
Abstract
Objectives:
To describe sonographic findings of appendicular lymphoid hyperplasia (ALH) and to report demographic data of patients with ALH operated for acute appendicitis (AA).
Materials and Methods:
In a retrospective study, 694 biopsies of consecutive AA surgeries with previous ultrasonography (US) were reviewed, after selecting the ALH cases.
Results:
Twenty-five ALH cases were proved histologically (3.8% of appendectomies). The mean age was 13 years, with 84% under 20 years. US findings showed increased appendiceal diameter (average 7 mm) (82%), hypoechogenic pseudonodular mucosal thickening (50%), concentric parietal thickening (13%), and periappendiceal inflammatory changes (18%). In four cases, a normal appendix was noted on US, with two associated with intestinal intussusceptions.
Conclusion:
ALH is a benign entity most frequent in children that can predispose to AA. Both pathologies can increase the appendiceal diameter. In the pediatric group, ALH could be considered when hypoechogenic pseudonodular appendicular mucosal thickening in the absence of periappendiceal inflammatory changes occurs.
Appendicular lymphoid hyperplasia (ALH) was first described in the mid-20th century. 1 Initially, ALH was thought to have a role in the pathogenesis of acute appendicitis (AA), due to obstruction of the appendicular lumen.1,2 Currently, ALH is considered an independent clinical entity.
AA is a common cause of acute abdominal pain, especially in children and young adults, and the diagnosis most frequently necessitates emergent abdominal surgery.2–4
The intestinal lymphoid tissue is normally located in the intestinal wall.1,5 The lymphoid tissue is more specifically present in the mucosal layer, in the lamina propria, of the small bowel and appendix, appearing as lymphoid nodules or lymphoid infiltrate.1,5,6 When the lymphoid nodule is prominent in the intestinal wall, it is referred to as intestinal lymphoid hyperplasia.5,6 Intestinal lymphoid hyperplasia has been frequently noted in pediatric patients and most often associated with viral gastroenteritis. 1
Clinically, it is difficult to differentiate AA from ALH in the emergency department. 2 AA is a condition that can progress to peritonitis, and only in a few cases is it spontaneously resolved. 7 ALH is a benign nonsurgical entity that can be clinically observed and can regress if the accompanying gastrointestinal inflammation is resolved. 2
A variety of diagnostic imaging modalities can be chosen to attempt to make the appendicular diagnosis, such as ultrasonography (US), computed tomography (CT), and magnetic resonance imaging (MRI), which are important in the appendicular diagnosis.4,8 Since most of the cases are pediatric, the nonionizing imaging choice would be US. 8 Other diagnostic methods, such as CT, use ionizing radiation, and MRI requires sedation or anesthesia. The American College of Radiology’s Appropriateness Criteria for the evidence-based choice have sonography ranked lower than CT, 9 and therefore more evidence is needed to raise the ranking of this diagnostic modality choice for AA and AH.
Objectives
The objectives of this study were to describe sonographic findings of lymphoid hyperplasia of the appendix and to report demographic data on patients who were surgically operated for suspected acute appendicitis. Based on the subsequent review of the histopathology report, the diagnosis of was ALH was made.
Materials and Methods
This was a retrospective, descriptive, and observational study approved by the hospital’s institutional review board, which granted a waiver for informed consent. All the patients who had an appendicular surgery for acute appendicitis in the study institution over a 15-month period were selected. Based on 751 appendicular biopsy specimens, the records for patients diagnosed with acute appendicitis were reviewed.
The inclusion criteria were an abdominal US performed 24 hours prior to surgery with sonographic images recorded in the hospital computer system. A sample of 694 consecutive cases was chosen for review. Of these patient cases, all those that had a histopathological diagnosis of appendicular lymphoid hyperplasia were selected. The age and sex distribution of this group of patients were tabulated.
Two US expert radiologists analyzed and described separately the preoperative appendicular sonographic findings in the cases of ALH, using the images recorded in a PACS IMPAX (Impax RIS-AGFA Healthcare, Belgium).
The appendicular diameter, hypoechoic pseudonodular mucosal thickening, concentric parietal thickening, appendicular hyperemia, periappendiceal inflammatory changes (presence of fluid or hyperechogenicity of the periapppendiceal fat), or normal appendix were analyzed. A basic statistical analysis of the case results was performed.
Results
Based on a total of 761 appendectomies reviewed, 649 patients had an abdominal US 24 hours prior to surgery and were recorded in the hospital database.
In 25 cases the histopathological diagnosis was ALH, this corresponded to 3.8% of the total acute appendectomies (Figure 1).
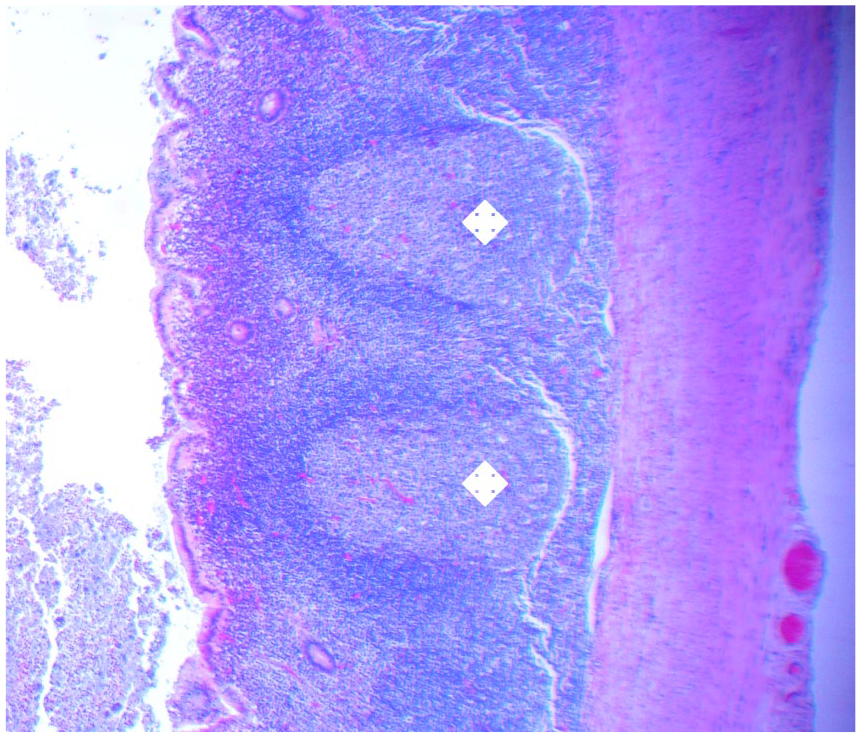
On histology, the prominent lymphoid nodules (label) were located in the lamina propria.
The sex distribution across the 25 ALH cases was 10 females and 15 males. The age distribution across the group was from 4 to 41 years, with an average of 13 years. In this cohort, 68% of the patients under 15 years old. In addition, 36% were under 10 years old, 32% were 10 to 15 years old, 16% were 15 to 20 years old, and 16% were 20 to 41 years old (Figure 2).
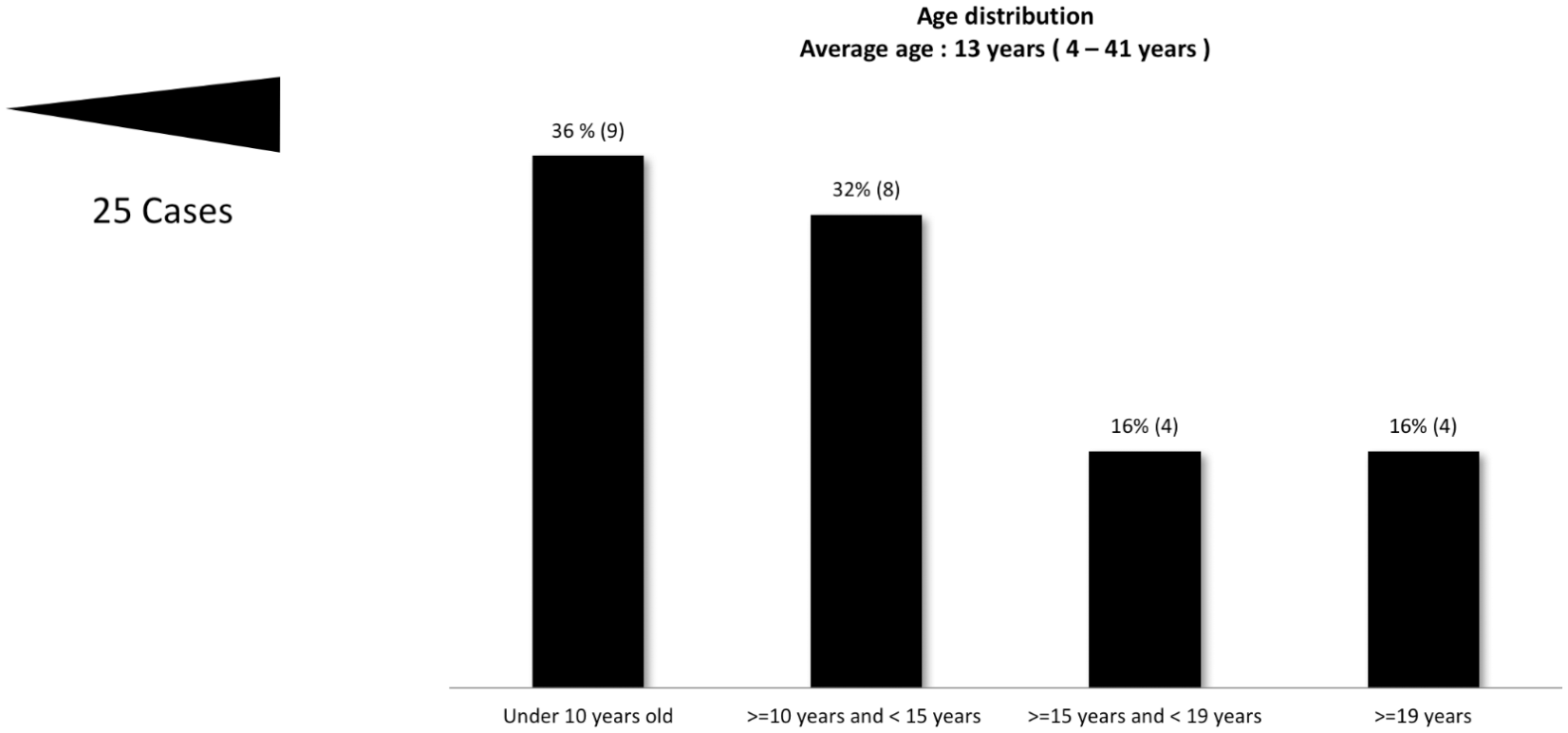
Appendicular lymphoid hyperplasia age distribution.
Based on the histological reports, 22 ALH patients had a lack of inflammation, and 3 patients had an inflammatory infiltrate.
Reviewing the US images, the appendix was visualized in 22 patients, and in 3 patients, it was not found.
In 18 cases, the sonographic reports provided a diagnosis of appendicitis, and in 4 cases, it was reported as a normal appendix.
The mean appendicular diameter was 7 mm. There were no differences in diameter between patients with ALH with or without inflammatory changes.
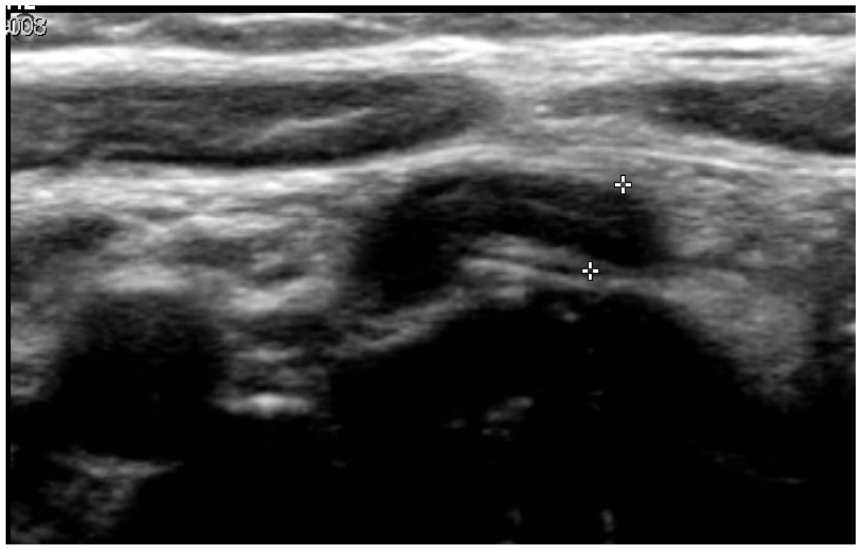
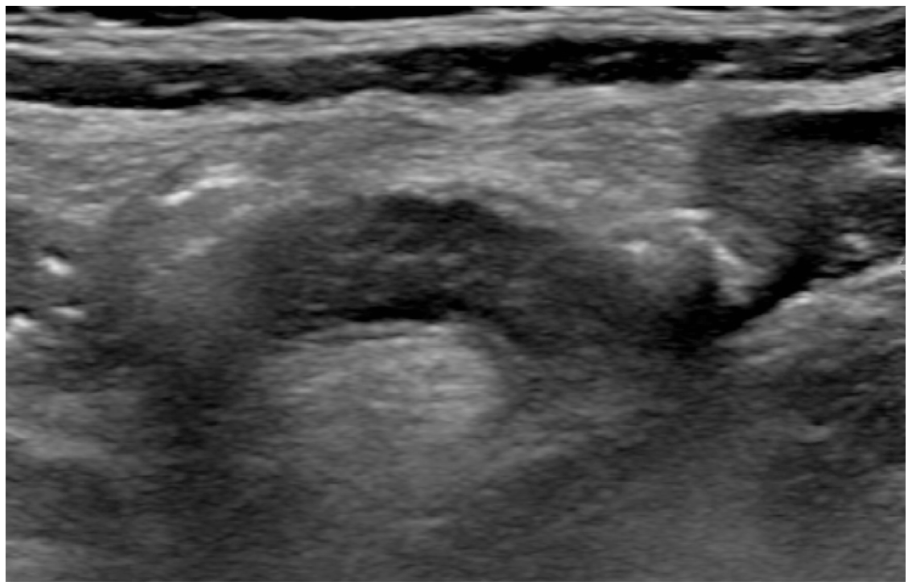
The sonographic analyzed findings were 18 cases with increased appendicular diameter (more than 5 mm) (82%) (Figure 3), 11 cases with hypoechoic pseudonodular mucosal thickening (50%) (Figures 4 and 5), 3 cases with concentric parietal thickening (13%) (Figure 6), 1 case of appendicular hyperemia (4.5%) (Figure 7), and 4 cases with periappendiceal inflammatory changes (18%) (Figure 8). In this cohort, 4 cases had a normal appendix on US, 2 with intestinal intussusception (9%).
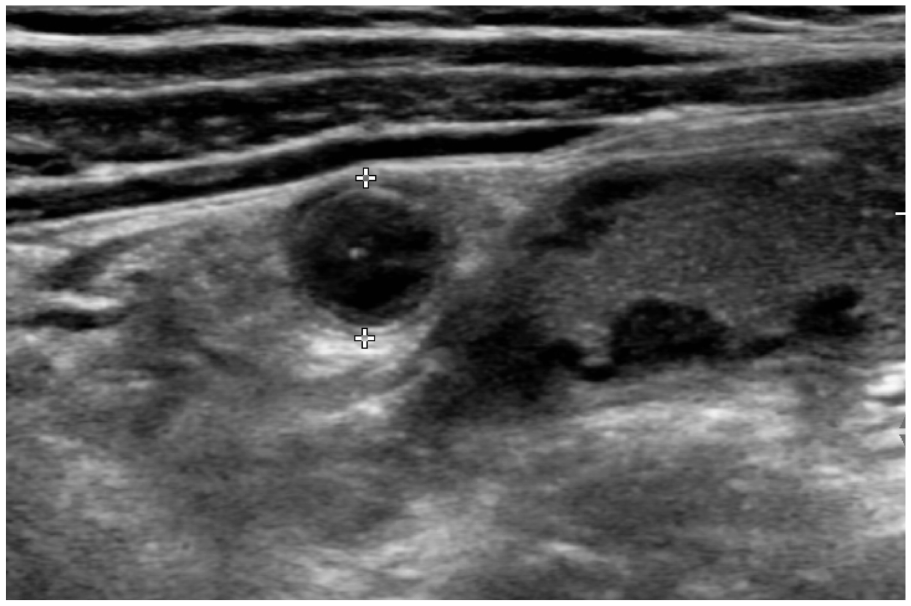
Transverse ultrasound image. An enlarged noncompressible vermiform appendix (structure with the caliper) with hypoechoic pseudonodular mucosa thickening and thin lumen. The adjacent ileum shows signs of intestinal lymphoid hyperplasia.
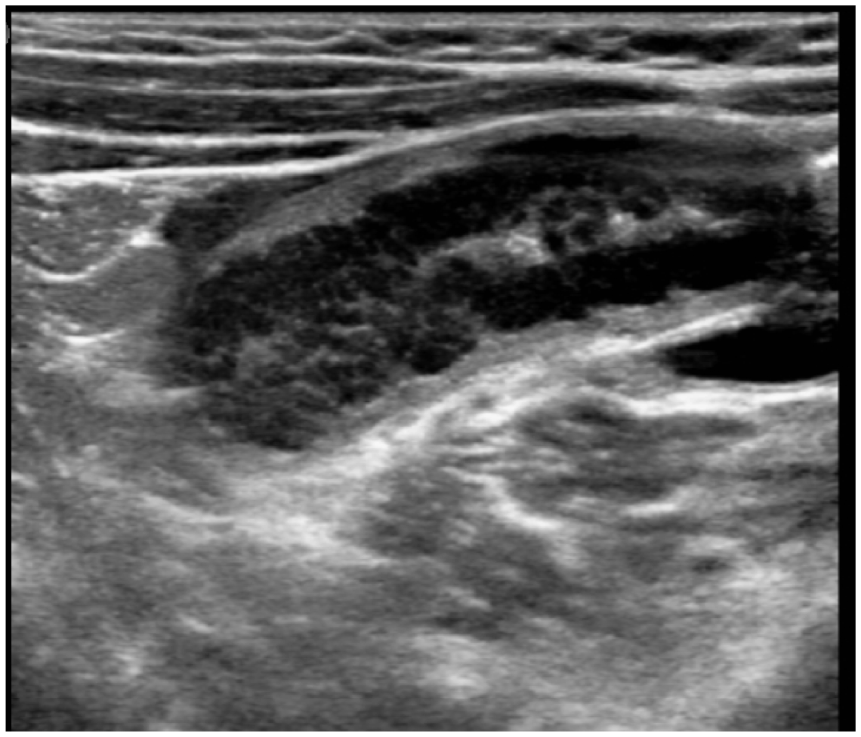
Longitudinal ultrasound appendicular images. Enlarged appendicular diameter and hypoechoic pseudonodular mucosa thickening.
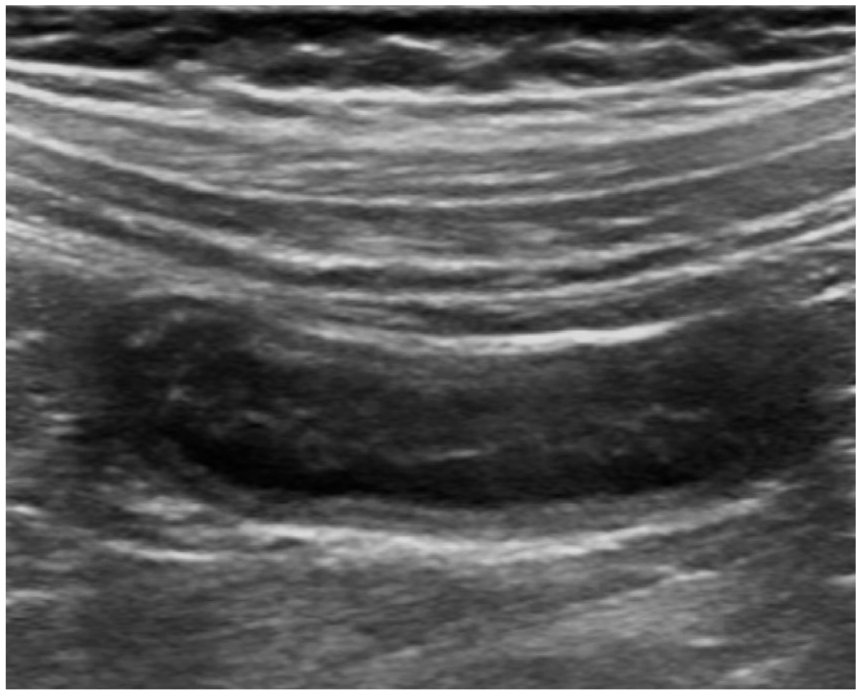
Longitudinal US image with an enlarged appendix and hypoechogenic pseudonodular mucosa thickening.
Longitudinal appendicular ultrasound. Appendix with concentric parietal thickening.
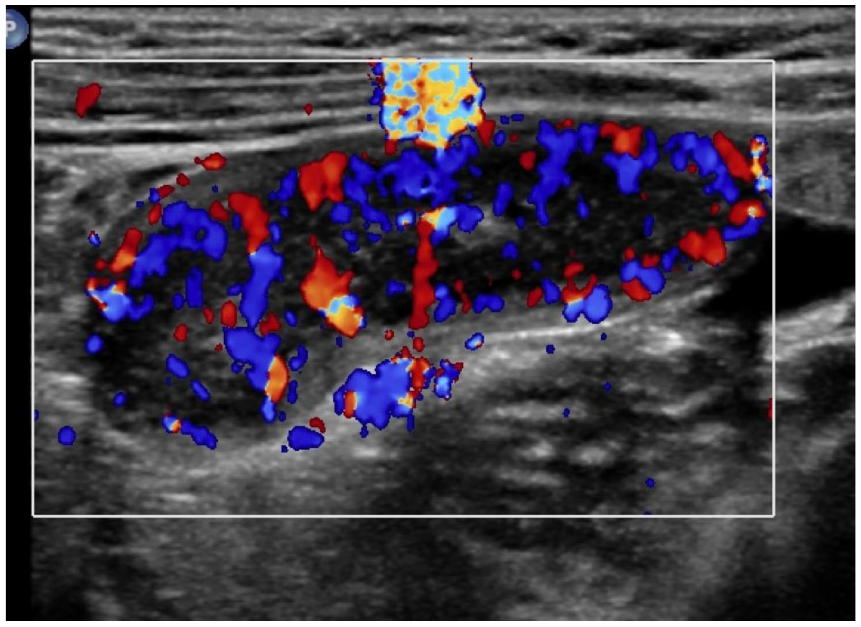
Longitudinal image with color Doppler shows marked appendicular wall hyperemia.
Longitudinal ultrasound image of the appendix, increased in diameter with thickened wall and inflammatory changes of the surrounding tissue.
Discussion
ALH corresponds to a benign reversible enlargement of the lymphatic tissue of the appendix wall, secondary to stimulation, especially for viral or bacterial infections, giardiasis, IgA deficiency, or cow milk protein allergy. 5
ALH is an infrequent condition based on the enlargement of the lymphoid follicles in the appendicular mucosae, without polimorfonuclear infiltrate.5,6 It can also present in the ileocecal region, rectum, and occasionally the colon and duodenum. 5 ALH produces an alteration in the intestinal motility that can cause pain and predispose to intussusception. 3
Acute appendicitis is one of the most frequent causes of acute abdominal pain, especially in the young population, and frequently is an emergency surgery indication.2–4 The incidence in developed countries is 90 to 100/100 000 inhabitants per year and most frequently in the second and third decades of life. 4
The obstruction of the appendicular lumen can produce AA.1,2 ALH is considered one of the risk factors for appendicular lumen obstruction in pediatric patients. 1 Also, the presence of coprolites, thick mucus, or impacted stool is included for luminal obstruction. 4 The presence of coprolites and HLA is less common. 10
The imaging evaluation of the appendix can be performed with US, CT, or MRI.8,9 Based on varied meta-analyses, the proper diagnostic choice could be controversial. In many cases, the physician may choose an imaging modality solely based local experience. 11 Making the diagnosis of AA, US and CT have sensitivity and specificity values higher than 90%, with negative and positive predictive values higher than 95%, which rival a physical examination. 3 US imaging techniques do not employ ionizing radiation or anesthesia but do permit the differentiation of bowel wall layers. 1
The appendicular US findings described are parietal thickness or a nodular hypoechoic inner band with reduction in the appendicular lumen. 1 This wall alteration can be observed in another intestinal segment. 1 ALH may result in a 6- to 8-mm noncompressible appendix that could be misdiagnosed as appendicitis in pediatric patients. 1 For a true-positive diagnosis of appendicitis, the presence of inflammatory signs should include at least two of the following: periappendiceal fluid, hyperechoic periappendiceal fat, or mural hyperemia to increase diagnostic accuracy. 1
This cohort study would suggest that ALH has a low incidence out of the total AA surgeries (3.8%) and is frequent in the younger population (84% of the patients under 20 years). The mean appendicular diameter was 7 mm. In this cohort, the sonographic findings were an increased appendicular diameter (82%), hypoechoic pseudonodular mucosal thickening (50%), concentric parietal thickening (13%), appendicular hyperemia (4.5%), periappendiceal inflammatory changes (18%), and associated intestinal intussusception (9%). The US documentation of inflammatory changes was less frequently noted. Hypoechoic pseudonodular mucosal thickening was the only finding that could not be described in the cohort of patients with AA.
Conclusion
ALH is a benign condition that is more frequent in the pediatric population, and it can predispose patients to appendicular appendicitis. Both pathologies can increase the appendiceal diameter. This cohort review would suggest that in pediatric patients, ALH could be considered when the following features are present: hypoechogenic pseudonodular appendicular mucosal thickening and the absence of periappendiceal inflammatory changes. It is important to recognize these two different entities as they have a different pathological evolution. It is highly suggested that clinical and diagnostic imaging studies are important follow-up steps.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.