
Abstract
Objective:
Sonographic evaluation for acute appendicitis in children often involves an exhaustive protocol, for which the therapeutic yield has not been formally evaluated. The purpose of the study was to pilot a retrospective chart review of children receiving an abdominopelvic sonogram upon presenting with suspected acute appendicitis.
Methods:
An annual retrospective chart review was designed to review abdominopelvic sonograms to rule out appendicitis and specifically performed at a Canadian children’s teaching hospital. Studies were excluded if the requisition stated multiple clinical concerns or if the patient was >18 years at the time of the sonogram.
Results:
Based on 230 patient cases reviewed, alternative diagnostic sonographic findings were found in 141 (61%) charts. Only 18 patient cases (8%) demonstrated both alternative sonographic findings as well as a change in management by the emergency room physician.
Conclusion:
Alternative diagnostic findings, based on a complete abdominopelvic sonogram, were common (61%) in this chart review but rarely changed patient management.
Acute appendicitis (AA) is the most common acute abdominal disorder that requires surgery, 1 and ultrasonography (US) is widely considered the most appropriate front-line imaging modality for pediatric AA patients. This is due to its comparable sensitivity and specificity with computed tomography (CT) 2 and its nonionizing, noninvasive nature. Although the accuracy of US for AA is well researched, no studies have evaluated the diagnostic or therapeutic yield of different sonography protocols.
Since initial use of US for the diagnosis of AA, 3 its application for acute appendicitis, in children, has evolved and expanded and includes the interrogation of all solid abdominal organs, as well as the retroperitoneum, bowel, and pelvis. This may be due to the belief that a comprehensive US is justified in the pediatric population, given that children may not be able to properly localize and describe their pain, limiting clinical assessment.
However, the frequency of relevant findings unrelated to the appendix in this setting remains unknown, so it is unclear whether more imaging equates to a better diagnosis for these patients. It is also important to consider whether exhaustive imaging protocols (paired with increasing rates of appendicitis cases 4 ) exacerbate the ongoing issue of long wait times in Canadian emergency rooms (ERs). 5 This also can result in added follow-up imaging appointments and increasing diagnostic imaging time. Overuse of diagnostic imaging is recognized as an ongoing issue, 6 and it may also contribute to observed high rates of burnout (compassion fatigue) 7 among sonographers.
The purpose of this study was to determine the feasibility of a retrospective chart review and measure the true value of an abdominopelvic US, in a pediatric setting, for suspected acute appendicitis. The primary outcome measure is the proportion of non-appendix-related findings (alternative findings) corresponding with a deviation in standard ER care. The objective was to determine whether an abdominopelvic US protocol contributed to the therapeutic yield of imaging for appendicitis versus a targeted approach. This type of pioneering quality improvement research is essential to promoting and maintaining value-based care, applying the as low as reasonably achievable (ALARA) principle, optimizing delivery of services for patient-centered care, and promoting/implementing evidence-based practice.
Methods
The design of this study was a retrospective chart review and a review of the patient’s medical records.
Sampling
To identify all the abdominopelvic US performed at the study institution over a one-year period, the clinical indication chosen was an intention to rule out acute appendicitis. The sample population that was identified was completed in two stages:
Stage 1: The radiology information system (RIS) was queried by a picture archiving and communication system (PACS) data specialist. This was done to identify all abdominopelvic US performed between January 1, 2018, and January 1, 2019, and requested through the ER.
Stage 2: A manual review was completed by a single reviewer, to screen the ER requisitions, for queried cases and exclude those based on eligibility criteria (see Table 1). Any ambiguous cases were flagged and a final decision was rendered by a clinical imaging expert with over 10 years of pediatric imaging experience.
Exclusion and Inclusion Criteria for Cases in Sampling Stage 2.
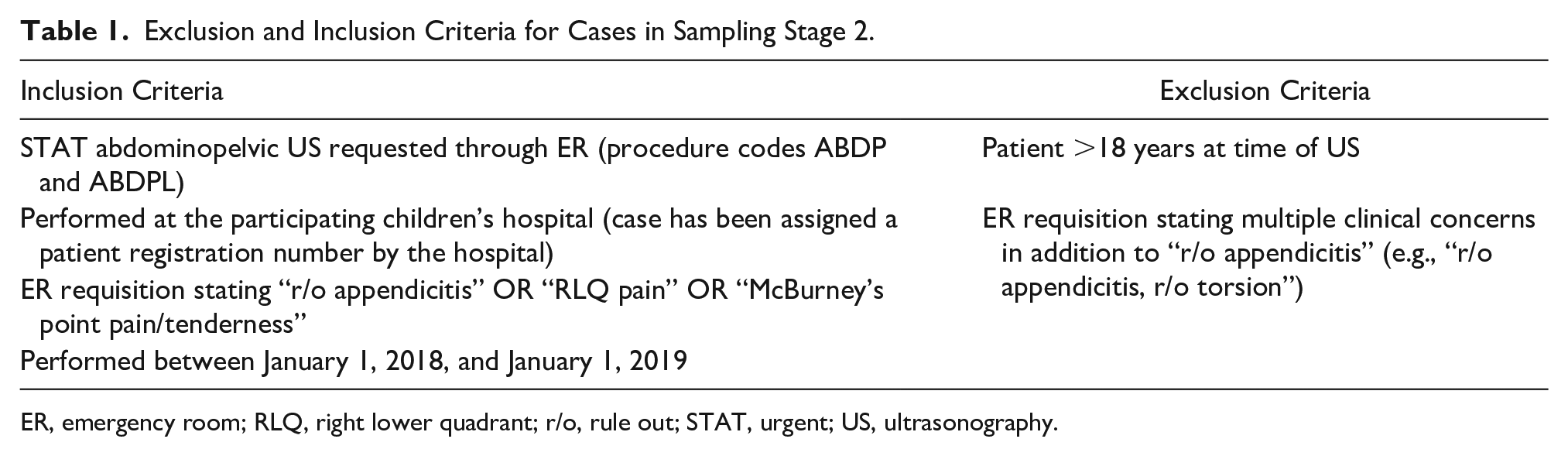
ER, emergency room; RLQ, right lower quadrant; r/o, rule out; STAT, urgent; US, ultrasonography.
Data Extraction
Data were extracted from the patient’s record according to the Data Collection Form (Appendix A, available online). “Presence of right lower quadrant (RLQ) focal tenderness” was determined if, in the sonographer’s impression sheet, it identified that the patient was tender to probe pressure. The visualization of the appendix, presence of 1- and 2-degree signs of acute appendicitis, and alternative findings were determined based on the radiologist’s final diagnostic report. The study institution’s definitions for US evidence of acute appendicitis can be found in Appendix B (available online). The length of the US was based on the time stamp for the first and last images saved to the patient file PACS.
Demographic information (sex, age, and chief complaint) and clinical data (white blood cell count, pain score) were extracted directly from the ER medical record, using an electronic database. To determine whether there was a deviation in the standard of care for suspected acute appendicitis, the Risk Stratification Tool (Appendix C, available online) was used as the guideline when investigating patient records. This tool serves as a patient management guideline for physicians in the ER at the study institution for patients suspected of having acute appendicitis.
The data extraction was independently performed by four credentialed diagnostic medical sonographers. Ambiguous records were discussed and consensus reached by the author group.
Data Analysis
The present study is based on the reported frequencies based on the observed findings, and no inferential statistical testing was planned. As a result, a sample size for statistical power was not needed. The primary outcome measure was the proportion of alternative US findings that resulted in a deviation of standard ER care. The results represent the proportion of cases for which alternative findings from the abdominopelvic US could have influenced patient management (Figure 1). This study was reviewed and approved by the Hamilton Integrated Research Ethics Board (HiREB) project 7220-C.
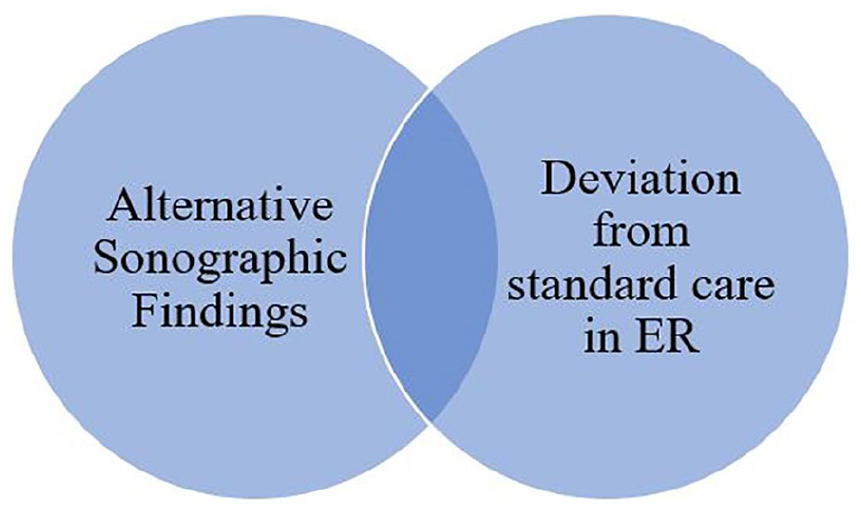
Schematic representation of findings that represent the primary outcome (shaded area). This area of overlap theoretically represents the proportion of alternative sonographic findings that are clinically relevant.
Results
The sampling strategy identified 1648 patient records in stage 1. In stage 2, 1125 patient records were excluded based on our eligibility criteria, with 523 eligible case for review (Figure 2). Of these, a random sample of 230 cases were reviewed for feasibility due to the logistical limitations. The mean patient age in this population was 9.27 years. In total, 174 US patient cases were male patients (75.6%) and 56 (24.3%) were female patients.
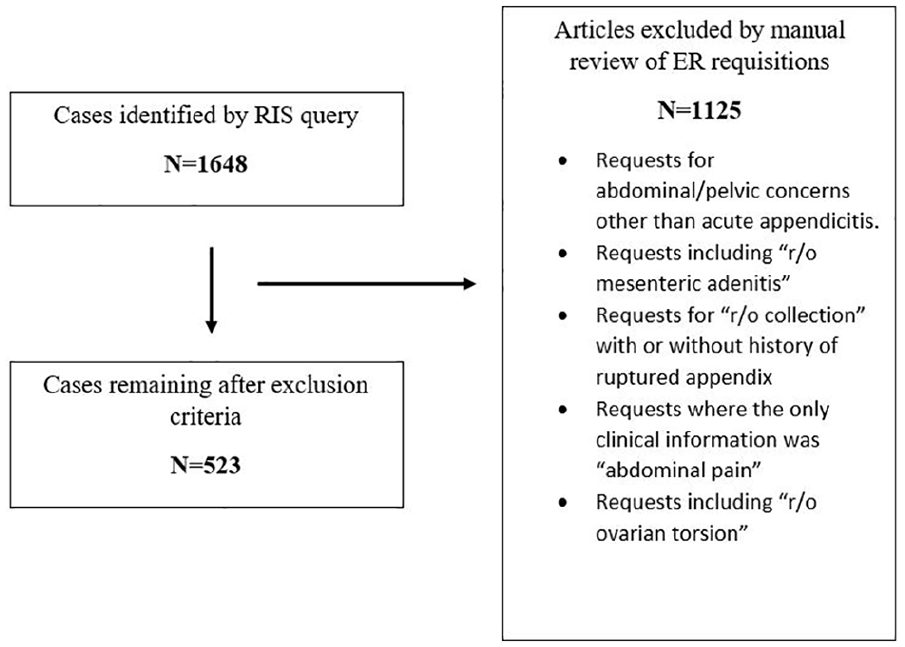
Flowchart of records selection with justification for excluded records.
Within this sample, alternative findings on US were found in 141 (61.3%) patient cases, and the ER’s patient management departed from standard acute appendicitis in 28 cases. Only 18 patient cases (7.82%) demonstrated both alternative US diagnostic findings, as well as a change in ER management. Table 2 outlines the specific outcomes of the 18 cases and demonstrates the relationship of overlap between alternative findings and changes in patient management. Alternative US findings included but were not limited to periportal hyperechogenicity (also called “periportal cuffing” and thought to be a nonspecific sign of fever 8 ), fluid-filled bowel loops, prominent RLQ lymph nodes, renal pelvic dilatation, small bowel intussusception, mild hepatosplenomegaly, and bladder debris.
Alternative Findings and Related Change in Patient Management in the 18 Cases That Demonstrated Both Alternative Findings and a Change in Emergency Room Standard of Care.
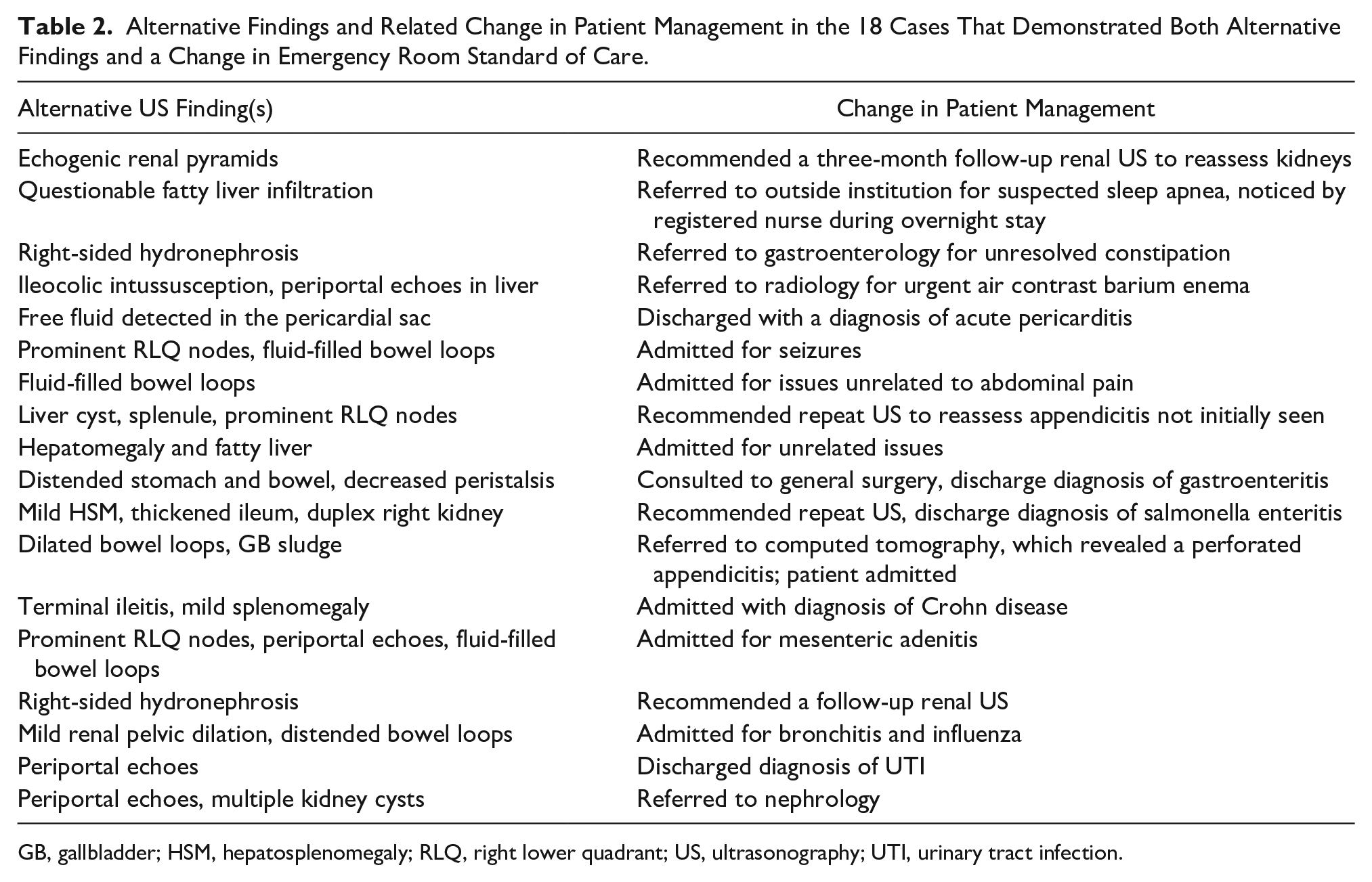
GB, gallbladder; HSM, hepatosplenomegaly; RLQ, right lower quadrant; US, ultrasonography; UTI, urinary tract infection.
The appendix was definitively identified in 142 of 230 cases (61.7%). The average time to complete the US was 27.7 minutes and the maximum US time was 95 minutes.
Discussion
This pilot study produced preliminary data on the frequency and impact of alternative US findings in pediatric patients with suspected AA. It would appear that no other study has assessed the abdominopelvic US protocol in this manner. These findings may suggest that anatomical variants of normal and findings of questionable significance are commonly detected on US (61%). In the current study, these findings were subsequently reported and may contribute to exhaustive imaging and exacerbate prolonged patient wait times and increased health care costs 5 due to follow-up US. Furthermore, this study demonstrated that few (8%) cases had both alternative findings and deviations in standard ER care. This may suggest that alternative findings on US are typically low impact and do not improve therapeutic yield. Alternative US findings were mainly reported in the liver (periportal cuffing), the bowel (fluid-filled loops, sluggish peristalsis), or classified as “other,” which was influenced by findings of prominent RLQ lymph nodes.
The appendix was definitively identified in 142 of 230 cases (61.7%). Estimates, based on the literature, on the detection of appendicitis in children vary widely. Some studies have reported detection rates of under 25% 9 and others as high as 82%. 10 This may be due to the US detection of the appendix in children, depending on body mass index (BMI), BMI-for-age percentile (but not weight), and sonographer expertise and experience.11,12 Detection rates may also depend on differences in US technique and ultrasound machine quality/parameters.
Strengths and Limitations
In this pilot study, a strength was that the data were analyzed from a relatively large sample size (230 patient records) and data extraction was performed by trained sonographers. In addition, a radiologist with over 10 years of experience in pediatric imaging guided the extraction and interpretation of the study findings.
A major limitation of this study is its inability, due to the methodology and study design, to identify whether a change in ER management of patients was attributable to alternative US findings. Although 18 cases were identified (in the sample of 230 cases) in which both alternative US findings and a change in ER management were evident, it was difficult to determine what caused those changes. The descriptive information in Table 2 is the only evidence available to suggest where this could have been the rationale for change in care.
This sample consisted of a disproportionate male to female patient ratio, which may have limited the study findings. This is likely because many female cases were eliminated in stage 2 due to requests for “r/o appendicitis and r/o ovarian torsion” and qualified under the exclusion criteria. The rationale was that inclusion of multiple clinical concerns on the requisition implied clinical uncertainty and was outside the scope of the pilot study. However, this approach does limit the applicability of the findings to the general population of children presenting with suspicion of AA. Future iterations of this work could either limit data extraction to cases of children of prepubertal age, when ovarian torsion is less common, 13 or include these in the study design.
Conclusion
In the present study, the US case and medical review determined that alternative US findings were common (61%) but had a low (8%) impact on the therapeutic yield. In this sample, only 8% of the abdominopelvic US performed to rule out AA demonstrated potentially significant alternative diagnostic findings. Whether or not this proportion justifies an exhaustive imaging evaluation versus one targeted to the appendix would need be further determined by the relevant knowledge users and stakeholders. A prospective study between groups receiving a limited versus complete abdominopelvic US could provide a higher level of evidence and inform diagnostic imaging guidelines. However, given the issues related to performing a prospective randomized trial in this acute population, a retrospective study may be the most feasible method for gathering the necessary evidence.
Future research in the area of US quality improvement could attempt to replicate these results with a different pediatric population to ensure consistency. In addition to US data, these studies should collect data on patient BMI, additional imaging postexamination, and review of the surgical reports for diagnostic confirmation. With these data, a deeper understanding may be gained on the downstream effects of an exhaustive imaging protocol. Prospective trials should be considered at sites where a limited US protocol is considered standard of care for suspected AA. This may be an option for comparing a limited US appendix protocol to an abdominopelvic protocol.
Supplemental Material
Supplemental_material – Supplemental material for Pilot Study: Outcomes of the Full Abdominopelvic Ultrasound Protocol for Diagnosis of Acute Appendicitis in Children: A Retrospective Chart Review
Supplemental material, Supplemental_material for Pilot Study: Outcomes of the Full Abdominopelvic Ultrasound Protocol for Diagnosis of Acute Appendicitis in Children: A Retrospective Chart Review by Robert Dima, Yongdong Wang, Sarah Zuccolo, Michelle Palmer and Kerry Cheong in Journal of Diagnostic Medical Sonography
Footnotes
Acknowledgements
The authors thank the following persons, without whom this project could not have been possible: Susan Kinnear, Kevin Marley, Stephanie Galez, and the incredible team of US technologists and radiologists at McMaster University Medical Centre in Hamilton, Ontario, Canada.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.