meso-Rex shunt has proven to be an effective treatment for extrahepatic portal vein obstruction, thus saving children from a complete transplant. There are variants to this bypass surgery, and sonography is commonly used to assess the condition pre- and postoperatively. In this case, the shunt was uniquely different from the typical Meso-Rex bypass surgery. Particular vasculature made it imperative for the sonographer to review the prior sonograms and review the chart information before preforming the examination. It should also be noted that sonographers must adapt the protocols to give the utmost treatment.
The Meso-Rex shunt is used to alleviate portal hypertension due to an extrahepatic portal vein obstruction. The shunt connects the superior mesenteric vein to the left portal vein, bypassing the main portal vein. Modified versions of this procedure are being conducted that can make the sonographic anatomy difficult to interpret due to the abnormal abdominal vasculature at the porta hepatitis or area of anastomosis. In most cases, the procedure places the Meso-Rex shunt in the left lobe of the liver, between segments III and IV, and is connected to the left portal vein. There are instances when the shunt may be placed in differing locations due to patient body habitus. However, for the patient in this case study, the shunt had a normal placement in the left lobe of the liver. The Meso-Rex shunt can be an effective treatment for children with obstructions and saves pediatric patients from a complete or partial liver transplantation. Saving the patient the inconvenience of liver transplant surgery may alleviate the threat of rejection and failure.1,2
Case Report
A two-year-old female was referred to a pediatric hospital, from an outside facility, and presented with an extrahepatic portal vein thrombosis. Prenatally, the patient presented with secundum atrial septum defect (ASD), cleft lip, and cholestasis. She had jaundice shortly after birth, and a potential biliary atresia diagnosis was considered. During this time, it was documented in her chart that it was difficult to demonstrate a gallbladder, leading to an uncertainty as to its presence. However, the neonatal jaundice was treated and resolved, and the biliary atresia was not pursued. At six months old, she was referred for further workup due to the incidental findings of hypersplenism and gastroesophageal varices. Over the following months, a full workup was completed by a health care team. The patient was also referred to a larger pediatric hospital for further investigation of the diagnosis of extrahepatic portal vein obstruction. Performed as part of the hospital’s diagnostic protocol, a transhepatic venogram demonstrated a functional liver and a patent left intrahepatic portal vein. These results made the patient a viable candidate for a Meso-Rex bypass (also known as a mesocaval shunt). The preoperative images, which included a sonogram and a computed tomography (CT) of the abdomen and pelvis, documented a malrotation of the intestines: the small bowel on the right side and most of the colon on the left. The malrotation of the intestines caused the superior mesenteric vein and artery to be inverted right to left as well. Again, it was noted that it was difficult to demonstrate the presence of a gallbladder. In addition, extremely pronounced portal biliopathy was visualized due to the obstructed extrahepatic portal thrombosis, causing the gastroesophageal varices to arise and compress the common bile duct. It was emphasized, at this point, that her inferior mesenteric vein was prominent and thought to be suitable for the bypass due to its length. Due to the patient’s malrotated bowel, the superior mesenteric vein was no longer to the right of the superior mesenteric vein but on the left side. This meant that the closest venous structure for attachment was the splenic vein. However, this was still farther away from the left portal vein than normal and thus why surgeons needed a longer vessel than the normal procedure. Normally, they would graft from the internal jugular vein. In this case, however, they would need a longer vessel to follow the course the shunt needed to make. A preoperative sonogram exhibited cavernous transformation at the porta hepatis with decreased portal venous flow.
Following the diagnostic workup and consultation with the specialized surgical team, the patient underwent surgery at 20 months of age to obtain the Meso-Rex shunt. During surgery, the surgical team grafted a piece from the inferior mesenteric vein for the bypass. It was noted at this point that (1) there was a large vein emanating from the splenic vein near the duodenojejunal flexure, and (2) the bowel was completely malrotated with the small bowel on the right and colon on the left. The inferior mesenteric vein graft was then surgically resected to an appropriate length and turned 180 degrees with a general curve along the inferior border (tail) of the pancreas to the opposite lesser sac and through the gastrohepatic ligament up the Rex recessus (left portal vein system near the ligamentum teres) (Figure 1). The lead surgeon checked the position and performed an end-to-end venous anastomosis, which used the Inferior Mesenteric Vein (IMV) graft to form a connection from the splenic vein to the left portal vein, creating the Meso-Rex shunt.
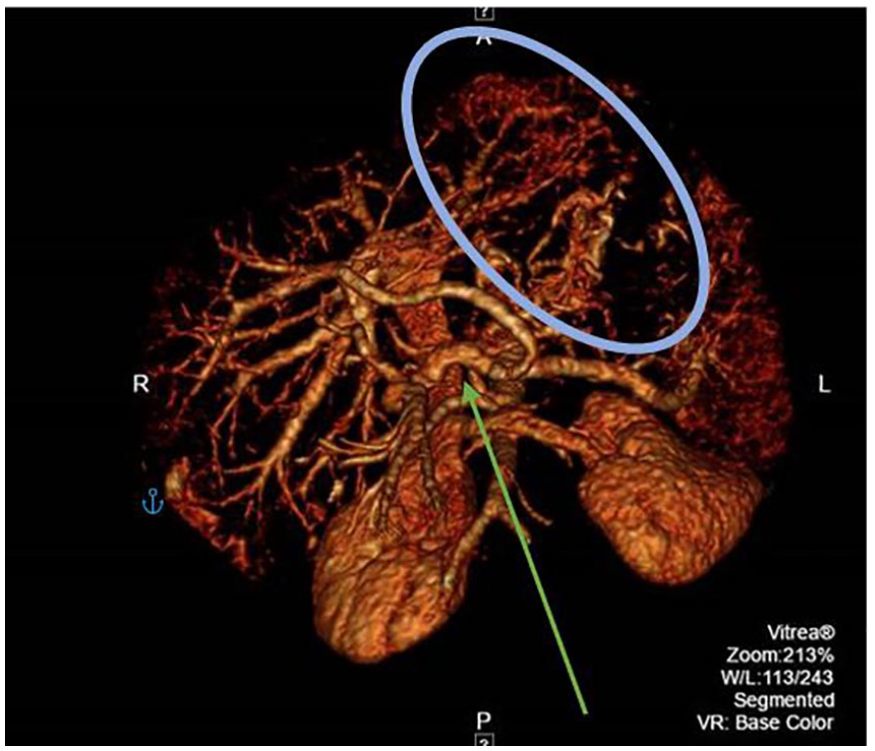
A three-dimensional computed tomographic scan demonstrating the tortuous Rex shunt placed (green arrow) and the noted varices (blue circle).
A sonogram was performed one day postoperatively to evaluate for patency of the shunt. The protocol at the pediatric hospital includes grayscale sonographic and duplex images of the left portal vein, the main portal vein, and mid-shunt, as well as at the anastomosis at the end of the left portal vein and at the Superior Mesenteric Vein (SMV) end. These images are in addition to the images in a complete abdomen protocol. In this particular case, the sonographer would obtain Doppler samples near the splenic vein end of the graft due to the atypical connection. The left portal vein just distal to the anastomosis was also evaluated (Figures 2–4). The sonographic findings of this examination concluded that the Rex shunt was patent with high-velocity flow at the left portal vein anastomosis, which was thought to be secondary to postoperative edema due to the timing of the sonogram. On the fifth postoperative day, the patient underwent a CT of the abdomen, and at 15 days, she had another sonogram. The findings of these examinations concluded that the graft was stable, leading to the patient being discharged. The patient then had a follow-up appointment for a sonogram at an outside hospital one month later to reevaluate the patency of the shunt (Figure 5). The most current examination was just 4 months postoperatively and was done to evaluate patency, splenic size, and liver appearance. A radiologist who was familiar with this particular case notified the sonographer of the uncommon nature of the procedure. The shunt was anastomosed to the splenic vein rather than at the superior mesenteric vein, which was supported by the sonographic images obtained (Figures 5 and 6). The images taken demonstrated a patent Rex shunt extending from the splenic vein to the left portal vein, along the border of the pancreas. The shunt appeared unchanged but notedly more turbulent than previous examinations at the site of the anastomosis, with normal tapering. Due to this tapering at the anastomosis, the velocities tended to be more elevated, which were normal as long as the anastomosis was still patent (Figure 7). The radiologist noted that the spleen was still enlarged, measuring 11.48 cm in length, and suggested a follow-up in three months to reevaluate the hypersplenism.
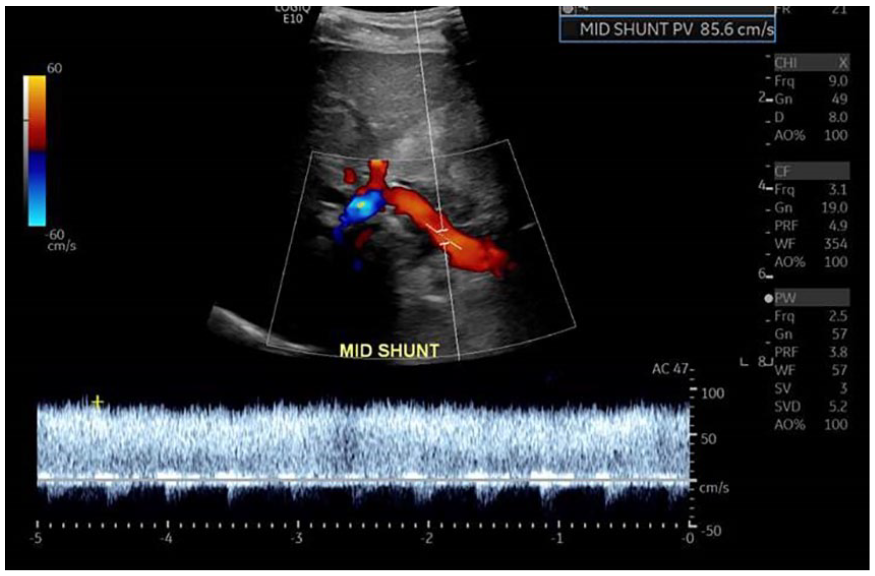
A duplex sonographic image at mid-shunt, near the liver, documenting hepatopetal flow at 85.6 cm/s.
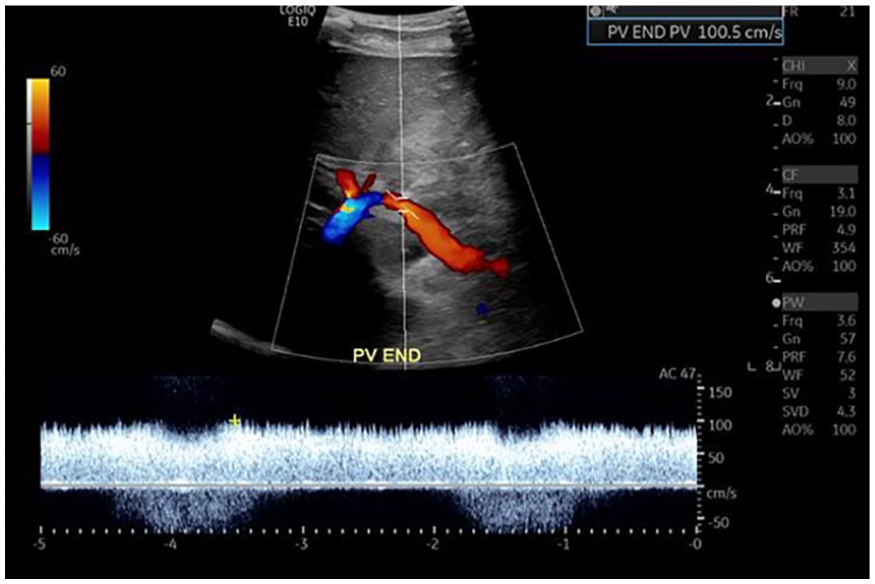
A duplex sonogram of the anastomosis with the left portal vein documenting hepatopetal flow at 100.5 cm/s.
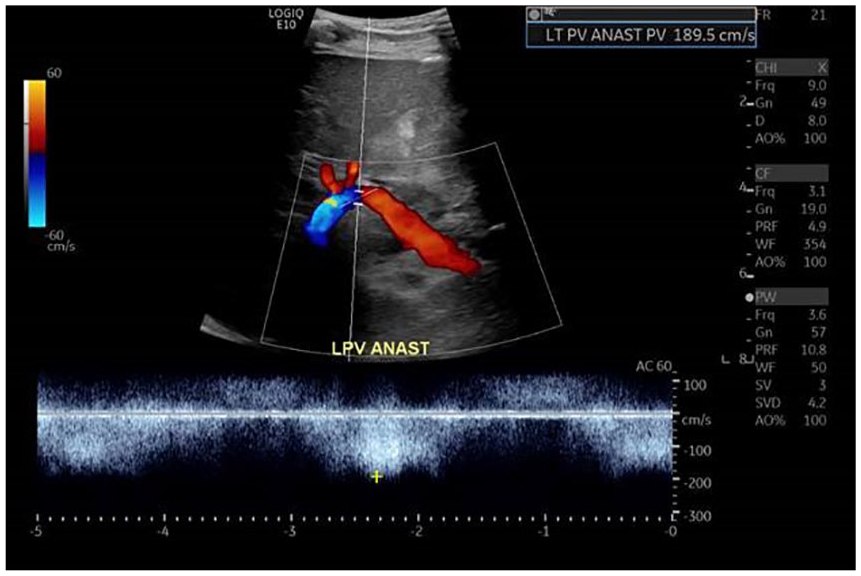
A duplex evaluation of the left portal vein just distal to the anastomosis, displaying the expected increased flow velocity distal to the connection point.
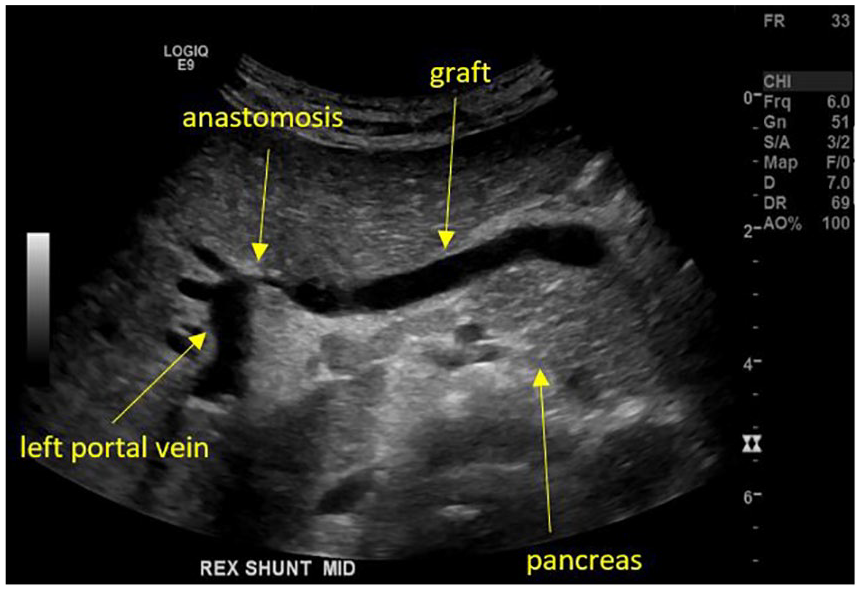
A grayscale sonogram of the shunt lying along the body of the pancreas and connecting to the left portal vein.
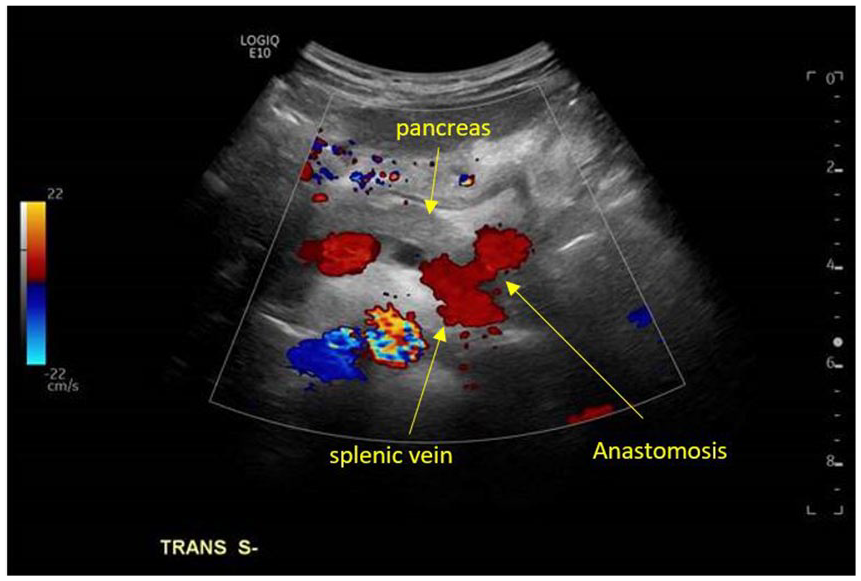
A color Doppler sonogram documenting the anastomosis of the shunt to the splenic vein at the level of the pancreatic tail.
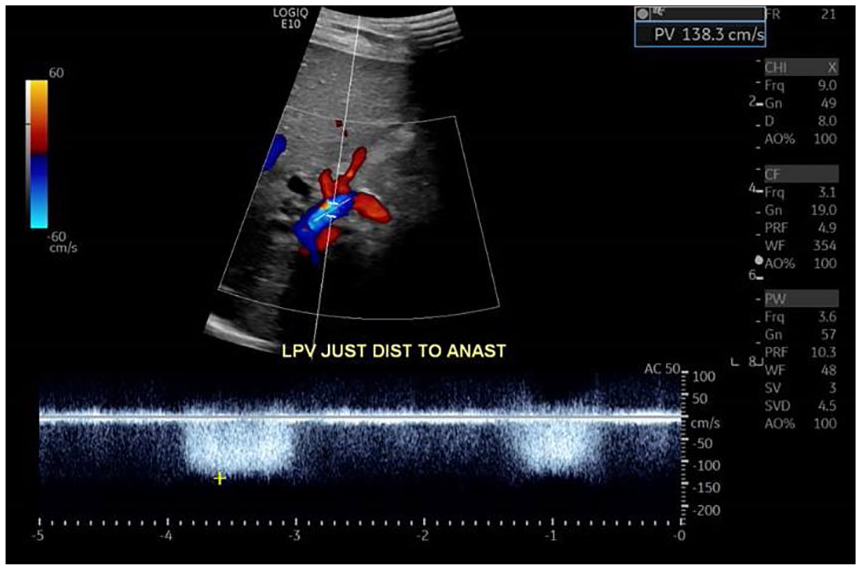
A duplex sonographic evaluation of the left portal vein just distal to the shunt anastomosis obtained at the follow-up examination approximately six weeks after surgery. Flow was turbulent but the velocity was not quite as elevated as on the previous examination. The velocity at this examination was 138.3 cm/s.
Discussion
The Meso-Rex bypass is a procedure involving the use of a native venous graft to create a shunt to bypass an obstructed extrahepatic portal vein. This procedure alleviates the patients’ need for a liver transplant as long as they meet the following criteria: absence of intrinsic liver disease, patent left portal vein in Rex recess measuring at least 2 mm in diameter, contiguity of the right and left portal veins, and adequate mesenteric veins to serve an inflow of blood from the mesentery. 3 The Rex shunt is meant to be a curative to the broad diagnosis of portal hypertension. 3 Portal hypertension in pediatric medicine is usually a result of an increase in intrahepatic resistance to hepatopetal portal venous flow. 1 Extrahepatic portal vein obstruction (EHPVO) is one of three different types of portal hypertension and is considered the most common cause of upper gastrointestinal bleeding in children.4,5 Clinical signs of this obstruction include splenomegaly, ascites, prominent abdominal veins hematemesis due to esophageal varices, hepatic encephalopathy, and hypersplenism.1,5 Splenomegaly in a one- to two-year-old female is anything over 6.3 cm, which is the mean size of the spleen in this age group. 2 The patient in this case presented with a number of these clinical signs, which were the cause for referral to a different pediatric hospital. However, in 50% of children and young adult cases, the etiology of the thrombosis is unknown. 2 These obstructions can happen in the venous flow at three levels: prehepatic (caused by portal or splenic vein thrombosis), intrahepatic (secondary to cirrhosis), or posthepatic (secondary to hepatic vein occlusion, congestive heart failure, or constrictive pericarditis). 3 It is possible for the thrombosis of the extrahepatic portal vein to extend into the intrahepatic portal vein as well. This thrombosis impairs the hepatopetal flow from the SMV and splenic vein, causing a development of prehepatic portal hypertension. 5 In this case, the patient had an extrahepatic main portal vein thrombosis. Doppler findings of this thrombosis include a decreased portal venous inflow, diminished portal vein pulsatility, and bidirectional or reverse portal venous flow. 1
The Meso-Rex shunt is a gold-standard treatment option because it restores venous flow in an otherwise normal liver.4,6 Originally, it was used to treat thrombosis on post–liver transplants in adult patients. 4 However, now it is used to save the patient from undergoing a transplant surgery, and there are no concerns for rejection due to the use of the patient’s vessels.5,6 Sonography is used to confirm the cavernous appearance of the liver preoperatively and is postoperatively used to evaluate shunt patency.6,7 The procedure begins by grafting the left internal jugular vein.5,6 The internal jugular vein is used to build this “bridge” around the blockage at the main portal vein.6,8 Alternate veins that can also be used include a coronary artery, recanalized umbilical vein remnant, the great saphenous vein, or, in the case of this patient, the inferior mesenteric vein.6,8 With regard to this patient, surgeons needed a vein that was longer due to the route the shunt would have to take to connect to the splenic vein. First, the surgical team reroutes the splanchnic (viscera organs) venous blood through the graft. 2 The surgeons then make a dissection for the Rex recessus, where the shunt will sit within the liver.5,6 They will then check the left portal vein for patency as this is the vessel that the graft will be anastomosed to distally. 6 The portal vein blood is then redirected into the left intrahepatic portal venous circulation. 8 After checking the liver site, surgeons will normally check the SMV site of anastomosis for the connection there.6,7 However, in this case, they connected the shunt to the splenic vein at the area of the tail of the pancreas. This connection has been reported to be used when the patient has a small or damaged SMV. 7 This patient’s SMV and the Superior Mesenteric Artery (SMA) were malrotated due to malrotation of the bowel, making the connection to the splenic vein more efficient.
The Rex shunt provides the patient with durable relief from portal hypertension symptoms.9,10 This shunt is better than other shunts comparatively because it has the potential to restore normal portal flow and liver function. Children with this EHPVO have no intrinsic liver disease, but they can have delayed growth, mild coagulopathy, or neurocognitive dysfunction. 10 It was found that this patient had a patent splenic vein, SMV, and IMV, which allowed for a good surgical outcome. Connecting the shunt will hemodynamically cause reversal of flow in the left portal vein, bringing blood into the liver. The placement of the shunt into the Rex recessus is a good location because it is rarely involved with cavernous transformation. It resolves the portal hypertension and increases flow to the liver, and over time, the intrahepatic portal venous branches expand as the cavernous appearance decreases. Due to the decreased resistance to hepatopetal flow, splenomegaly also decreases over time while the hepatic volume tends to expand 1.3 to 2.7 times the baseline. 9
Conclusion
With this groundbreaking procedure being performed on children from all over the United States, it is imperative that sonographers are aware of it. Much like this case, these patients travel to and from different hospitals to obtain follow-up sonograms. Knowing what anatomy can differ and what to expect are crucial. Sonographic imaging of the abdominal vasculature is already a technically difficult study. These children can also display abnormal anatomy, making it important to understand the “normal” measurements, flow velocities, and procedural variations that can be encountered. It is important to review prior measurements so as to better understand the current values obtained during examination. This case is an excellent example of the importance of reviewing the prior diagnostic information and knowing what to expect when examining patients, particularly pediatric patients, with this shunt. Had the sonographer not reviewed the prior case, the velocities could have been taken inaccurately, causing discrepancy in the diagnostic values. At a minimum, time would have been lost due to the confusion of encountering such a difficult abdominal vascular pathway. The case is not only important for pediatric sonographers, who will likely face this type of vascular circulation, but could be equally important in examining adults. This patient will hopefully live a long life after having this procedure but will likely need an abdominal Doppler examination as an adult. Longitudinally, it is imperative that sonographers adapt to patients’ extraordinary anatomy to provide patients like this with a quality examination.
Footnotes
Acknowledgements
Special Thank You to Kaitlyn William, RT(R), RDMS, RVT.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.